
Abstract
Purpose:
The aim of this study was to assess the effects of the COVID-19 pandemic on anxiety, sleep outcomes and change in clinical management practices among orthopaedic surgeons following a nation-wide lockdown.
Methods:
We conducted an online cross-sectional study using piloted structured questionnaires with self-reported responses from Indian orthopaedic surgeons. Study participants were identified through social networking sites: Facebook and WhatsApp. The extent of anxiety and sleep quality was assessed by the standardised seven-item Generalised Anxiety Disorder (GAD-7) scale, single-item sleep quality scale, questions on unavailability of personal protective equipment, training module on COVID-19 and change in orthopaedic patient management.
Results:
One hundred male orthopaedic surgeons responded to the survey with majority (79%) in 30–44 years age group. Severe anxiety scores were observed in 8%; moderate, mild and minimal anxiety was observed in 12%, 27% and 53% surgeons respectively. Changes in management practice due to the pandemic was admitted by 65% respondents. We also observed an association between higher anxiety among surgeons and primary or secondary level of healthcare facility: (p = 0.04). Sleep disturbance was significantly associated with change in management practice to non-operative procedures (p = 0.03).
Conclusion:
Anxiety among orthopaedic surgeons during the COVID-19 pandemic is related to factors like younger age group, working in a primary or secondary healthcare facility. Early recognition of anxiety is essential to prevent serious psychological sequelae.
Keywords
Introduction
The severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), is a newly discovered coronavirus (also called COVID-19) that has caused an unprecedented pandemic with clinical presentation ranging from asymptomatic state to rapidly progressive acute respiratory distress syndrome (ARDS) 1 creating a formidable global challenge requiring full focus and commitment from all governments, international institutions and organisations, the healthcare workforce, civil society as well as the general public.
Although the best defence against any pandemic is a strong health system, the fragility and inadequacy of the Indian public health system is well known and dependence on it would be imprudent when some of the best health systems in the world have been found to be grossly inadequate. 2 Large disparities continue to exist in India between rural and urban across social classes with overdependence on private healthcare providers. Healthcare workers (HCWs), both from private and public sector, have been at the forefront of the effort to control the spread of COVID-19 infection. The risk to own families, separation from families, strict isolation measures required, shortage of personal protective equipment (PPE), non-availability of essential equipment like ventilators as well as lack of clarity about pathogenesis, routes of transmission and treatment modalities for COVID-19 infection are potential risk factors leading to increased stress and disturbed sleep leading to a negative psychological impact on HCWs including orthopaedic surgeons. 3
This pandemic jeopardised working conditions resulting in anxiety among doctors in India who either had to close their private practice or wait for a safer environment conducive to elective surgical procedures. 4 With the clinical practice of orthopaedic surgeons being elective as well as emergency service based on the healthcare facility where one is working, a higher baseline rate of their burnout cannot be ruled out. 5 Past research studies provide evidence to support the high anxiety levels among HCWs 6 –9 including orthopaedic surgeons in India 10 and UK. 11 In order to assess the burden of anxiety among orthopaedic surgeons in India during this outbreak, a web-based cross-sectional survey using a seven-item Generalised Anxiety Disorder Scale (GAD-7) 12 was conducted. This is a novel study from India which assessed the burden of anxiety using a previously validated standardised questionnaire (GAD-7), sleep outcomes and the impact of unavailability of adequate PPE among orthopaedic surgeons during the COVID-19 pandemic. We hope that results from this study will enable hospital administrators and policy makers to identify and support individual surgeons at risk, implement appropriate measures for prevention of various possible risk factors and enable mitigating environment for effective regulation of emotions by at-risk surgeons.
Material and methods
Study design and participants
An online cross-sectional survey was carried out among the orthopaedic surgeons practising in India. The eligibility criteria for including the study participants was: (1) male and female orthopaedic surgeons who were involved in any kind of patient care to the patients, (2) residents of India, (3) working in private or public practice, (4) well versed in English language. Orthopaedic surgeons who did not provide voluntary informed consent to the study were excluded. All the participants were verified members of various online peer groups (Facebook and WhatsApp) of orthopaedic surgeons in India.
Sample and data collection
The sampling frame of our study included social media platforms: Facebook and WhatsApp. The sampling method was respondent-driven probability sampling based on social media’s peer network structure to encourage and recruit more respondents for the survey. The number of participants was based on the sample size calculation for cross-sectional studies 13 and past studies from the literature. 11 –14
This method drew on Facebook’s inherent peer network structures to encourage users to recruit other orthopaedic surgeons who may or may not be on Facebook. 15 Participants were invited through three online venues: public (‘wall’) posts advertising our research survey on some orthopaedic groups; peer referral on Facebook and WhatsApp group messages from 2 May to 16 May 2020.
The Facebook advertisement for our online survey included a headline describing the survey, and a brief scholarly review of the literature on the impact of COVID-19 on orthopaedic surgeons. For any further information about the survey, contact details of the principal investigator were mentioned in the advertisement. Moreover; there was an electronic link to the research questionnaire along with the time required to undertake the survey (approximately 5 minutes). A hyperlink to the survey was also shared through Facebook and WhatsApp.
The advertisement to participate in the survey was reposted every 3 days continuously for 2 weeks. This strategy resulted in the advertisement’s reappearance in users ‘News Feed’. Furthermore, we created a Facebook page to promote our research and sent out mass messages to the orthopaedic members of our Facebook page as well as personal messages via Facebook and WhatsApp to remind orthopaedic surgeons to participate in our survey.
Ethical statement
The study was approved by the institutional ethics committee of principle investigator’s institute (IES/2020/154). Voluntary participation after the informed written consent was declared in the advertisement. The information on the survey also highlighted that the participants would not be identified in the study and their responses would be anonymous. Thus confidentiality of the participants was fully respected. Participants had the right to withdraw from the study at any stage without any justification. There was no provision of incentives to our study participants. It was also declared that the survey responses would be stored on institutional OneDrive and would be password protected by the principal investigator of this study.
Survey questionnaire
The online survey was prepared on Google forms application and comprised of 20 compulsory questions with multiple choice options. We pilot tested our questionnaire on the first 10 respondents and their data has not been used in this study. The first seven questions were based on GAD-7 questionnaire. These questions assessed the frequency of anxiety symptoms over the past 2 weeks on a four-point Likert scale with assigned scores of 0, 1, 2, 3 to the response categories respectively of ‘not at all’, ‘several days’, ‘more than half the days’ and ‘nearly every day’. GAD-7 total score for the seven items ranged from 0 to 21 with increasing scores indicating more severe functional impairments as a result of anxiety. Scores of 5, 10 and 15 were taken as the cut-off points for mild, moderate and severe anxiety respectively 12 followed by screening questions for any depressive symptoms. Five questions were designed to assess the participant’s anxiety with regard to orthopaedic practice in COVID-19 environment and PPE (Personal Protective Equipment) for healthcare workers. The rest of the questionnaire obtained participants’ demographic information including age, gender, marital status, educational level, type of healthcare facility where employed and field of subspecialisation, if any.
Sleep quality
A single item previously validated sleep quality scale was used. 16 The effect on quality of sleep over last 7 days on a numerical scale of 0 to 10 was recorded.
There were five categories: 0 = terrible, 1–3 = poor, 4–6 = fair, 7–9 = good, 10 = excellent. When rating their sleep quality, participants were instructed to consider the core components of sleep quality including how many hours of sleep they had, how easily they fell asleep, how often they woke up during the night, how often they woke up earlier than they had to in the morning and how refreshing their sleep was.
Preparedness for COVID-19
The participants were questioned on whether they had attended any training module on management and preparation to tackle patients with COVID-19 pandemic.
Anxiety in professional patient related work
The participants’ anxiety on doing elective surgery currently and commencing the same after lockdown was recorded and any change in clinical management of certain fractures to ‘non-operative’ in prevailing COVID condition. The anxiety related to access to good quality PPE was recorded and the reluctance to perform patient care work if PPE is not available.
The online survey questionnaire is included as Appendix 1.
Statistical analysis
Descriptive analysis for demographic data and preparedness for COVID-19 related questions was performed. Multivariate regression analysis was used to correlate the factors influencing the prevalence of anxiety and sleep disturbance with age group, level of healthcare facility, subspecialisation and response related to PPE. The specific questions related to professional work change were correlated with GAD-7 score, age and field of specialisation. The data was analysed using SPSS software with p < 0.05 as statistically significant.
Results
Demographic characteristics
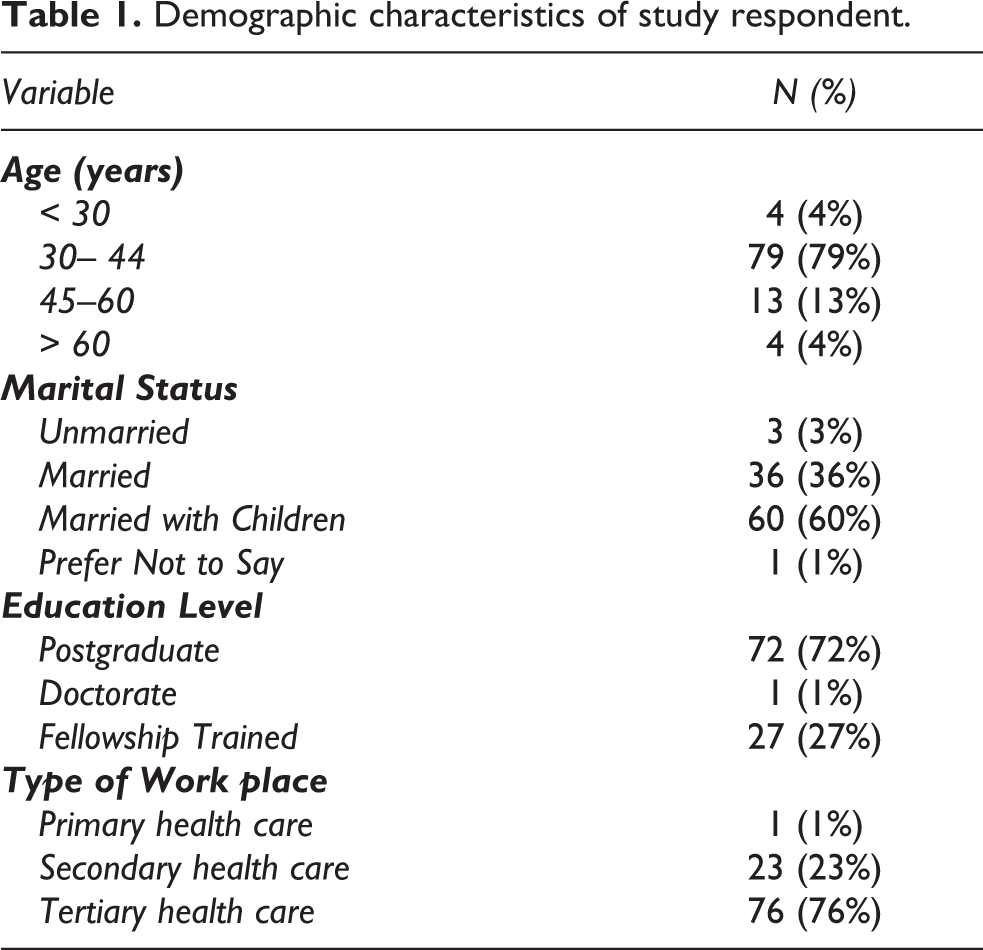
Table 1 shows the demographic characteristics of hundred male orthopaedic surgeons. Most participants were in the age group of 30–44 years (79%), married with children (60%) and were working in tertiary care hospitals (76%).
Demographic characteristics of study respondent.
There was a higher proportion of surgeons without availability of satisfactory PPE (42%) as compared to 26% respondents who had PPE available for work. Surprisingly, only 39% surgeons had attended a training module on COVID-19, as compared to 61% who had not attended any such training session (Table 2).
Linear regression analysis of factors affecting anxiety and sleep quality in Orthopaedic surgeons during COVID-19 pandemic.

Levels of anxiety and sleep disturbance among orthopaedic surgeons during COVID-19 pandemic
More than half of the participants (53%) had minimal anxiety scores in comparison with 8% surgeons with severe anxiety scores. The sleep quality was poor to fair in 30% surgeons and only 12% reported excellent sleep quality (Table 2).
Change in management practice and resuming elective orthopaedic surgery
Sixty-five per cent of respondents admitted to change of management of certain fractures such as fracture of tibia to non-operative; whereas 24% did not change their practice. Most of the surgeons (66%) were prepared to commence elective surgery, out of which 38% planned to commence elective surgery as per advice from professional bodies.
Factors affecting anxiety and sleep among orthopaedic surgeons during COVID-19 pandemic
Univariate analysis
Table 2 shows linear regression analysis of factors affecting anxiety and sleep quality in orthopaedic surgeons. Eight per cent of respondents had severe anxiety score >15 on GAD-7 scale, out of which 7% were in 30–44 years age group as compared to a higher percentage of minimal anxiety levels across all age groups. However, the overall correlation of anxiety with age group was not significant statistically (p = 0.91). Moderate and severe anxiety levels were observed in respondents who were married or married with children (13.9%, 5.6% and 11.7%, 10.0% respectively) without any significant correlation (p = 0.94). Fellowship trained surgeons had a higher proportion of minimal and mild anxiety levels (66.6% and 22.2% respectively) as compared to postgraduate surgeons who had a higher percentage of moderate and severe anxiety (15.3% and 8.3% respectively). There was no significant association between place of work, availability of PPE and prior training on COVID-19 with levels of anxiety. Although age did not have a statistically significant association with sleep quality (p = 0.09); it is notable that more than 25% of respondents in 30–44 years age group had poor to fair sleep scores.
Multivariate regression analysis. Table 3
shows the results of correlation analysis of variables affecting anxiety in orthopaedic surgeons. There was statistically significant association between higher anxiety levels among surgeons and working in primary or secondary level healthcare facility (p = 0.04).
Multivariate regression and correlation analysis of variables affecting anxiety in orthopaedic surgeons.

?Ref: Reference category.
Sleep disturbance was potentially associated with working in primary or secondary healthcare facility (p = 0.05); whereas it had no significant association with age, educational level, PPE availability and training on COVID-19 (Table 4).
Multivariate regression and correlation analysis of variables affecting sleep quality in orthopaedic surgeons.

?Ref: Reference category.
The questions related to change in management practice and resuming elective orthopaedic surgery and subspecialisation showed that sleep disturbance was significantly associated with change in management practice to non-operative procedures (p = 0.03). There was no significant correlation of response to resuming elective surgery, change to non-operative management and subspecialisation with anxiety levels and sleep disturbance (Tables 5 and 6).
Association of change in management practice and resuming elective orthopaedic surgery and subspecialisation with anxiety levels.

Association of change in management practice and resuming elective orthopaedic surgery and subspecialisation with sleep quality.

Discussion
This is the first online survey conducted on orthopaedic surgeons in India during the COVID-19 pandemic that highlights the potential burden of anxiety, sleep disturbance, inadequate availability of PPE, as well as the impact of any training module on management and preparation to face this pandemic.
Stress and anxiety among surgeons is not a new phenomenon 10,17 resulting in burnout 5 as well as suicide in extreme situations. 18 The sudden implementation of a nation-wide lockdown resulting in disruption of routine and elective surgical work may have been a significant stressor for our survey respondents. The correlation of higher anxiety and sleep disturbance in surgeons working in secondary and lower level of healthcare facilities, as in smaller cities or towns, points to the effect of pandemic induced lockdown on orthopaedic routine practice. This also highlights the presumed inadequacy of smaller centres and private clinics to monitor and implement safe practices in the wake of a pandemic.
There is ample evidence on ill-effects of a pandemic on mental health of general population 8,19,20 and the subset of HCWs in particular. Shanafelt et al. 21 have revealed the effects of such pandemics resulting in significant anxiety in health professionals and strategies to cope with them. The preparation to fight against the pandemic focuses on adequate training of HCWs and confidence building measures 21,22 for frontline workers in the form of training modules on COVID-19. Majority of the surgeons in our study (61%) reported to non-attendance in any training module that would have prepared them for the COVID-19 pandemic, bearing indirect effect on anxiety levels. As the pandemic evolves and intensifies further, a higher number of doctors and surgeons can be expected to suffer from anxiety and psychological impacts of being at the frontline, vulnerable and having a perceived lack of control. 6,23 –26
A major stressor that a HCW confronts is his or her own safety and family’s well-being. 21 This was evident in our study results showing higher anxiety levels in married surgeons as compared to unmarried surgeons, though not statistically significant. A recent survey conducted by University of Arkansas for Medical Sciences to assess and ensure well-being of their physicians revealed that the primary worry of all HCWs is the safety of their family in this pandemic. 27 The anxiety of threat to self, and indirectly their family, is also triggered by lack of adequate PPE and quality assurance. 28 Only 26% of respondents in our study reported access to good quality and adequate PPE, reflecting the role of this factor in contributing to anxiety and poor sleep quality.
The implementation of a strict lockdown and exponential increase in numbers of COVID-19 infections led to a paradigm shift in orthopaedic practice to predominantly trauma service as guidelines for a safe surgical practice continue to evolve. 29 One significant aspect of this is change in management of certain fractures to non-operative methods in the wake of high risks of operating on all such fractures with relative indications. This is highlighted in our study’s respondent group as 65% surgeons were sure of changing their management strategy to non-operative. The decision of government of India as well as majority of nations to gradually relax lockdown restrictions rekindled the hope of resuming routine surgical practice. However, there is evident anxiety with regard to taking a decision to resume elective surgeries as the surgeons were either not ready, confused or anxious (13%, 19%, 2% respectively). However, 38% surgeons in our study were inclined to follow advice of professional bodies that highlights the need for better communication and support system among our fraternity and mechanisms to mitigate stress. The economic burden of an intense lockdown on a surgeon can manifest with rising anxiety levels, primarily due to the impact on elective surgical practice that eventually culminates in reduced income, 30,31 occasionally predisposing the anxious surgeon to resume practice in an ill-prepared manner. The impact of fellowship training or a senior post is another significant stressor that remains inconclusive. Thakrar et al. 11 demonstrated a lesser level of psychological impact in associate consultants as compared to station health officer or other junior staff. The extrapolation of this scenario in the context of subspecialisation leading to minimal levels of anxiety remains to be proven, as in our study we did not observe any such significant association. However, the indirect assumption would be that subspecialised surgeons would be employed in a tertiary care facility with lesser chances of being out of work, economically drained or have minimal concerns of getting adequate PPE; as compared to working in a primary or secondary level healthcare facility which was associated with higher anxiety and poor sleep quality.
A major strength of our study is the use of the GAD-7 scale which is a standardised and validated tool for measuring anxiety in such cross-sectional surveys. 11,32 The restricted sample size of our study and the social media dependent sampling frame limits the representativeness of the sample; which may have influenced the results. Additionally, there is an apparent age bias in our study as 79% of respondents are in 30–44 years age group. This follows the universal trend of response in online surveys 33 where it has been shown that younger participants (up to 44 years) are more keen to take such online surveys as compared to those who are 45–54 years and older, who prefer other survey modalities such as mail (paper and pencil) survey.
Conclusion
This is the first survey in India to be conducted objectively with validated criteria like GAD-7 scale and sleep quality scale to assess the prevalence of anxiety among orthopaedic surgeons during the COVID-19 pandemic. This pandemic has impacted orthopaedic surgeons psychologically in the form of generalised anxiety that is related to factors like younger age group, working in a primary or secondary healthcare facility and unavailability of adequate PPE. The participating orthopaedic surgeons in this study admit to change in management practice to non-operative for certain fractures in wake of worsening risks of contracting the infection themselves. Furthermore, surgeons look forward to guidelines from professional bodies on crucial decisions like resuming elective operative work after lockdown. Early recognition of anxiety among orthopaedic surgeons is essential to avoid worsening the psychological impact of this evolving pandemic.
Supplemental material
Supplemental Material, sj-pdf-1-osj-10.1177_23094990211001621 - Impact of COVID-19 pandemic on orthopaedic surgeons in terms of anxiety, sleep outcomes and change in management practices: A cross-sectional study from India
Supplemental Material, sj-pdf-1-osj-10.1177_23094990211001621 for Impact of COVID-19 pandemic on orthopaedic surgeons in terms of anxiety, sleep outcomes and change in management practices: A cross-sectional study from India by Vyom Sharma, Narinder Kumar, Bhawna Gupta and Akanksha Mahajan in Journal of Orthopaedic Surgery
Footnotes
Acknowledgements
We are thankful to our participants for their time in responding to our survey.
Author contributions
VS, NK and BG designed and conducted the study. VS, NK, BG analysed the data. VS, NK, BG and AM drafted the manuscript. All authors have read and agreed to the drafted version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.