
Abstract
Introduction:
Clinically, a consensus of the treatment strategies of ACL grade 2 injury is not reached. Therefore, the present study established a proprioceptive deficit model of the ACL via an arthroscope to aid with further studying ACL grade 2 injury and treatment strategies.
Materials and Methods:
12 cynomolgus monkeys were randomly divided into the model group and the blank control group. In the model group, 1/4 of the ACL was cut under an arthroscope, whereas no intervention was performed in the blank control group. Physiological data including the maximum degree of knee flexion, the thigh circumstance and the calf circumference were measured, and the Pivot-shift, Anterior and Lachman tests were also performed. Moreover, electrophysiological data including somatosensory evoked potentials (SEPs) and motor nerve conduction velocity (MNCV) were measured. SEPs and MNCV were assessed for the latent period and amplitude.
Results:
Comparing the data before and after the surgery, in the blank control group, no significant difference was observed. In the model group, significant difference was observed in the Pivot-shift, Anterior drawer and Lachman test (p < 0.05), indicating the instability of the ACL. Moreover, the latent period of SEPs and MNCV were significantly increased (p < 0.009), whereas the amplitude of SEPs and MNCV was significantly decreased (p < 0.009), indicating a degenerated proprioception of the knee joint.
Conclusions:
Following cutting 1/4 of the ACL, the knee joint became unstable and proprioception was declined. The results indicated that the proprioceptive deficit model of the ACL was successfully established, which could promote further studying ACL injury.
Introduction
The role that anterior cruciate ligament (ACL) serves is to maintain the stability of the knee joint. 1 However, ACL injury occurs in a large proportion of the population and causes a number of movement-related issues, including increased displacement and rotation of the tibia, leading to instability of the knee joint. Proprioceptive capabilities also decline following ACL injury. 2 –5 Proprioception, a necessity for normal life, refers to the perception when part of our body is static or moving. Proprioception is generated by muscle spindle afferents, mechanoreceptors in joint capsules and cutaneous tactile receptors, and is composed of limb position sense and limb movement sense. 6,7
According to the severity, ACL injury is commonly classified as grade 1, 2 or 3, and this classification is recognized by American Academy of Orthopaedic Surgeons (AAOS). Grade 1 injury, also called mild injury, means the ligament has been slightly stretched without joint instability. Grade 2 injury, also called moderate injury, refers to a partial tear. And grade 3 injury is also called severe injury and means a complete rupture of the ACL. In this grade, the knee joint becomes fully unstable. If the patient only displays a mild ACL injury and all other structures of the knee are intact, and the stability of the knee joint can be ensured, conservative treatment is recommended. By contrast, if the ACL suffers from severe injury and is completely ruptured, it becomes unable to control knee movement, which means the stability of the knee joint is heavily affected. Ligament reconstruction is the conventional treatment strategy on this grade of injury, and a majority of studies have reported better functional outcomes of ligament reconstruction on this grade of injury than conservative treatment. 8
However, there are still debates concerning strategies to cure moderate injury of the ACL. To date, there is no consensus on whether conservative treatment or ligament reconstruction is superior, and for those who choose ligament reconstruction, the surgery is technical demanding and requires a good knowledge of knee anatomy. 9 Furthermore, options of reconstruction patterns are varied and also under discussion. 10 –12 Those situations increase the difficulty of treating this grade of ACL injury and restore the proprioception of patient.
Therefore, the development of a proprioceptive deficit model of the ACL, which can simulate human ACL injury, is important for studying ACL moderate injury and help patients to restore their proprioception. A number of animal models have been established and used in previous studies, 13 –19 but the majority are not suitable for related research. For example, certain small animals require less time to establish the model, but are associated with increased surgical and postoperative care due to the small body size, which can ultimately result in infection or death. For other big animals used in research that have a larger sized knee joint, expanding the visible field during surgery would cost more, and require increased modeling and rehabilitation time.
Therefore, increasing attention has been applied to primates, as they display the closest relationship with humans. 20 Among them, cynomolgus monkeys are one of the most suitable models due to their high genetic similarity, and similar anatomies and physiologies to humans. 21 Besides, cynomologus monkeys stand and walk only on their hind limbs, and because of their nature, they stand and walk longer than the aforementioned animals, hence sharing higher similarities with humans in the aspects of standing and walking. Moreover, cynomologus monkeys display more signs of instability after ACL injury compared with animals that stand and walk on four limbs.
In general, the two physiological traits allow the knee of cynomolgus monkeys to replace the knee of humans, and the ACL injury model of cynomolgus monkeys to replace that of humans. As a result, cynomologus monkey is the most suitable model currently available.
Previous studies often developed animal models of ACL injury via open surgery, risking blood loss and trauma to the animal. Moreover, common injuries are not only to the ACL, but also to soft tissues and anatomic structures around the knee, which was different to natural injury occurring during daily life and may result in negative effects on the subsequent experiments involving the structures around the knee joint. Therefore, the present study improved the method, using an arthroscope small enough to operate in the knee joint. In summary, the purpose of the present study was to develop a proprioceptive deficit model of the ACL using cynomolgus monkeys via arthroscopic techniques, which simulated human moderate ACL injury and may serve as a suitable model for related studies.
Materials and methods
Experimental animal and feeding
Previous studies suggested that primates, such as cynomolgus monkeys, were the most suitable model in ACL injury experiments. 21 Therefore, in the present study we select cynomolgus monkeys to develop the ACL moderate injury model. Cynomologus monkeys were selected for three main reasons: (i) their knee structure shares many similarities with humans, including the ACL, the PCL, the meniscus and the articular cartilage; (ii) they stand and walk only on their hind limbs, which was more similar to humans than other animals, meaning the sign of the unstable knee joint was more distinct; and (iii) arthroscopy was used to operate on the monkeys as the articular cavity of the monkey was large enough to insert an arthroscopic lens. During the procedure, all monkeys remained healthy without infection, indicating a strong immune system of the monkey. As an infected subject can affect the process and even lead to a decreased success rate, this was a further reason for the selection of cynomolgus monkeys. 12 male, specific pathogen-free cynomolgus monkeys (age, 4.4–4.7 years; weight, 6.50–6.72 kg) were purchased from Yunnan Yinmore Bio-Tech., Ltd. and housed in several solid cages at its laboratory primate breeding center (SYXK2009-0003). All procedures were approved by the Ethical Inspection Committee of Animal Experiments of Yunnan Yinmore Bio-Tech., Ltd. (number YBT1602). The monkeys received care in accordance with the “Principles of laboratory animal care” (NIH publication No. 86-23, revised 1985) and the Association for Assessment and Accreditation of Laboratory Animal Care.
Grouping and modeling
Previous experiments also suggested that the most appropriate sample size was n = 6 per group. 22 Therefore, the following two groups were established in the present study (n = 6 per group): The model group and the blank control group. The monkeys in the blank control group were kept in the cages all the time and did not receive any intervention. Unilateral knee surgery was performed in the model group to injure a random side of the knee joint.
Prior to surgery, the arthroscopic instruments and other equipment went through strict disinfection. Subsequently, Zoletil 50 (Virbac, France; 5 mg/kg) was administered intramuscularly to anesthetize monkeys, which were then placed in supine position. After tourniquets were prepared, the hair of surgical area was trimmed and the incision was marked, the surgery began. Firstly, saline was injected into the knee cavity to dilate it (Figure 1(a)). Subsequently, the knee cavity was cut at the marked incision to establish lateral and anterior medial approaches to the knee joint, which were then used to explore the knee joint (Figure 1(b)). The ACL, the PCL, the meniscus and the articular cartilage were all confirmed as intact using an arthroscope (Figure 2(a)). Subsequently, 1/4 of the ACL was transversely cut under an arthroscope to simulate grade 2 injury of the ACL (Figure 2(b)). Finally, the incision was stitched with 3-0 absorbable sutures. All processes were performed by the same doctors. Levofloxacin hydrochloride and sodium chloride injection (Qidu Pharmaceutical Co. Ltd., China; 8 mg/kg, one dose/12 h) was administered intravenously in the following 3 days for infection prevention, and tramadol hydrochloride injection (Grunenthal GmbH, Germany; 2 mg/kg, one dose/day) was administered intramuscularly to relieve pain. In the following 2 weeks, soft padded bandages were wrapped around the operated limbs.
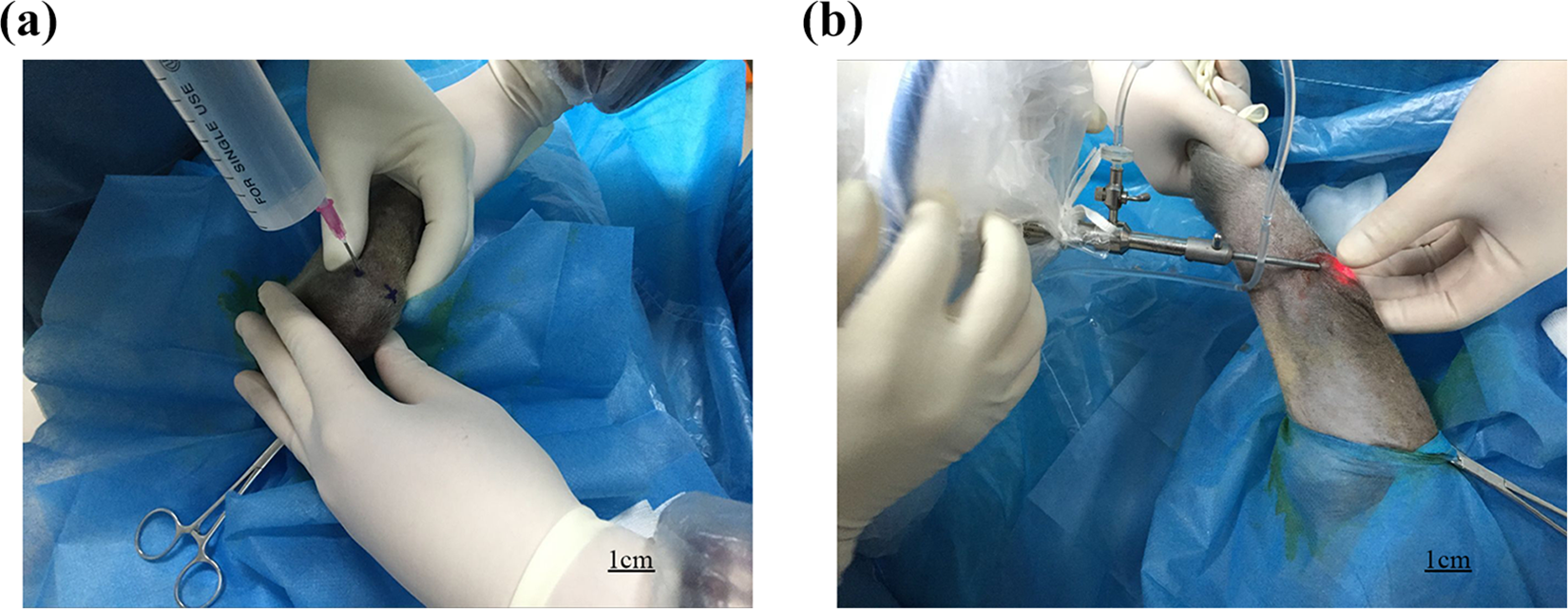
The surgical process. (a) Injecting saline into the knee cavity to dilate it. (b) Establishing lateral and anterior medial approaches to the knee joint via arthroscopy to detect the knee joint.

The operations under arthroscopy. (a) The vision under arthroscopy before cutting ACL. All tissues especially the ACL were verified intact. (b) The injured ACL after cutting one-quarter of it.
Physiology
After 2 weeks of healing post-surgery, the following physiological data were measured and three tests were performed on all monkeys. The same measurements and tests were also performed prior to the surgery on all monkeys. The measurements of the control group were performed in the same side as the modeling group. All operations were performed while the monkeys were anaesthetized and were conducted by the same orthopedist.
First, the maximum degree of knee flexion was measured (Figure 3(a)). After ACL transection, the knee flexion will be affected due to abnormal joint motions, scar tissue formation and changes in knee mobility, and the measurement can help to observe alterations to knee joint movement before and after surgery. The monkeys that underwent anesthesia were maintained in supine position, and the knee joints were flexed in the maximal degree to allow for the measurement to be taken.
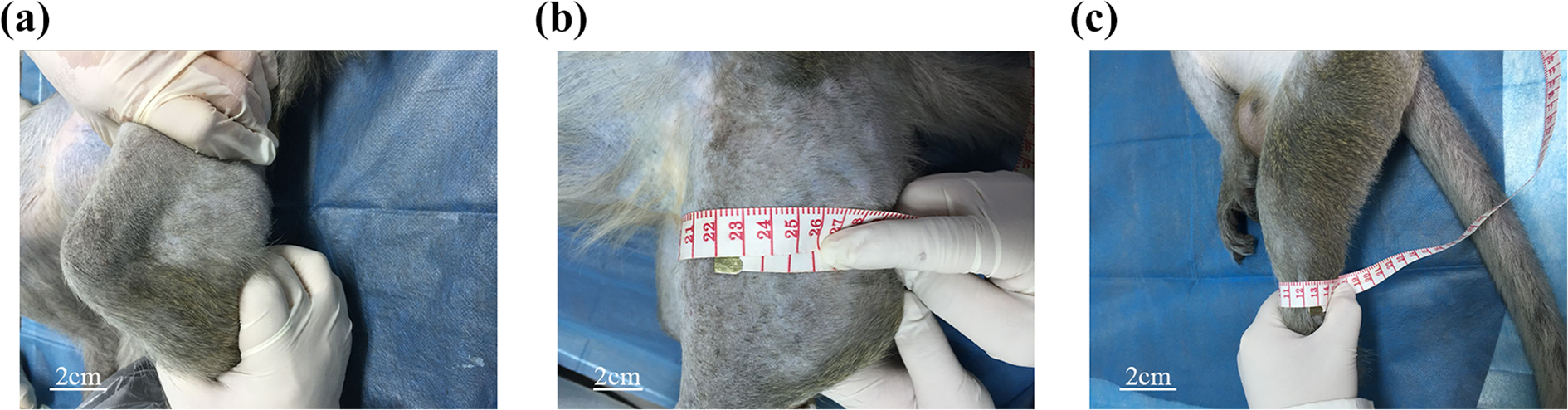
The measurements of physiological data. (a) Measuring the maximum degree of knee flexion. (b) Measuring the thigh. (c) Measuring the calf.
Subsequently, the thigh and the calf circumference were measured (Figure 3(b) and (c)), which suggested the atrophy degree of the muscle after surgery. Monkeys have shorter thighs than humans; therefore, the thigh circumference was measured at the location of 5 cm above the patella, higher than the location of human measurement by ∼5 cm. The calf circumference was measured at the location of the thickest part of the calf.
In addition, the Pivot-shift test was conducted (Figure 4(a)). Anaesthetized monkeys were positioned with the knee joints fully extended. The proximal side of the calf was grasped by one hand of the examiner, and the foot was hold by another hand to rotate the calf. Then the leg was gradually moved from extension to flexion. Tibia subluxation indicated a positive result when the knee was flexed in the range of 30 to 40 degrees, showing the instability of the knee joint.

The performance of three tests. (a) Performing the Pivot-shift test. (b) Performing the Anterior drawer test. (c) Performing the Lachman test.
In addition, the Anterior drawer test was performed (Figure 4(b)). To perform this test, the hips of anaesthetized monkeys with spine position were brought to 45 degrees and the knees were brought to 90 degrees of flexion, so that the feet were flat on the table. The examiner, standing in front of the involved knee, grasped the tibia below the knee joint line and moved the tibia anteriorly, and the movement was scored as follows: (−), bilateral tibias move forward equally; (1+), injured tibia moves further than the healthy tibia and the tibia moves <5 mm; (2+), tibia moves 5–10 mm; and (3+), tibia moves >10 mm. (−) indicated that the involved knee was stable, whereas the other scores indicated the opposite results, and higher scores indicated higher instability.
Finally, the Lachman test was performed (Figure 4(c)). The knees of anaesthetized monkeys with spine position were fixed at 15 degrees. Then the examiner griped the tibia and the thigh, and pulled the tibia anteriorly. Increased forward translation and the lack of a firm endpoint indicated a positive result, and the scoring criteria of the translation was in accordance with it of the Anterior drawer test.
Nerve electrophysiology
Alterations to ACL nerves in the model group were detected after 2 weeks of healing and simultaneously with the aforementioned postoperative measurements and tests. ACL nerves were assessed via electrophysiology, including somatosensory evoked potentials (SEPs) and motor nerve conduction velocity (MNCV). MNCV and SEPs were assessed for the latent period and amplitude. Those assessments are methods to reflect the activity of the proprioceptive fibers and test the proprioception, and extended latent period and decreased amplitude indicated nerve injury and proprioception decline.
The monkeys in the model group underwent nerve electrophysiology assessments at room temperature (26°C) three times, once a month. For comparison, the monkeys in the blank control group also underwent nerve electrophysiology once.
To measure SEPs, the corresponding bilateral skin of the ACL, which was attached to the bipolar surface electrode, was stimulated. The stimulative parameter was constant voltage (single-phrase square wave electrical stimulation; pulse width, 0.1 ms; intensity, 15–20 mA). The SEPs of the monkeys were recorded using a photoelectric evoked potentiometer (MEB-9402C), and the graphics latent period and amplitude indexes of SEPs were measured and analyzed.
To measure MNCV, three electrodes were used. The popliteal fossa was connected to the stimulating electrode, the muscle belly of the hamstring was connected to the recording electrode, and the reference electrode was at the recording electrode by 2 cm. Subsequently, the corresponding bilateral area attached to the ACL was stimulated by the bipolar surface electrode. The stimulative parameter was constant voltage (single-phrase square wave electrical stimulation; frequency, 2 Hz; pulse width, 0.1 ms; intensity, 25–30 mA). The waveform and the latent period of MNCV were measured and analyzed.
Statistical analysis
Statistical analyses were performed using SPSS (version 20.0; IBM Corp.), and Photoshop (version 2018, Adobe Systems Incorp.) was used to stitch figures. Shapiro-Wilk test was used to check data normality. Normally distributed data are presented as the mean ± standard deviation, and non-normally distributed data are presented as percentiles 25 and 75 (P25–75). Wilcoxon-Mann-Whitney test was used to analyze physiological data, and statistical significance was set at p < 0.05. Kruskal-Wallis followed by Dunn’s multiple comparison test was used to analyze electrophysiological data, and therefore statistical significance was set at p < 0.009 in this comparison.
Results
Monkey condition
2 weeks after the surgery, in the model group, incisions of all monkeys healed, no monkeys were infected, and their operated limbs could gradually move. In the blank control group, all monkeys remained healthy and had no reports of anything unusual. After all procedures, all monkeys were still fed carefully for further studies.
Physiology
Prior to surgery, no significant difference was found between the model group and the blank control group, including age, weight, maximum degree of knee flexion, the thigh and the calf circumference, and Pivot-shift, Anterior drawer and Lachman test results (p > 0.05; Table 1). After surgery, in the blank control group, no significant difference was observed compared with the preoperative data (p > 0.05). In the model group, no significant difference was also found in the maximum degree of knee flexion, the thigh circumstance or the calf circumference; however, the Pivot-shift, Anterior drawer and Lachman test results were significantly different (p < 0.05; Table 2).
Baseline characteristics before the surgery.

Normally distributed data are presented as the mean ± standard deviation, and non-normally distributed data are presented as percentiles 25 and 75 (P25–75). Wilcoxon-Mann-Whitney test was used, and p < 0.05 were considered as significant.
Comparison of physiological characteristics.
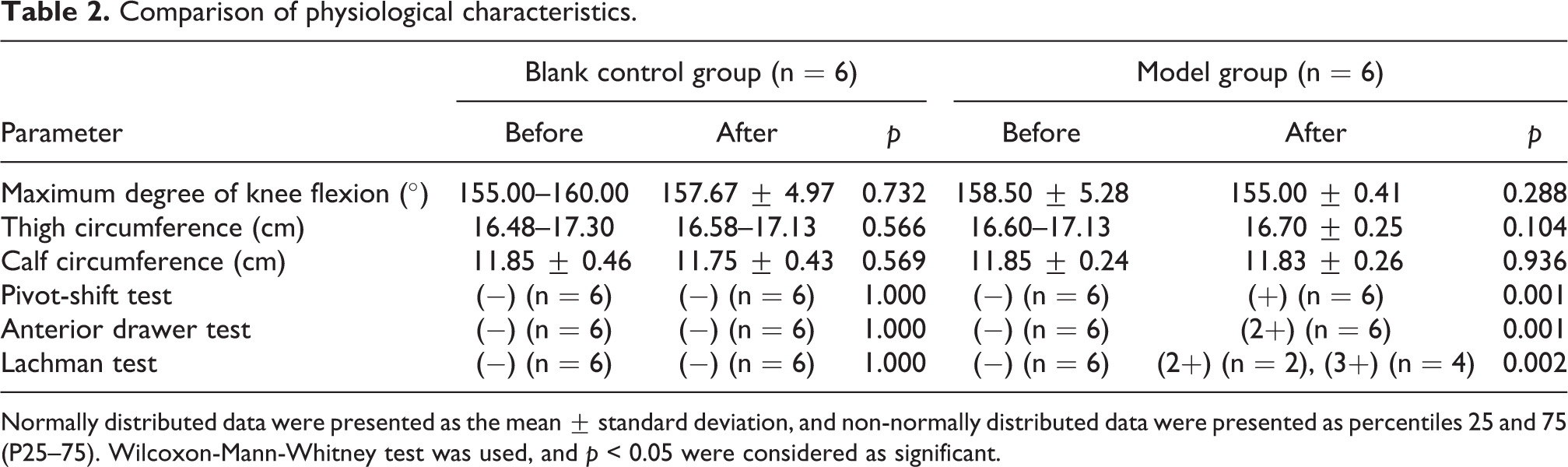
Normally distributed data were presented as the mean ± standard deviation, and non-normally distributed data were presented as percentiles 25 and 75 (P25–75). Wilcoxon-Mann-Whitney test was used, and p < 0.05 were considered as significant.
Nerve electrophysiology
After the surgery, the latent period of SEPs and MNCV were significantly increased in the model group (p < 0.009; Table 3), whereas the amplitude of SEPs and MNCV was decreased (p < 0.009; Table 3), indicating nerve injury and reduced proprioception of the knee joint.
Comparison of electrophysiological characteristics.

SEPs: somatosensory evoked potentials; MNCV: motor nerve conduction velocity.
Normally distributed data are presented as the mean ± standard deviation, and non-normally distributed data are presented as percentiles 25 and 75 (P25–75). Kruskal-Wallis followed by Dunn’s multiple comparison test was used, and therefore p < 0.009 was considered as significant in this comparison.
Discussion
Every year >2 million people suffer from an ACL injury worldwide, 23 and the available treatment strategies have been under improvement due to improved understanding of knee kinematics and progressive surgical techniques. 24
At present, there are two treatment strategies used in clinic, conservative treatment and ligament reconstruction. The majority of studies consider the former as the gold standard of ACL mild injury, and the latter as the gold standard of ACL severe injury. However, the treatment of ACL moderate injury is uncertain. A number of studies have identified prognostic factors for postoperative adverse outcomes after ACL reconstruction and deem it not a prerequisite for returning to recreational physical activities after ACL tears, while some other researchers doubt the efficiency of conservative treatment on the stability and proprioception restoration. 25 –27 Under the circumstances, higher quality studies and randomized controlled trials are required to confirm the most appropriate treatment strategy. 28
The present study developed a proprioceptive deficit model of the ACL to compare the two treatment strategies and help to promote the development of proprioception restoration. Arthoscopy was used, which has been widely used in knee joint surgery and has been reported to be safe. 29 –31 As a well-established technique, arthroscopy only required a 0.5 cm incision to be made, decreasing the risk of infection, inflammation and tissue damage, as well as shortening the healing time. 32 In addition, reducing bleeding during surgery can avoid blood accumulating in the knee joint, which would contribute to unwanted effects post-surgery. Furthermore, due to the small size of the incision, it allows for the joint cavity to be detected and for 1/4 of the ACL to be cut more precisely, reducing damage to the surrounding tissues and the ACL. Previous studies have often performed open surgery to establish an ACL model, leading to an opposite result. As a result, arthoscopy was selected in the present study.
In the model group, 1/4 of the ACL was cut under an arthroscope to simulate ACL moderate injury, whereas in the blank control group no intervention was performed. Before and after the surgery, the maximum degree of knee flexion, the thigh and the calf circumference were measured, and the Pivot-shift, Anterior drawer and Lachman tests were performed. In the model group, no significant difference was observed in the maximum degree of knee flexion, the thigh circumstance and the calf circumference (p > 0.05), indicating that short term knee instability would not lead to atrophy of hind limb muscles and decrease knee flexion. However, the Pivot-shift, Anterior drawer and Lachman tests displayed the opposite results (p < 0.05). Moreover, physiological data were measured, including SEPs and MNCV. SEPs and MNCV were assessed via two indicators: the latent period and the amplitude. In the model group, after the surgery, the latent period of SEPs and MNCV was increased (p < 0.009), whereas the amplitude of SEPs and MNCV was decreased (p < 0.009). Collectively, the results indicated decline of proprioception and instability of the knee joint.
The present study had a number of limitations. Firstly, only male monkeys were used and the effects of sex were not examined. In future studies, both male and female monkeys should be used to examine the effects of sex. In addition, all postoperative measurements were performed within only 3 months post-recovery, due to time limitation. Therefore, the present study lacked long term follow-up to assess subsequent alterations to proprioception. Moreover, the present study did not perform pathological staining or immunohistochemistry, or evaluate microscopic alterations to the ACL. What is more, the present study did not include a positive group. Lastly, the study did not demonstrate the capability of ACL reconstruction to restore the effects caused by ACL transection. All those limitations should be investigated and addressed in further studies.
To conclude, the proprioceptive deficit model of the ACL in cynomolgus monkeys was successfully established. The model simulated the proprioceptive deficit of human ACL moderate injury and may aid with further understanding the underlying mechanism.
Conclusions
After cutting 1/4 of the ACL, the knee joint appeared to be unstable and proprioception was declined. The results indicated that the proprioceptive deficit model of the ACL was successfully established, which could aid with further studying ACL injury.
Footnotes
Author contributions
Lei Zhang and Ruihan Wang contributed equally to this work.
Data and materials availability
The data and materials used and analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by National Natural Science Foundation of China (Youth Science Foundation Project) [grant number 82004458]; Traditional Chinese Medicine Research Project of Sichuan Traditional Chinese Medicine Administration [grant number 2020JC0138]; Luzhou People’s Government–Southwest Medical University Science and Technology Strategic Cooperation Project [grant number 2018LZXNYD-ZK43]; Shi-zhen Zhong Academician Talent Team Sub-project [grant number 2018zszysrctdxm]; and Affiliated Traditional Chinese Medicine Hospital of Southwest Medical University Research Project (National Nature Foundation Training Program) [grant number 2019XYLH-001].