
Abstract
Purpose:
This study aims to systematically review the literature comparing surgical treatments options and respective failure rates for basicervical hip fractures.
Methods:
A comprehensive search of databases, including MEDLINE, Embase, Web of Science, and Cochrane Central for studies published in English on or before June 21, 2019 was performed. Selected search terms included “basicervical,” “basi cervical,” “AO/OTA type 31-B,” “femoral neck fracture” AND “bone nails,” “bone screws,” “fracture fixation,” “internal fixation,” “arthroplasty,” “cephalomedullary,” “sliding hip screw,” “ORIF,” and “treatment outcome.” We included studies that assessed outcomes of basicervical fracture fixation using open reduction internal fixation or arthroplasty. Two authors extracted the following data from each paper: study design, country, cohort year, definition of basicervical, intervention type, sample size, patient demographics, follow-up length, percent of fractures that required revision, and the percent of implants that failed.
Results:
Sixteen articles encompassing 910 patients were included. The main outcome was the percent of implants that required revision. The total revision rates were 8% (8 studies, 157 patients, range 0%–55%) for cephalomedullary nails, 7% (10 studies, 584 patients, range 0%–18%) for sliding hip screws, 23% (3 studies, 40 patients, range 16%–50%) for cannulated screws, 0% (1 study, 6 patients) for total hip arthroplasty, and 8% (2 studies, 13 patients, range 0%–11%) for hemiarthroplasty.
Conclusion:
Management of basicervical fractures with SHS and CMN produces similar failure and re-operation rates. Limited evidence is available on the use of cannulated screws and arthroplasty, but available studies suggest that cannulated screws have an unacceptable revision rate (23%) while arthroplasty may be acceptable. Future studies examining the comparative efficacy of various fixation methods would benefit from strict definition of fracture type as well as consistent reporting of functional outcomes, re-operation rates, and mortality.
Introduction
Fractures of the proximal femur are a significant cause of morbidity and mortality worldwide, especially in patients over the age of 50. 1 Overall, hip fractures in older adults are common, with femoral neck fractures accounting for 3.6% of all fractures. 2,3 The treatment of a subset of these fractures, basicervical femoral neck fractures, is still controversial due to challenges in classification and limited evidence regarding treatment outcomes.
Basicervical fractures are relatively rare compared to other femoral neck fractures, accounting for only 1.8–7.6% of all hip fractures. 3 There exists some heterogeneity in how basicervical fracture are defined, but one common definition is fractures of the base of the femoral neck that occur medially from the intertrochanteric line above the lesser trochanter. 4 There is currently limited evidence regarding optimal implant choice for basicervical fractures. Implant choice has been proposed to depend on the extent of displacement, fracture configuration, physiological age and bone quality. 3 Arthroplasty procedures are favored for older adults, as it may allow for earlier weight-bearing. 5 Plates and screws or cephalomedullary devices have been proposed to maintain the native hip joint, but studies have commented on an increased mortality and failure rate when these methods are used to treat basicervical fractures, suggesting biomechanical instability and an increased rate of implant-related complications in this fracture subtype. 6,7 Patient-reported outcomes following basicervical neck fracture treatment have also been reported to lag behind those of either more proximal femoral neck fractures or intertrochanteric fractures. 8,9
To our knowledge, few studies have examined the management of basicervical fractures. This study aims to systematically review the literature comparing surgical treatments options and respective failure rates for basicervical hip fractures.
Materials and methods
Search strategy
This systematic review was performed in accordance with published guidelines by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) Statement. 10 The protocol has been registered at PROSPERO (ID = CRD42019137790). We searched MEDLINE, Embase, Web of Science, and Cochrane Central for studies published on or before June 21, 2019. Articles that were electronically published but not yet available in print were included. 11 Selected search terms included “basicervical,” “basi cervical,” “AO/OTA type 31-B,” “femoral neck fracture” AND “bone nails,” “bone screws,” “fracture fixation,” “internal fixation,” “arthroplasty,” “cephalomedullary,” “sliding hip screw,” “ORIF,” and “treatment outcome.” The search strategy is outlined in Appendix. During screening, the reference sections of included studies and systematic reviews were manually screened to identify additional relevant articles.
Study selection
Two investigators independently screened the studies for eligibility, using the following inclusion criteria: (1) adult patients with basicervical fracture; (2) treatment with either ORIF (nail/screw) or arthroplasty; (3) outcomes, specifically revision rate, of basicervical group reported; (4) availability of full-text articles in English. To maximize the total number of fractures included in our analysis, there was no requirement for the minimum number of fractures included in the study, the minimum length of follow-up, or the minimum age of included patients. Abstracts, systematic reviews, cadaveric and technical studies and meeting presentations were excluded. Ipsilateral neck/shaft fractures were excluded. In mixed series, for example studies that included both basicervical and intertrochanteric fractures, only groups that met the inclusion criteria and reported separate data for basicervical fractures were included in the analysis.
The screening was conducted using Covidence systematic review software (Veritas Health Innovation, Melbourne, Australia). First, two investigators independently classified studies as ineligible or potentially eligible based on title and abstract. If both investigators agreed, the full text was assessed for inclusion. In the event of a discrepancy, a third author was consulted. This process was repeated during the assessment of full-text articles for inclusion. Two investigators independently appraised the included studies using The Cochrane Collaboration’s tool for assessing risk of bias. The search yielded 2736 articles, of which 16 were included in this study (Figure 1).

PRISMA flowchart depicting search results and study selection. The number of studies identified during initial search, added during reference screening, excluded during duplicate removal, excluded during title and abstract screening, excluded during full-text review, and included in the final analysis is included in parentheses within each box. For articles excluded during the full-text review, the reason for exclusion and number of studies excluded for each reason is included.
Data extraction
Two authors extracted the following data from each paper: study design, country, cohort year, definition of basicervical, intervention type, sample size, age at time of injury, sex ratio of patients, follow-up length, percent of fractures that required revision, and percent of implants that failed. The primary outcome was revision rate. Other extracted variables include radiographic malunion, perioperative complications, mortality within 1 year of operation, and time to weight-bearing; however, these were not included in further analysis because so few papers (≤4) reported on these outcomes. The definition of basicervical and failure rate (defined as nonunion, implant cutout, implant breakage, femur fracture, and avascular necrosis) were analyzed as secondary outcomes.
Data analysis
Heterogeneity among included papers and limited literature reporting basicervical outcomes prevented meta-analysis. Quantitative statistical analysis was not pursued in depth due to the relative paucity of data and resulting lack of power as determined by post-hoc testing. Data including study design, country in which the study was performed, number of included patients, mean age, duration of follow-up (months), type of surgery, and outcome measures were collected from individual manuscripts and compiled in order to obtain descriptive statistics and characterize the years of included studies, treatment options, sex ratio of patients, and average age of patients. The rate of revision and total failure rate was calculated for each study. The total rate of revision and total failure rate for each fixation method was then calculated.
Results
Demographics
Sixteen articles were included, dating from 1991 to 2020. There were 910 patients with basicervical fractures with 43% being male and an average age of 76 ± 4.8 years. Treatment options included sliding hip screws, (SHS) (10 studies), hemi or total hip arthroplasty (HA or THA) (4 studies), cephalomedullary nails (CMN) (8 studies) and cannulated screws (CS) (3 studies), with some studies including two or more treatment groups (Table 1). Mean follow-up duration ranged from 12 to 75 months.
Characteristics of included studies.
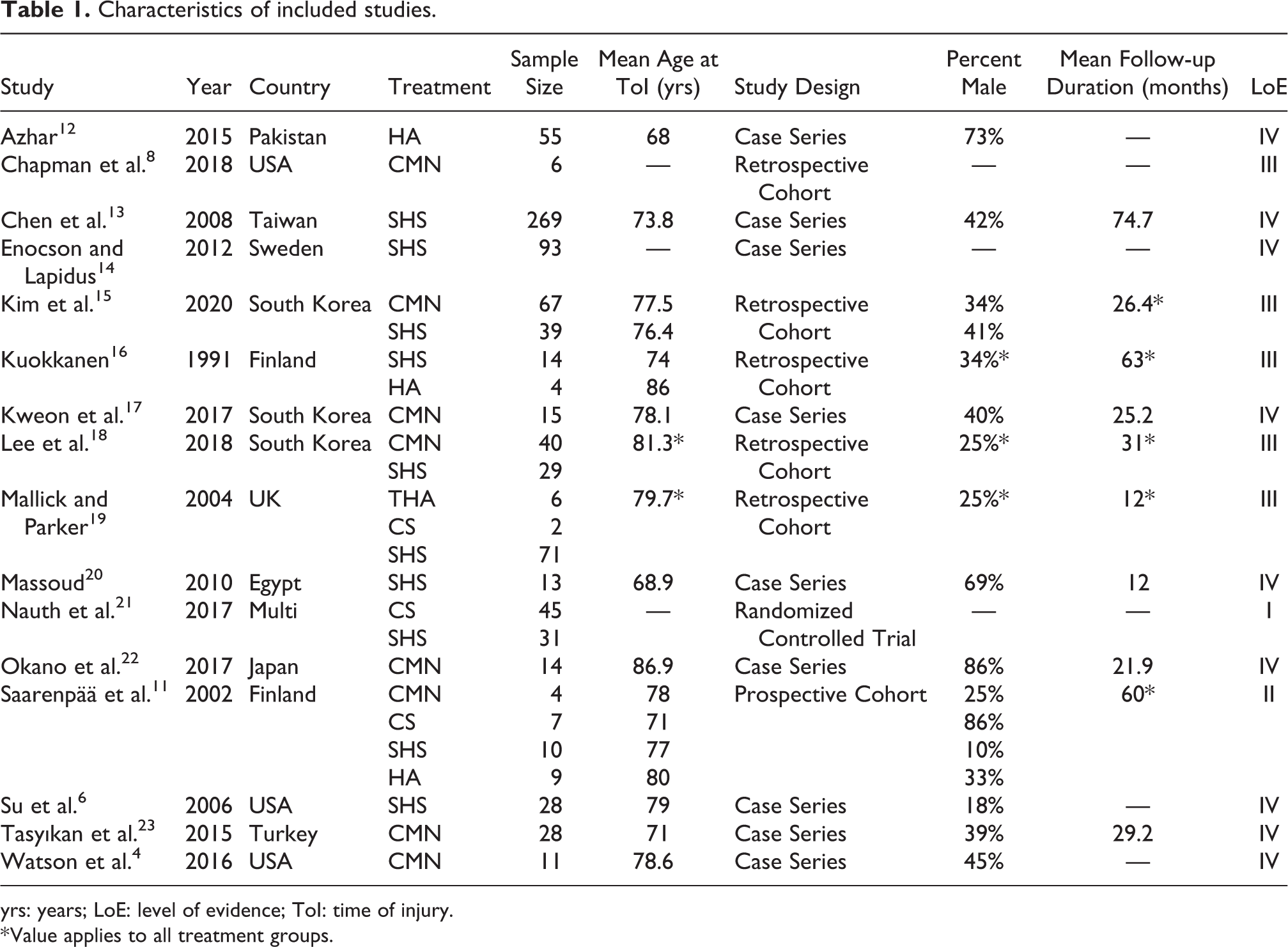
yrs: years; LoE: level of evidence; ToI: time of injury.
* Value applies to all treatment groups.
Diagnosis
The diagnostic criteria of basicervical fractures varied between studies. Four studies specified that the fracture line must lie medial to the intertrochanteric line. 4,22,18,15 Eight studies stated that the fracture line could run along the intertrochanteric line or at the junction of the femoral neck and the intertrochanteric region. 11,6,19,13,20,17,23,14 One study specified that the fracture line must be distinctly extracapsular and located on the femoral neck. 16 One study used the AO/OTA guidelines as diagnostic criteria. 8 One study did not state diagnostic criteria but the radiographs were assessed by the orthopaedic surgeon. 12 All studies defined them as basicervical hip fractures. Given the scarcity of literature on basicervical fractures, all above studies were included in our final analysis.
Outcomes
Revision rate was the most frequently reported outcome across studies. The total revision rates were 8% (8 studies, 157 patients, range 0%–55%) for cephalomedullary nails, 7% (10 studies, 584 patients, range 0%–18%) for sliding hip screws, 23% (3 studies, 40 patients, range 16%–50%) for cannulated screws, 0% (1 study, 6 patients) for total hip arthroplasty, and 8% (2 studies, 13 patients, range 0%–11%) for hemiarthroplasty. Reason of failure, mortality, radiographic malunion, perioperative complications, and time to weight-bearing were not consistently reported across studies, so these outcomes were not included in our analysis. Table 2 shows the revision rate and total failure rate of each study. “Notably, only three studies (with n = 13 fractures) reported on revisions and failures following HA, and only one study (with n = 6 fractures) reported on revisions and failures following THA.”
Average revision rate and total failure rate across fixation methods.
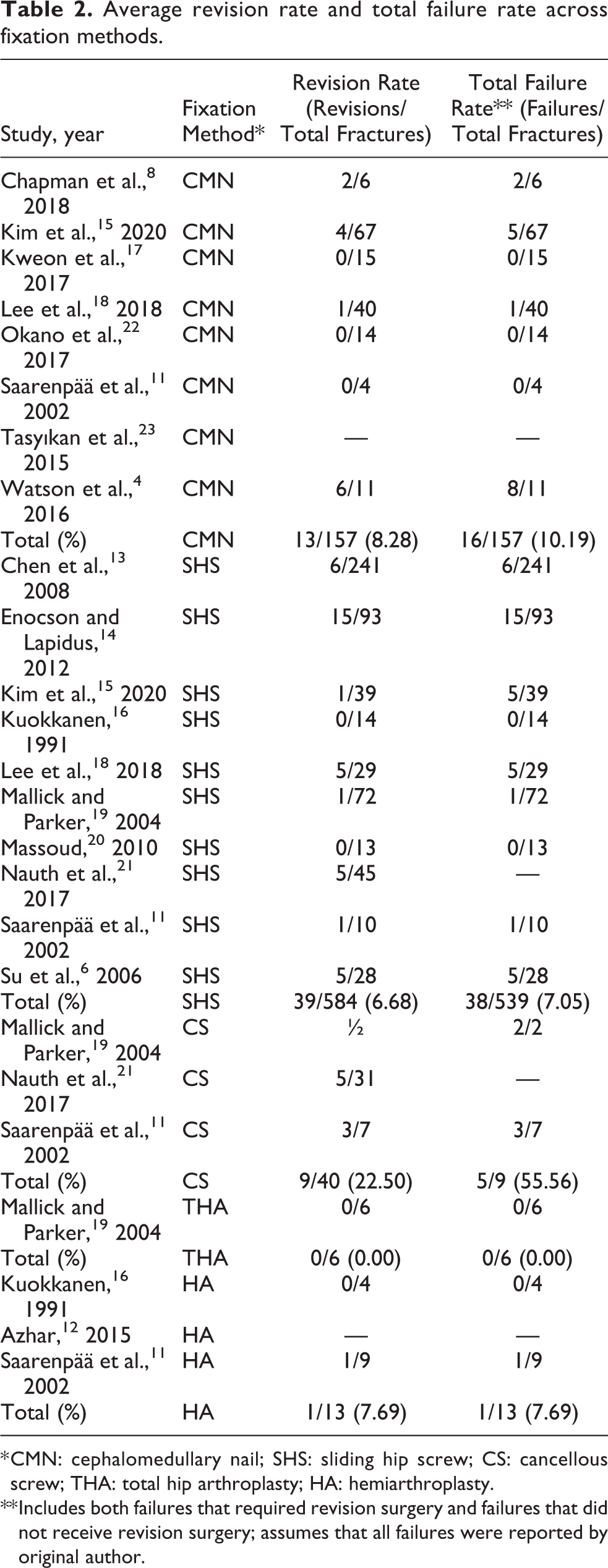
* CMN: cephalomedullary nail; SHS: sliding hip screw; CS: cancellous screw; THA: total hip arthroplasty; HA: hemiarthroplasty.
** Includes both failures that required revision surgery and failures that did not receive revision surgery; assumes that all failures were reported by original author.
Discussion
Main findings
Our results suggest that SHS and CMN may result in similar rates of revision (7% and 8% respectively) and failure (7% and 10% respectively) with a slightly higher rate of complications with a CMN. Additionally, though evidence is limited, the use of multiple cannulated screws appears to have an unacceptable failure rate (56%) and should be discouraged in surgical treatment of basicervical fractures. Many clinically important variables were not consistently reported across studies. We suggest that future studies include reason of failure, mortality, radiographic malunion, perioperative complications, and time to weight-bearing as outcomes. At this time, it is not possible to determine the optimal fixation method for basicervical fractures due to the limited number of high-quality comparative studies necessary for in-depth quantitative analysis, but this data suggests using a SHS.
Diagnosis
The management of basicervical fractures is still controversial because of the difficulty in accurately diagnosing the fracture. Classification based on radiographs is often difficult due to poor quality and inadequate projections. In AP radiographs, a basicervical fracture is often obscured by the trochanteric area, which makes the fracture line poorly visible or invisible; a lateral projection that provides unobstructed visualization of the level of the fracture line is essential for reliable classification. 11,24 Due to the aforementioned radiologic limitations; it may be advantageous to consider CT imaging when standard radiographs cannot definitively diagnose a basicervical fracture. However, diagnosis is further obscured by the lack of a precise definition for “basicervical fracture” among orthopedists. In the studies reviewed here, some studies defined basicervical fractures as those in which the fracture lies medial to the intertrochanteric line, 4,22,18,15 some defined basicervical fractures as those where the fracture runs along the intertrochanteric line, 19,13 and others defined basicervical fractures as a subset of intertrochanteric fractures in which the fracture line can be seen radiologically to cross close to the base of the femoral neck and its junction with the intertrochanteric region. 25 We suggest that the diagnosis of basicervical fractures should be limited to those with no involvement of any part of the trochanteric region, including the greater trochanter.
Treatment options and outcomes
Fixation of basicervical fractures is complicated by the challenge of achieving stable fixation given the extracapsular fracture line, high fracture angle, and lack of muscular attachment to its proximal fragment. 20 Our findings suggest that fixation of basicervical fractures in older adults by SHS is associated with lower rates of re-operation when compared to CMN. These findings, along with prior randomized-control trials, suggest that SHS is an acceptable treatment for basicervical fractures, and the utility of SHS as a fixation method seems to be independent of the use of derotational screws, which may not have an effect on fracture stability or clinical outcome. 6,21 These findings may contradict previous studies showing that basicervical fractures appear to behave as unstable extracapsular fractures rather than as intracapsular fractures. 26 Studies descriptively defining basicervical fractures as excluding the trochanteric region have found that CMN may yield poor functional outcomes. Watson et al. evaluated 11 patients who underwent fixation of basicervical neck fractures with CMN and found implant failure in 6 out of 11 patients despite anatomic or near-anatomic reduction at the time of surgery. 4 Similarly, Okano et al. found that 2 out of 16 patients treated with CMN for basicervical fractures had implant-related complications. 22
The efficacy of SHS in intertrochanteric hip fractures has been previously validated by biomechanical studies. Deneka et al. found in a cadaveric model of a basicervical femoral neck fracture that SHS maintained a higher average peak force and ultimate load to failure than CMN. 27 These findings are also in concordance with Imren et al. and Blair et al., who concluded that fixation strength was higher in SHS compared to cannulated compression screws (CCS). 28,29
Yet, clinical data on the optimal fixation technique for basicervical fractures among older adults have been limited and controversial. Several studies have concluded—similar to our findings—that surgical treatment of acute basicervical fractures of femur with SHS provides satisfactory results. 6,19,13
Limitations
A limited body of research, heterogeneity in classification, considerable diagnostic imprecision, and inconsistent reporting present limitations for both this study as well as the literature on the basicervical fracture pattern. Given the relative rarity of basicervical fractures, clinical data comparing treatment modalities remains sparse. Here, though multiple treatment methods were compared, low numbers of patients treated with arthroplasty or cannulated screws precludes meta-analysis and quantitative analysis; it therefore also obscures clinical conclusions. Regarding diagnostic imprecision, it is similarly conceivable that poor quality and inadequate projections could contribute to considerable inter-observer variability in classifying basicervical fractures. However, we only included studies that were robust in their classification schema, and studies were internally consistent with their stated definitions. Additionally, reported outcome measures also varied considerably across included studies. For example, though re-operation rates were commonly reported, other measures such as mortality and functional outcomes were inconsistently reported for basicervical fractures. Future studies would benefit from consistent reporting of: (1) functional outcomes using standardized measures (e.g. Harris Hip Score); (2) re-operation rates; and (3) 90-day mortality rates in order to enable comparison across fixation methods.
Conclusion
The optimal management of basicervical fractures is still controversial due to imprecise characterization and inherent instability of these fracture types. Based on the current data we cannot make a conclusion on optimal management, though SHS may produce lower re-operation rates when compared to CMN. However, not enough data exists to definitively establish the optimal fixation method. There are too few studies that report on the outcomes of basicervical fractures treated with total hip arthroplasty, hemiarthroplasty, and cannulated screws. Though evidence is limited, the use of multiple cannulated screws appears to have an unacceptable failure rate and should be discouraged in surgical treatment of basicervical fractures.
Supplemental material
Supplemental Material, sj-docx-1-osj-10.1177_23094990211003344 - Treatment and outcomes of basicervical femoral neck fractures: A systematic review
Supplemental Material, sj-docx-1-osj-10.1177_23094990211003344 for Treatment and outcomes of basicervical femoral neck fractures: A systematic review by Mihir S Dekhne, Hannah M. Thomas, Thomas Haider, Sharri Mortensen, Edward K. Rodriguez, Michael J. Weaver and Arvind von Keudell in Journal of Orthopaedic Surgery
Supplemental material
Supplemental Material, sj-docx-2-osj-10.1177_23094990211003344 - Treatment and outcomes of basicervical femoral neck fractures: A systematic review
Supplemental Material, sj-docx-2-osj-10.1177_23094990211003344 for Treatment and outcomes of basicervical femoral neck fractures: A systematic review by Mihir S Dekhne, Hannah M. Thomas, Thomas Haider, Sharri Mortensen, Edward K. Rodriguez, Michael J. Weaver and Arvind von Keudell in Journal of Orthopaedic Surgery
Footnotes
Declaration of conflicting interests
The author(s) declared potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Arvind von Keudell - consulting fees from Stryker.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.