
Abstract
Background:
Infections following orthopedic procedures, such as implant insertion, are common and pose significant burdens globally. Comprehensive evidence of its prevalence and the influencing factors is crucial for developing effective infection prevention strategies across regions.
Objective:
To assess the prevalence of infection and associated factors after Surgical Implant Generation Network nailing in African countries with the Surgical Implant Generation Network program.
Method:
A comprehensive search was performed across multiple databases, including PubMed, Global Index Medicus, Scopus, Embase, Science Direct, Hinari, and African Journals Online, complemented by a search of Google Scholar. After data extraction, the data were exported to STATA 17 statistical software for analysis. The pooled prevalence of infection was estimated using a random effects model. The level of heterogeneity was assessed using the I² test, while publication bias was evaluated through a funnel plot and Egger’s and Begg’s tests.
Results:
This meta-analysis included 23 full-text studies involving a total of 4266 patients treated with Surgical Implant Generation Network intramedullary nailing for long bone fractures. The pooled prevalence of infection was 5.69% (95% CI: 4.55%–6.83%), with a moderate level of heterogeneity (I² = 57.86%, p < 0.001). The review also identified significant predictors of infection, including open fracture type, complex fracture patterns, surgery performed within 15 days of injury, the presence of a prophylactic drain, female gender, and procedures conducted by junior surgeons.
Conclusion:
This meta-analysis revealed a relatively high infection prevalence in patients who underwent Surgical Implant Generation Network nailing for fractures. Infection risk was significantly higher in cases involving open or complex fractures, early surgical intervention, use of prophylactic drains, female patients, and procedures conducted by less-experienced surgeons. To mitigate this burden, clinical efforts should focus on optimizing the timing of surgery, avoiding unnecessary drain placement, strengthening supervision for junior surgeons, and prioritizing enhanced intraoperative and postoperative care for high-risk fracture types.
Background
Fractures are a growing global health concern, with 455 million cases reported in 2019, a 70.1% increase since 1990. They cause significant morbidity and mortality due to complications such as infections. 1 Fractures are often managed with various implants, with intramedullary nailing being a common technique, especially for long bone fractures. 2
In resource-limited settings, the Surgical Implant Generation Network (SIGN) nails are particularly common among intramedullary nails. These nails are supplied by the SIGN program to ensure affordable and effective orthopedic care. 3 The SIGN is an initiative aimed at improving access to orthopedic surgical care in low- and middle-income countries (LMICs). The SIGN provides relevant training to orthopedic surgeons and supplies affordable and effective surgical implants that are specifically designed for long-bone fracture fixation in resource-limited environments. In addition to supplying hardware and providing training, the SIGN initiative promotes the use of standardized surgical techniques to enhance outcomes and reduce complications, including infections. The SIGN nail has been utilized in more than 437,086 patients across 58 developing countries.3,4
Alongside the efforts of the SIGN, the World Health Organization (WHO) has developed initiatives aimed at enhancing surgical safety and reducing postoperative complications. One notable intervention is the WHO Surgical Safety Checklist, which has been adopted by many LMICs and includes key components to minimize the risk of surgical site infections (SSIs).5,6 Additionally, the WHO developed global guidelines for the prevention of SSIs to support standardized practices worldwide. 7 Despite these important efforts, the consistent implementation of infection prevention strategies in LMICs remains hindered by limited resources, inadequate infrastructure, and variability in surgical training and expertise.8,9
Infections are among the most common complications following orthopedic procedures, such as implant insertions. The risk of infection in patients undergoing internal fixation can range from 0.4% to 16.1%, and this risk is influenced by factors such as the type of fracture (whether it is closed or involves varying degrees of soft tissue injury). 10 Large-scale studies on SIGN nailing have reported infection rates ranging from 1% to 11.9%.3,11–13
The occurrence of infection is associated with various patient and surgery-related factors such as advanced age, comorbidities, cognitive impairment, smoking, longer procedure duration, higher grade Gustilo–Anderson open fracture (OF) type, and intraoperative complications. These factors increase the risk of SSIs in orthopedic procedures.11,12,14–16
Although infections are preventable, they continue to have a significant impact on patients and healthcare systems worldwide. They not only increase patient morbidity and mortality rates but also result in additional costs.17–19 For instance, a study in the United States revealed that the median cost of treating operated patients with SSIs was $108,782, whereas patients without infections incurred costs of $57,418. 19 In LMICs, the additional cost of treating SSIs can range from $174 to $29,610. 20 Compared with patients who were not infected, patients with SSIs had longer hospital stays by 7–11 days. Additionally, there has been an increase in readmissions and the need for additional surgeries.21,22
Understanding the prevalence rate of infection after SIGN nailing and its predictors is crucial for reducing poor outcomes after surgery. While studies have been conducted in various countries, there is a lack of comprehensive and updated evidence specifically addressing infection prevalences and associated factors in Africa. Therefore, this study aimed to assess the pooled prevalence and associated factors of infection after SIGN nailing in Africa, focusing on countries where the SIGN program has been implemented. This aggregation of data is crucial for developing effective infection prevention strategies tailored to regional needs.
Methods
Protocol and registration
This review was conducted following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 guidelines. 23 A completed PRISMA checklist is provided in the Supplementary File 1. The protocol for this systematic review and meta-analysis was not preregistered.
Data sources
The data sources used in this study included several electronic databases, such as PubMed, Global Index Medicus, Embase, Scopus, ScienceDirect, Hinari, and African Journals Online. In addition, Google Scholar was accessed, and the institutional repositories of various Ethiopian universities were reviewed. To ensure comprehensive coverage, a manual search of the reference lists of the included articles was conducted. The search period for this review was from June 2 to 21, 2024.
Search strategy and selection criteria
The search strategy was developed using the CoCoPop framework. 24 Co (Condition) included terms related to infection, Co (Context) focused on African countries with the SIGN program, and Pop (Population) covered different terms related to patients treated with SIGN nailing. For context, the names of each of the 30 African countries with the SIGN program were included. 25 The search strategy employed various techniques, including truncation (*), Boolean operators (“OR” and “AND”), and phrase searching (“. . .”). Additionally, MeSH terms were utilized in PubMed, Emtree terms in Embase, and relevant synonyms to ensure a comprehensive search. The details of search strategy is presented and provided (Supplementary File 2).
Inclusion and exclusion criteria
This review included studies published in English that reported the prevalence of infection (both superficial and deep) and/or factors associated with infections in patients with long bone fractures who underwent SIGN nailing. There were no restrictions on the study period, and articles accessible through our search sources between June 2 and 21, 2024, were included. Articles lacking abstracts or full texts, anonymous reports, editorials, case reports, studies without clear outcome reporting, and qualitative studies were excluded.
Data abstraction procedure and quality assessment
Initially, references from the searched databases were imported into EndNote software (Clarivate, Philadelphia, PA, USA) to remove duplicates and prepare the references for further processing. Two authors (D.E. and T.F.A.) then independently reviewed and screened titles and abstracts based on predefined criteria. After this, full-text articles were retrieved and reviewed independently by both authors. Any discrepancies in selection were resolved through discussion with a third author (O.A.).
The quality of the studies was assessed using the Newcastle‒Ottawa Scale (NOS). 26 Originally designed to evaluate cohort and case–control studies, the NOS was also adapted for cross-sectional studies. 27 The scale assesses three categories: selection of study groups, comparability of groups, and ascertainment of outcomes or exposures. For cross-sectional studies, a total of seven items were used, while for cohort studies, eight items were used. Each study is rated on a star system, with a maximum of nine stars indicating the highest quality. Two authors (D.E. and E.K.B.) independently evaluated each study using this tool. Finally, only studies with an average score of 6 or higher were included in the final analysis. 28
Outcome measurement
The first outcome of this review focused on the prevalence of SSIs following SIGN intramedullary nailing. SSI was defined as any infection occurring at or near the surgical incision within 1 year, encompassing superficial, deep incisional, and organ/space infections. 7
The second outcome was the identification of factors associated with infection among patients who underwent SIGN intramedullary nailing. This was assessed using adjusted odds ratios (aORs). A variable was considered a significant risk factor if it demonstrated a statistically significant association with infection in the multivariable analysis of included studies (p < 0.05 or if the aOR did not include 1).
Data extraction and analysis
Using the Joanna Briggs Institute data-extraction form as a template, 29 the data extraction format was prepared using Excel 2013 software (Microsoft Corp., Redmond, WA). The format consisted of the author(s) name, publication year, country, region, study design, sampling technique, sample size, participant’s age group, proportion of open type of fracture, description of inclusion and exclusion criteria, prevalence of infection, and the aOR with its 95% CI of selected predictors of infection.
After extraction, the data were exported to STATA version 17 (Stata Corp, College Station, TX, USA) for meta-analysis. Given the moderate heterogeneity observed (I² = 57.8%), a random-effects model using the DerSimonian–Laird method was employed to estimate the pooled prevalence of infection. 30 Heterogeneity was assessed with the I2 statistic, where values of 40%, 60%, and 90% indicated low, moderate, and substantial heterogeneity, respectively. 31 Due to the observed heterogeneity, subgroup analyses were performed based on the study region, study design, participant age group, and proportion of patients with OFs.
Publication bias was examined with funnel plots to assess symmetry subjectively, and Begg’s and Egger’s regression tests were used for objective assessment. 32 The significant results from these tests warranted trim and fill analyses. Leave-one-out sensitivity analysis was conducted to evaluate the influence of individual studies on the pooled infection estimate. Finally, the results were presented using text, tables, and various plots.
Results
Search results
The electronic search yielded 842 articles from various sources. From these, 276 duplicate articles were removed. Out of the remaining 566 articles, 521 unrelated articles were excluded after a thorough evaluation of their title and abstract, leaving 45 articles for further consideration. However, three articles could not be retrieved due to a lack of full-text availability. Consequently, 42 full-text articles were thoroughly assessed based on the inclusion criteria. After a full-text review, 19 articles were excluded for various reasons: two studies did not clearly report results,33,34 16 were outside the predefined study region,17,35–49 and one study focused on patients treated with intramedullary nailing methods other than SIGN. 50 Finally, 23 studies were included in the meta-analysis.51–73 The details are presented in the PRISMA flow diagram (Figure 1).
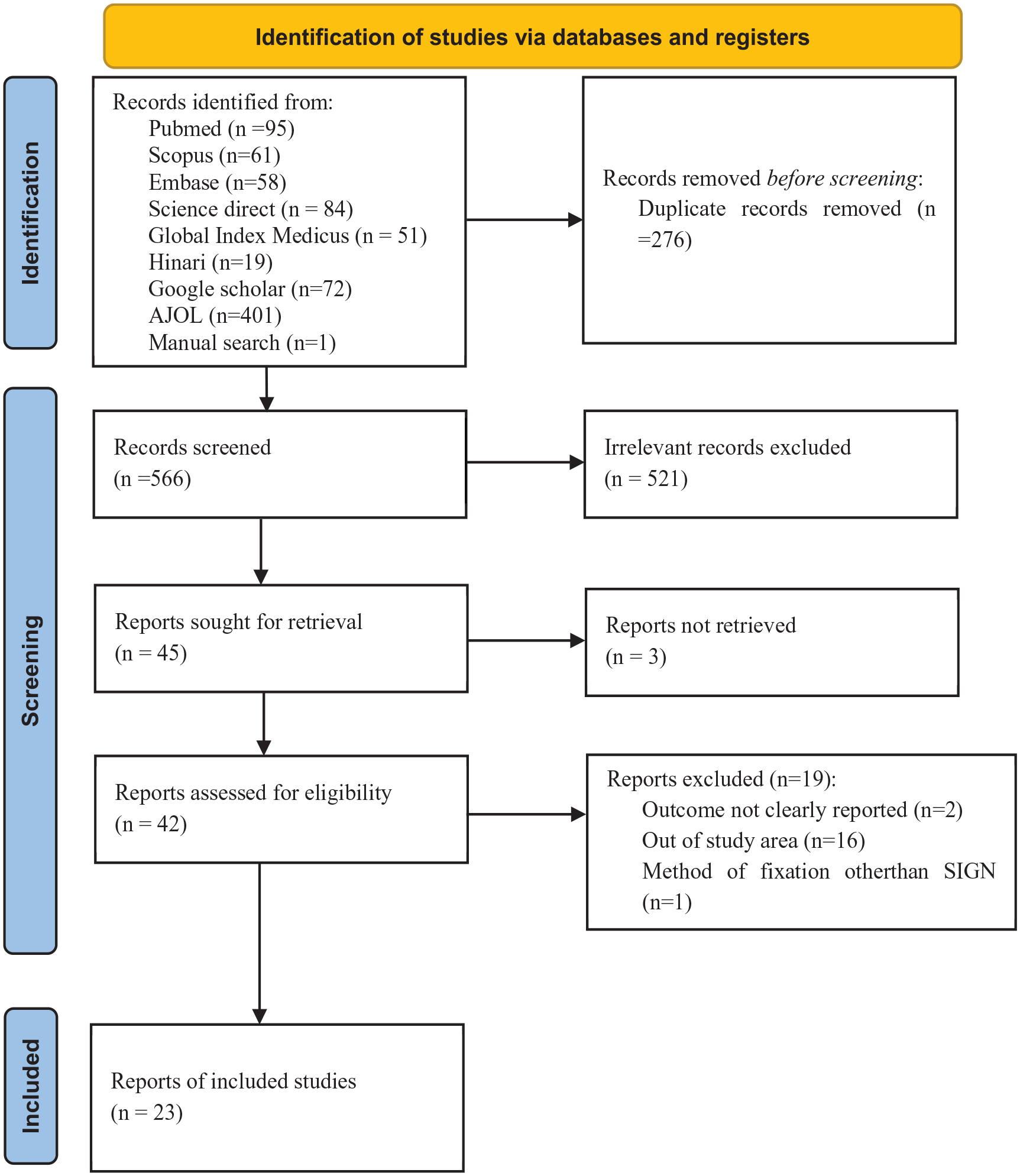
Flowchart of a selection of studies for a systematic review and meta-analysis of infection prevalence after intramedullary nailing in African countries with the SIGN program, 2024 (n = 23). 23
Characteristics of the reviewed studies
This meta-analysis included a total of 23 studies published between 2007 and 2023. These studies involved a cumulative sample size of 4266 patients who had fractures and were treated with the SIGN intramedullary nail. Of the included studies, 13 used a cross-sectional design, nine used a cohort approach, and one was a randomized controlled trial. The majority of the studies (15 in total) were conducted in Ethiopia and Nigeria. Additionally, there were four studies from Tanzania and one each from Kenya, Malawi, Uganda, and Zimbabwe (Table 1).
Descriptive summary of 23 studies included in the meta-analysis of the infection prevalence after intramedullary nailing in African countries with the SIGN program, 2024.

AIDS: acquired immunodeficiency syndrome; AO: Arbeitsgemeinschaft für Osteosynthesefragen (German for “Association for the Study of Internal Fixation”); CS: cross-sectional; GCS: Glasgow Coma Scale; GA: Gustilo–Anderson; HIV: human immunodeficiency virus; IM: intramedullary; LIMN: locked intramedullary nail; OF: open fracture; OTA: Orthopedic Trauma Association; PC: prospective cohort; RCT: randomized controlled trial; SCI: spinal cord injury; SIGN: Surgical Implant Generation Network; SSI: surgical site infection; TBI: traumatic brain injury.
Risk bias assessment for included studies
Out of the 23 studies included and evaluated using the NOS, five cohort studies received a score of 7, and the remaining five cohort studies achieved a score of 8 out of a possible 9 points. Additionally, all 13 cross-sectional studies scored between 8 and 10 out of 10 points. These results indicate that the included studies are of good quality.
Pooled prevalence of infection after SIGN nailing
Across the included studies, the infection prevalences ranged from 2.33% 69 to 15.45%. 68 The meta-analysis revealed that the pooled prevalence of infection following intramedullary SIGN nailing across African countries with the SIGN program was 5.69% (95% CI: 4.55%–6.83%), with moderate heterogeneity (I² = 57.86%, p < 0.001; Figure 2).
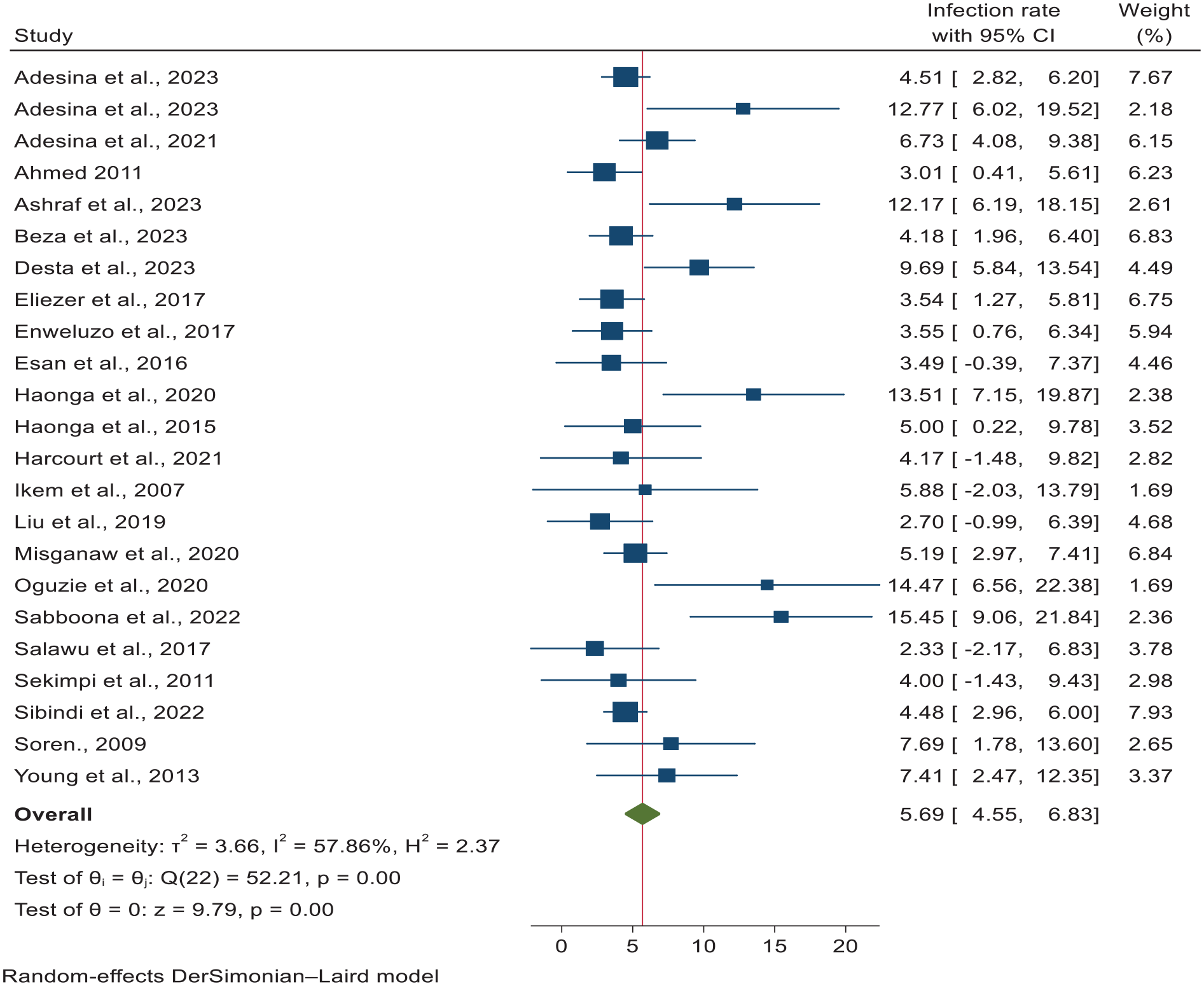
A forest plot for the pooled infection prevalence after intramedullary nailing in African countries with the SIGN program, 2024 (n = 23).
A meta-regression analysis was conducted to investigate potential factors that contributed to the heterogeneity. The analysis included variables such as region, study design, publication year, sample size, proportion of patients with OFs, and participant age group. Among these factors, the proportion of OFs showed statistical significance. Subsequently, subgroup analyses were performed based on region, study design, participant age group, and proportion of patients with OFs. Notably, studies involving patients with OFs revealed a significantly higher infection prevalence of 13.45% (95% CI: 10.27%–16.62%; Figure 3).
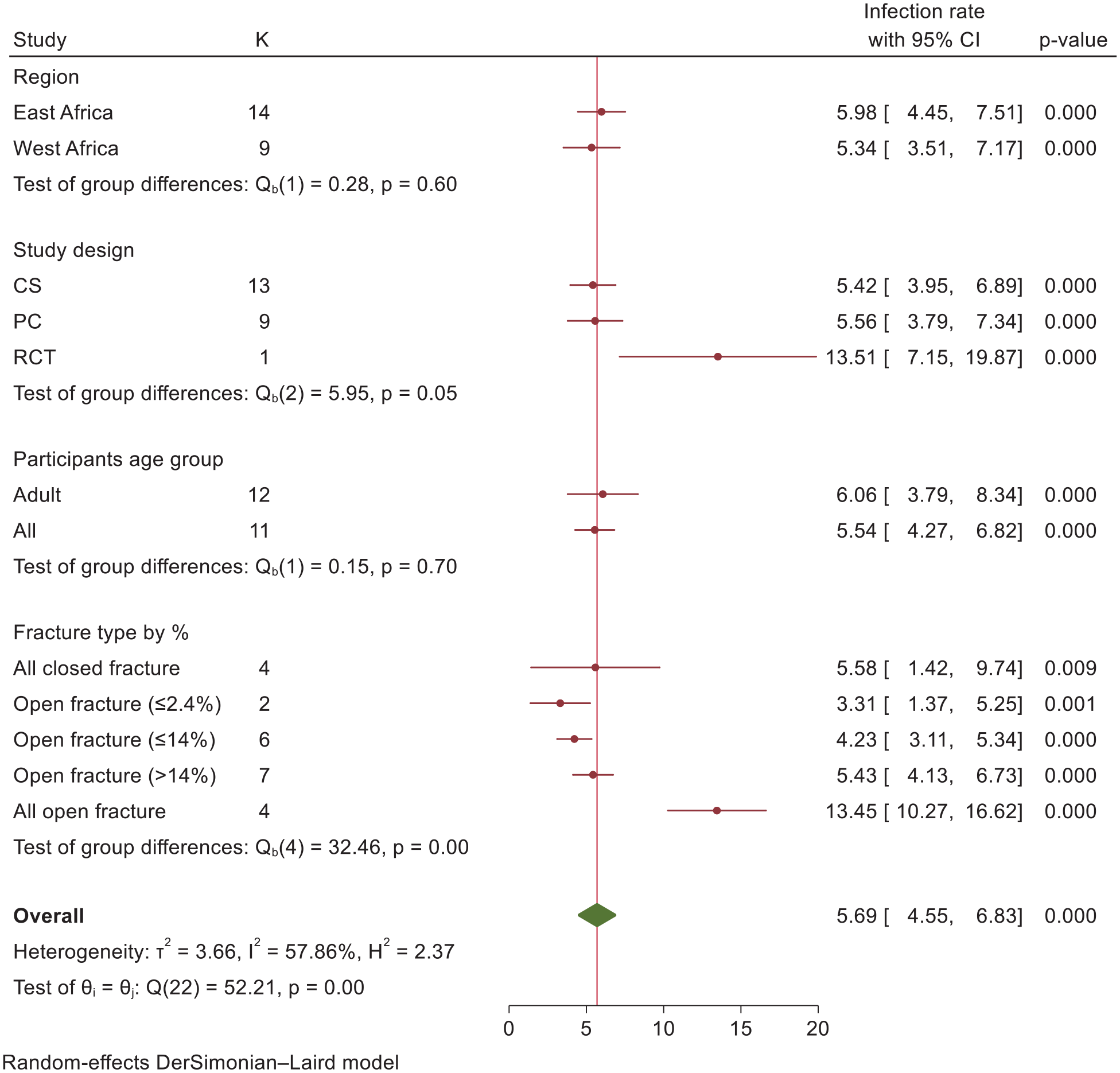
Subgroup analysis for infection prevalence after intramedullary nailing in African countries with the SIGN program, 2024 (n = 23).
Factors associated with infection after SIGN nailing
Although a thorough search was conducted, this review revealed only two studies that reported predictors associated with infection after SIGN nailing in African countries with the SIGN program.66,67 These predictors include OF type, 66 complex fracture patterns, 66 surgery within 15 days of injury, 66 the presence of a prophylactic drain, 67 female gender, 67 and procedures conducted by junior surgeons 67 (Table 2).
Predictors of infection following SIGN nailing in African countries with the SIGN program, 2024.

aOR: adjusted odds ratio; SIGN: Surgical Implant Generation Network.
Publication bias
Both the subjective and objective interpretations of the analysis indicated the presence of publication bias. The funnel plot distribution appeared to be asymmetric (Figure 4). Additionally, both Egger’s and Begg’s regression tests yielded statistically significant results (p < 0.005). Consequently, further analysis was conducted using meta-trim-and-fill methods to examine the impact of publication bias on the pooled prevalence of infection. This resulted in the imputation of four studies. However, the pooled prevalence of infection did not show a statistically significant difference after imputation, with a prevalence of 4.94% (95% CI: 3.64%–6.23%), indicating no significant effect on the pooled estimate.

Funnel plot showing the asymmetric distribution of 23 articles on infection prevalence after intramedullary nailing in African countries with the SIGN program (n = 23).
Sensitivity analysis
A leave-one-out sensitivity analysis demonstrated that the pooled infection estimates following SIGN nailing across African countries with the SIGN program remained stable regardless of the exclusion of any single study. This indicates that the results are robust and not significantly influenced by any individual study (Figure 5).

Sensitivity analysis of infection prevalence after intramedullary nailing in African countries with the SIGN program, 2024 (n = 23).
Discussion
This systematic review and meta-analysis aimed to assess the pooled infection prevalence and associated factors following SIGN intramedullary nailing in African countries with the SIGN program. The overall prevalence of infection was 5.69% (95% CI: 4.55%–6.83%). This result aligns with a previous systematic review. 13 However, our findings indicate a lower infection prevalence than that reported in a large-scale study, which reported an 11.9% infection prevalence. 12 Differences in participant inclusion criteria might explain the variations between the two studies. The current review included studies reporting infection prevalences for all types of fractures, whereas the other study focused exclusively on patients with open tibial shaft fractures. 12 The lower infection prevalence in the current review might be due to the inclusion of patients with closed fractures. The evidence consistently shows that OFs increase the risk of infection.12,66 The subgroup analysis by fracture type in the current study also confirmed that there was a greater risk associated with OFs.
In contrast, the infection prevalence observed in the current study was greater than that reported in another large-scale study. 11 This discrepancy might also be associated with differences in the clinical characteristics of the participants. In our review, 26% of individuals had OFs, compared to only 17.0% in the comparator study. This suggests that the higher prevalence of OFs in our review may have contributed to the observed higher infection prevalence.
In this review, some factors emerged as significant predictors of infection following SIGN nailing. Notably, OF types and complex fracture patterns demonstrate a heightened risk of infection, underscoring the challenges in managing such cases effectively. 66 This association stems from the compromised skin barrier in OFs, which facilitates pathogen entry, and the challenges of managing extensive tissue damage in complex fractures during surgery, which can ultimately increase infection susceptibility. These factors highlight the critical importance of meticulous wound management, prompt surgical intervention, and tailored prophylactic measures in mitigating infection risks associated with open and complex fractures.
The timing of surgery within 15 days of injury also emerged as a significant factor for increased infection prevalences. 66 This might be because patients for whom surgery was delayed 15 days or more often had clean, closed fractures or fractures with a known infection status requiring treatment before intramedullary nail insertion. Delaying surgery in these patients allows initial infection management and wound stabilization, potentially reducing the risk of postoperative infections associated with acute trauma and surgical intervention. 74
The presence of prophylactic drains has been identified as a potential risk factor for infection. 67 This can be justified by the fact that while drains are intended to prevent hematomas/seromas, 75 they can also disrupt tissue perfusion, provide a pathway for bacteria to enter the wound, and serve as a medium for bacteria to form biofilms on their surface. These biofilms can reduce the ability of leukocytes to kill bacteria.75,76 All of these factors ultimately increase the risk of infection in patients who have drains, emphasizing the importance of strict aseptic techniques, close monitoring to minimize the risk of infection, and the need for further studies. The current review also revealed that female gender is associated with a greater likelihood of infection, warranting further investigation into potential physiological or procedural factors influencing this disparity. 67
Another predictor of infection is the type of surgeon performing the procedure. Procedures performed by consultant surgeons are associated with lower infection prevalences, 67 highlighting the significance of experience in achieving positive surgical outcomes. This is because consultants are generally more experienced, perform procedures more efficiently (with a shorter duration of surgery), and have better tissue-handling skills. 76 This underscores the need for adequate training and supervision of less-experienced surgeons to improve surgical outcomes. This study has limitations. The scope was limited by excluding articles published in languages other than English, which may have affected the comprehensiveness of the review. Furthermore, due to the limited number of relevant articles, it was not possible to quantitatively pool the estimates of predictors, resulting in a qualitative review only.
Conclusion
This meta-analysis revealed a high prevalence of infection in patients who underwent SIGN nailing for fractures. The risk of postoperative infection was particularly higher in patients with OFs, complex fracture patterns, early surgical timing, the use of prophylactic drains, female gender, and procedures performed by less-experienced surgeons. These findings highlight the need for targeted infection prevention strategies in SIGN-supported settings. Specifically, careful consideration should be given to the timing of surgery, judicious use of drains, and enhanced supervision and training of junior surgeons. Moreover, patients with anatomically complex or OFs warrant closer intraoperative and postoperative monitoring to reduce the risk of infection and improve surgical outcomes.
Supplemental Material
sj-docx-1-smo-10.1177_20503121251352653 – Supplemental material for Prevalence of infection and associated factors after intramedullary nailing in African countries with the Surgical Implant Generation Network program: A systematic review and meta-analysis of available evidence
Supplemental material, sj-docx-1-smo-10.1177_20503121251352653 for Prevalence of infection and associated factors after intramedullary nailing in African countries with the Surgical Implant Generation Network program: A systematic review and meta-analysis of available evidence by Destaw Endeshaw, Natnael Kebede, Abiyu Abadi Tareke, Ousman Adal, Eyob Getachew, Asnake Gashaw Belayneh, Getnet Alemu Andargie, Kedir Seid, Gebeyehu Lakew, Amlaku Nigusie Yirsaw, Mitiku Tefera, Eyob Ketema Bogale, Tadele Fentabel Anagaw and Eneyew Talie Fenta in SAGE Open Medicine
Supplemental Material
sj-docx-2-smo-10.1177_20503121251352653 – Supplemental material for Prevalence of infection and associated factors after intramedullary nailing in African countries with the Surgical Implant Generation Network program: A systematic review and meta-analysis of available evidence
Supplemental material, sj-docx-2-smo-10.1177_20503121251352653 for Prevalence of infection and associated factors after intramedullary nailing in African countries with the Surgical Implant Generation Network program: A systematic review and meta-analysis of available evidence by Destaw Endeshaw, Natnael Kebede, Abiyu Abadi Tareke, Ousman Adal, Eyob Getachew, Asnake Gashaw Belayneh, Getnet Alemu Andargie, Kedir Seid, Gebeyehu Lakew, Amlaku Nigusie Yirsaw, Mitiku Tefera, Eyob Ketema Bogale, Tadele Fentabel Anagaw and Eneyew Talie Fenta in SAGE Open Medicine
Footnotes
ORCID iDs
Author contributions
D.E., O.A., E.K.B., N.K., E.G., A.G.B., G.A.A., and T.F.A. contributed to the study conception, literature review, and data extraction. D.E., A.N.Y., and K.S. were involved in the data management, analysis, and interpretation of the results. D.E., G.L., M.T., A.A.T., and E.T.F. participated in article preparation. All authors reviewed and approved the final article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
All data generated or analyzed during this study are included in this published article and its supplementary information files.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.