
Abstract
Objective
Radiofrequency (RF) shrinkage is used in anterior cruciate ligament (ACL) reconstruction. The present study investigated the therapeutic effects of RF on ACL relaxation and the probable influencing factors.
Methods
Patients with ACL relaxation were included. Participants were randomly divided into two groups: a treatment group, in which patients were treated with RF shrinkage (RF group); a control group, in which patients received conventional surgical treatment. Thermal shrinkage was performed on ACL using an ArthroCare® CAPSure® wand. Lysholm scores, proprioceptive testing and Tegner activity scores were evaluated before and after treatment (at 6 and 12 months).
Results
A total of 38 patients were included. The mean ± SD Lysholm score of those in the RF group at 12 months’ post-treatment was significantly higher than in controls. The angle of deviation of the knee joint in RF group was significantly larger than in the control group at 6 months’ post-treatment.
Conclusions
RF shrinkage treatment for ACL laxity could improve knee scores, and may affect proprioception and recovery of activity after surgery.
Introduction
The anterior cruciate ligament (ACL) is an important structure for maintaining knee stability: it is responsible for both static stability as well as dynamic stability of the knee joint, as the ligament contains tension receptors that can control muscle contraction. ACL injury can lead to joint instability, resulting in the loss of physiological movement, as well as the load conduction disorders and intra-articular damage.
Ligament reconstruction has been accepted as the standard treatment for ACL rupture, but conflicts remain about the preferred treatment for ACL relaxation.1,2 Ligament reconstruction can restore joint stability, but a certain degree of damage may follow the surgery.3–5 Bipolar radiofrequency (RF) shrinkage provides a means to treat ACL relaxation, in addition to being used for ACL reconstruction.6–9 The principle of RF is to repair the degenerated collagen fibres at 65℃, to restore ligament tightening.10,11 The present study evaluated the effects of RF shrinkage treatment on ACL relaxation and the probable influencing factors.
Patients and methods
Study population
Consecutive patients with ACL relaxation were included in this study, which was conducted at the Chinese PLA General Hospital, Beijing, China, between May 2008 and December 2010. Patients were eligible for the study if they had ACL laxity (diagnosed based on visible observation, an abnormal Lachman test and abnormal anterior drawer test), and were between 18 and 50 years of age. Exclusion criteria were ACL tear and serious osteoarthritis in the same knee joint. ACL laxity, with complete ligaments but poor continuity, was diagnosed based on visible observation, abnormal Lachman test 12 (where the patient’s affected knee is flexed to 30° and the examiner pulls on the tibia to assess the range of anterior motion) and abnormal anterior drawer test (where the patient is placed in the supine position with the hip flexed at 45° and the knee at 90°, and the tibia is pulled forward by the examiner to assess the range of motion compared with the normal limb), during exploration using arthroscopy. Patients were randomized into two groups at study entry according to a computer-generated randomization schedule: a treatment group in which patients were treated with RF shrinkage (RF group) and a control group where patients received conventional therapy.
The study was approved by the Ethics Review Committee of the Chinese PLA General Hospital. All patients participating in the study provided verbal informed consent. The Declaration of Helsinki was followed during the performance of this study.
RF treatment
In the RF group, thermal shrinkage was performed on the ACL using ArthroCare® CAPSure® A1830 wand with a power setting of two (Arthrocare Corp., Austin, TX, USA). In addition, synovial resection, meniscal repair or cartilage repair were adopted for synovitis, meniscus tear and cartilage damage, respectively. Postoperatively, patients were placed in hinge orthosis (Smith & Nephew, Memphis, TN, USA) which were allowed to bear weight and unrestricted motion for 6 weeks. Meanwhile, closed-chain exercises, such as knee flexion (0–90°), and once a week rehabilitation training for triceps, were advanced as tolerated. At 6 weeks following treatment, the brace was only used during walking, while weight-bearing, walking and a wide range of activities was advised. After 3 months, the orthosis was released and exercises extending to terminal extension loads were initiated, but severe exercises were avoided up to 6 months following therapy. Treatment for patients in the control group was same as those in the treatment group, with the exception of thermal shrinkage.
Study assessments
Scoring systems were used to evaluate ACL and knee function (including the Lysholm knee scoring scale, 13 proprioceptive test and Tegner activity scale 13 ) before and after treatment.
The Lysholm knee scoring scale is based on a questionnaire completed by patients that comprises eight sections (limp; use of cane or crutches; locking sensation; giving way sensation; pain; swelling; climbing stairs; squatting), with multiple questions. Each question carries a predetermined score with a maximum possible test score of 100, with high scores indicating severe disability.
The Tegner activity scale is a questionnaire to assess the level of activity of a patient before and after injury. This questionnaire comprises 11 levels in descending order, from competitive sports at level 10 to sick leave or disability pension at level 0. This scale is used during recovery from treatment to determine patients’ rehabilitation needs.
Proprioception of the knee was measured by the reproduction of passive positioning of the knee in standing position (bending test) and sitting position (straight test). First, femoral trochanter, femoral epicondyle, fibular head and fibular lateral condyle were marked on the body surface. Participants stood, blindfolded, then one leg was flexed to 30° and 60° for 5 min while using the other leg as support; patients then returned to the standing position. This action was repeated three times and the joint angle was recorded using a digital camera; the joint angle was calculated using the markers on the body surface. Proprioception in the sitting position was measured in a manner similar to the standing test.
Statistical analyses
Database management and analyses were undertaken using the SPSS® statistical software package, version 10 (SPSS Inc., Chicago, IL, USA) for Windows®. Data were presented as mean ± SD; between-group comparisons were made using a paired t-test. A P-value < 0.05 was considered to be statistically significant.
Results
A total of 38 patients with ACL relaxation were included in this study. In the RF group, 16 patients (eight men and eight women) were followed for 12 months. Three patients received ligament reconstruction surgery within 1 year because of ligament rupture (two cases due to severe exercise; one due to dissatisfaction with therapeutic efficacy). In the control group, 15 patients (eight men and seven women) were followed up for 12 months: one patient received ligament reconstruction surgery within 1 year because of dissatisfaction with therapeutic efficacy and three patients were lost to follow-up.
Characteristics of patients with anterior cruciate ligament (ACL) relaxation, treated with (RF group) or without (control group) radiofrequency (RF) treatment to perform thermal shrinkage of the ACL.

Data presented as mean ± SD.
No statistically significant between group differences observed (P ≥ 0.05); paired t-test.
Lysholm and Tegner scores 13 pretreatment and at 6 and 12 months’ post-treatment in patients with anterior cruciate ligament (ACL) relaxation, treated with (RF group) or without (control group) radiofrequency (RF) treatment to perform thermal shrinkage of the ACL.

Data presented as mean ± SD.
P < 0.05 versus pretreatment values; P < 0.05 versus control group; paired t-test.
Proprioception (standing position, bending test) a test results pretreatment and at 6 and 12 months’ post-treatment in patients with anterior cruciate ligament (ACL) relaxation, treated with (RF group) or without (control group) radiofrequency (RF) treatment to perform thermal shrinkage of the ACL.
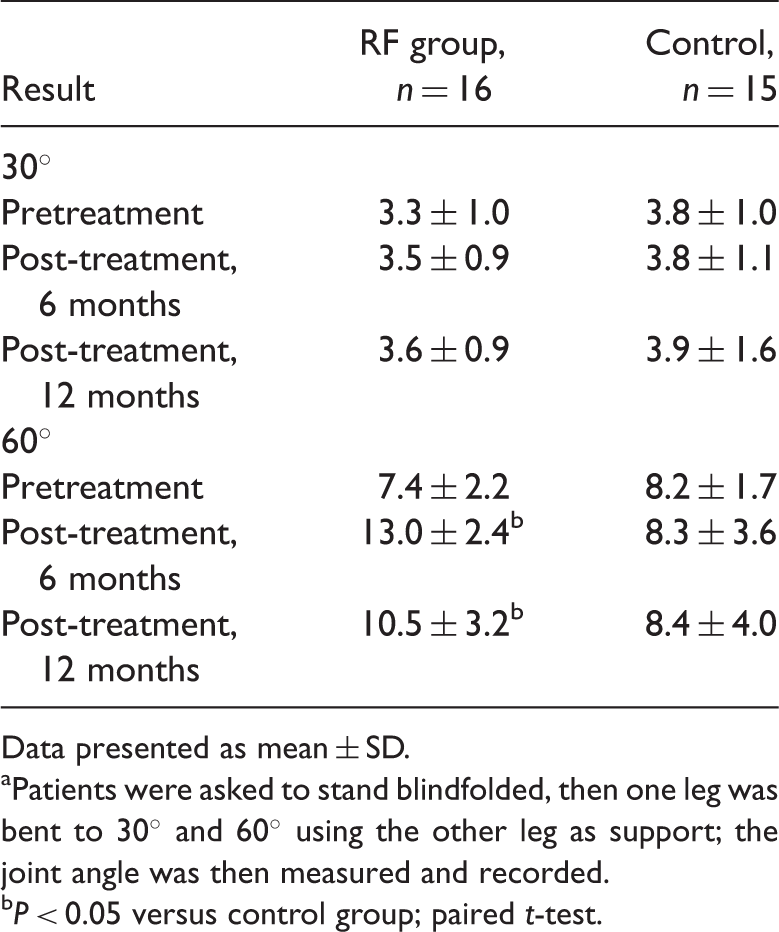
Data presented as mean ± SD.
Patients were asked to stand blindfolded, then one leg was bent to 30° and 60° using the other leg as support; the joint angle was then measured and recorded.
P < 0.05 versus control group; paired t-test.
Proprioception (sitting position, straight test) a test results pretreatment and at 6 and 12 months’ post-treatment in patients with anterior cruciate ligament (ACL) relaxation, treated with (RF group) or without (control group) radiofrequency (RF) treatment to perform thermal shrinkage of the ACL.

Data presented as mean ± SD.
Patients were seated blindfolded, then one leg was straighted to 30° and then to 60°; the joint angle was then measured and recorded.
P < 0.05 versus control group; paired t-test.
Discussion
Radiofrequency shrinkage can reconfigure the structure collagen fibres from a triple-helix into a random coil, resulting in tightening and improved stabilization of the joint. 14 It is generally believed that 65–75℃ is the temperature range offering the most favourable safety profile for RF treatment. 15 RF can penetrate to ∼1–5 mm, with the depth being related to treatment time. 16 The temperature of RF is the important factor in determining the therapeutic efficacy. Collagen degeneration would occur if the temperature was too high or if the duration of treatment was prolonged.17,18
The ligament can be repaired by the occurrence of fibrosis, which is followed by the growth of blood vessels and nerve fibres into the injured ligament; the collagen is then reconstructed. It has been shown that the ductility of the ligament is increased for 6–12 weeks following RF treatment.19–21 Thus, the biomechanical strength of the ligament would be inevitably weakened in the short term after RF treatment, and the risk of ligament rupture would be increased. Two ligament ruptures were observed in the present study as a result of strenuous sports activity, which suggests that immobilization and functional rehabilitation after ACL RF shrinkage is very important.
The clinical effects of RF shrinkage have yet to be fully defined. In another study, 11 of 18 participants experienced ligament laxity 4 months after RF shrinkage treatment. 21 Additionally, following RF shrinkage, the distance of the tibia forward of the knee has been shown to decrease from 13.1 mm to 2.6 mm and the Lysholm score to increase from 35.9 to 88.5. 22 Studies reveal that the efficiency of RF shrinkage is close to 90%,23–25 whereas another showed that it was only 49.2%. 26 Since relaxation, ruptures and reconstruction are reported differently among those studies, it is difficult to compare them.
Proprioception is the sense of joint position and movement, and its receptors are widely present in the joints and the surrounding soft tissues. Histological studies have shown that there are a large number of mechanoreceptors in the ACL, which is the main site that receives proprioceptive impulses. 27 Proprioception can control the activities of the muscles around the joint, which are important in maintaining joint stability. It has been suggested that ACL functional reconstruction should include remodelling of nerve functions, in addition to the reconstruction of mechanical properties.28,29
The measurement of proprioception is difficult and can only be done indirectly. Proprioception can be evaluated using two movement progressions: passive movement in a non-weight-bearing position; initiative movement in a weight-bearing position. The latter can reflect the systematic status of position and the movement of skin, muscles and joints, which mimic those found in normal life.30,31 Proprioception remodelling after ACL reconstruction has been shown to be as good as that observed in normal healthy subjects; but few studies have observed the effects of ACL laxity on proprioception.32,33
The present study showed that the Lysholm score after treatment was significantly higher than before treatment, in both the RF and control groups. In addition, the Lysholm score in the RF group was significantly higher than that in the control group following treatment. These data suggest that immobilization and rehabilitation training after surgery can improve joint function. The efficacy of RF shrinkage treatment is better than conventional therapy, although knee proprioception is decreased in the short term. We observed no significant improvement in Tegner scores after surgery. It could be speculated that surgical treatment may lead to a decline in proprioception, which can affect confidence-building in returning to the original level of physical activity. In addition, the long period of ACL laxity makes most people reluctant to engage in their original sporting events, and the time of immobilization is prolonged because of the risk of ligament rupture after surgery.
In conclusion, RF shrinkage treatment for ACL laxity could improve knee score. Meanwhile, joint proprioception may deteriorate and the recovery of movement after surgery could be affected.
Footnotes
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.