
Abstract
Objectives:
Effective implementation of prevention and control actions by health professionals is substantial to contain the deadly COVID-19 pandemic. Thus, this study aimed to assess health care worker’s practice of using personal protective equipment and psychological preparedness against the COVID-19 pandemic in Eastern Ethiopia.
Methods:
A facility-based cross-sectional study design was used. The health care workers (HCW) who were working in the selected health facilities were randomly selected. Variables that had p-value of < 0.15 were transformed to multivariable logistic regression model. Finally, the significance level was declared at the p-value < 0.05 with a 95% confidence interval (CI).
Results:
A total of 418 HCWs were randomly selected and included in this study. The study participants mean age was 27.96 years with a ±5.6SD. HCWs who were male (adjusted odds ratio(AOR) = 2.21, 95% CI: 1.29–3.79), regularly using sanitizer, accessing COVID-19 management guideline (AOR = 2.83, 95% CI: 1.46–5.47), trained on COVID-19 prevention methods (AOR = 2.6, 95% CI: 1.4–4.7), hopeless of eventually getting COVID-19 at workplace (AOR = 1.9, 95% CI: 1.13–3.28), and feeling unsafe at work when using standard precautions (AOR = 0.46, 95% CI: 0.27–0.79) were associated with good PPE using compared to their counterparts. Moreover, nursing/midwifery professionals practiced good personal protective equipment compared to physicians (AOR = 3.7, 95% CI: 1.8–7.7).
Conclusion:
The study demonstrated that being a male, being a nurse/midwifery, regularly sanitizing hands/medical equipment, having COVID-19 management guidelines, trained on COVID-19, and feeling of eventually getting COVID-19 at workplace had a positive association with PPE utilization. Besides, the study revealed that not feeling safe at work when using standard precautions was negatively associated with PPE utilization of HCWs. Therefore, the prevention priorities should be given to frontline HCWs by providing all possible support and strictly implementing the prevention and control guidelines of COVID-19 to prevent the health system from collapse.
Keywords
Introduction
Coronavirus disease infection that is caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) has become a global health threat with 159,319,384 confirmed cases and 3,311,780 deaths. 1 The new SARS-CoV-2 has now spread to 222 countries. 2 Controlling the spread of the disease and providing medical care to infected patients has been an unprecedented challenge. With health care systems under pressure to limit the spread of the novel coronavirus, a big part of this responsibility has been shouldered by health care workers (HCW). Hence, HCWs are part of the population segment who are inevitably at risk of getting the infection; 570,000 infected and 2500 died in the Americas, 3 and more than 10,000 HCWs were infected in Africa. 4
Due to its high transmission rate, morbidity, and mortality, appropriate methods of donning and doffing personal protective equipment (PPE) according to infection prevention and control guidelines are important to protect HCWs, patients, and their families from inadvertent exposure to COVID-19. Adequate PPE is a central component of infection prevention control (IPC) and of paramount importance in the fight against COVID-19. 5 In Ethiopia, where there is a shortage of human power and PPE, the pandemic is terrifically rising; 264,960 confirmed cases and 3951 deaths. 6 The lack of awareness and training about the basic concept of PPE use may complicate the PPE using–related gaps.7,8 Since pandemics are often unpredictable, along with mitigation and suppression strategies, health systems and, in particular, the preparedness of HCWs to respond to pandemics are critical to containing disease spread.9–11 However, low-resource countries like Ethiopia were experiencing multilevel barriers to preparedness due to limited resources and weak health care infrastructure.12,13 HCWs’ inadequate preparedness (24%–57%) 14 to respond to an outbreak contributes to workers leaving their positions due to fear of infection and community distrust of government and HCWs.15–17 Being a nurse, female, having an isolated ward, knowing COVID-19 management, good communication with management, and work experience >10 years had association with the PPE utilization. 14
Many studies revealed that COVID-19 spread caused excessive hospital overload, a shortage of health care resources, workload for professionals, fear of transmission, burnout, and the scarcity of face masks, sanitizers, and gloves that may cause a further barrier communication and expressing compassion.18–24 Owing to the heavy workload at the forefront and discomfort from wearing PPE for long periods, nurses in especially high-workload departments such as the emergency department have been suffering from considerable short- and long-term mental health problem burdens.25–28 The psychological problem is the major outcome for staff providing health care amid the COVID-19 pandemic presenting with depression, anxiety, insomnia, and general psychological distress.29–37 Educational level, increased workload, age 20–40 years, working at emergency unit, insufficient precaution measures, being a nurse, female, and direct contact with patients were associated with psychological distress.12,25,31,32 The studies also revealed that COVID-19 impacts were manifested by the poor mental health status of health professionals such as the feeling of loneliness, depression, anxiety, and sleep disturbance.38,39
The purpose of this study is quite important to assess the availability of PPE in the health facilities, HCWs’ practice of using PPE, and level of psychological preparedness to stop the further spread of the pandemic among HCW and between HCWs and the patients. Therefore, this study aimed to assess the PPE utilization practice and psychological preparedness among HCWs against the COVID-19 pandemic in Eastern Ethiopia.
Methods and materials
Study design, area, and period
This study was conducted among HCWs working in the Harari region and East Hararghe Zone using a facility-based cross-sectional study design from 21 August to 5 September 2020. The Harari regional state Health service coverage is 100%. Harari region contains three government hospitals (two public hospitals and one police hospital), two private hospitals, and one non-government hospital (Fistula Center). East Hararghe zone contains five hospitals and 67 health centers. Of these health facilities, two hospitals and six health centers are on the main road to Addis Ababa, the capital city of Ethiopia.
Population eligibility criteria
All the health facilities and HCWs in Harari Region and Oromia region East Hararghe zone were the target population. Based on their risk of encountering the disease, the health facilities immediate to the main road to the capital city of Ethiopia were purposively selected. Then, health care professionals who were working in the selected health facilities were selected randomly. The HCWs who were not available due to sickness, personal affairs, and facility’s duty were excluded from the study.
Sample size determination, sampling technique, and sampling procedures
A sample size was determined by using single proportion population with p = 0.5(no prior data from the study area), z = 95% confidence interval (CI), margin of error (d) = 0.05, n = (zα2)2pq / d2 = (1.96)2 (0.5)(0.5) / (0.05)2, n = 384. By considering 10% non-response rate, the final sample size was determined to be 418. Thus, 418 frontline HCWs were included in the study (Figure 1).

Schematic presentation of health workers selection of the study in Harari region and Eastern Hararghe Zone, 2020.
Data collection methods
Fifteen BSc health professionals were involved in the data collection. Also, three public health professionals were assigned to supervise. They started the data collection processes after taking 2 days of training from the principal investigator on the objective, relevance of the study, and technique of interview with demonstration. The questionnaires included socio-demographics: profession, types of health facility, HCW experiences, types of the health facilities, availability of PPE, utilization of PPE, HCWs’ awareness, sources of information, and psychological preparedness toward COVID-19 developed from different literature. The participant information was kept confidential. Health professionals were provided with questionnaires asking the basics of COVID-19 pandemic preparedness.
Study variables and measurements
PPE using practice was the outcome variable of this study. Independent variables included socio-demographic characteristics, profession, types of health facility, HCW experiences, training on COVID-19, availability of PPE, availability of case definition for COVID-19, and psychological preparedness–related characteristics. The PPE utilization was assessed with a set of nine questions. Regarding the HCWs’ psychological preparedness, the Likert-type scale consisting of two grades of responses (agree vs disagree) was used.
Operational definition
The PPE using practice was scored “good” when the health care professionals’ PPE using scores were 5–9 on PPE practice–related questions, scored “poor” when scores were 0–4 out of a total of nine PPE using–related questions.
Data quality control
A tool was developed from different literatures; especially the COVID-19 management protocol manual of Ethiopia was used (suplementary 1). Moreover, the tool was pretested on non-selected health facilities’ health care providers. Finally, a valid pretested questioner was distributed to collect the actual data from randomly selected HCWs.40–42 There was intensive training involving all tools of data collection, which also had practical sessions. All data collectors and supervisors took 4 days of theoretical and 2 days of practical training. Data quality was kept by checking for consistency, completeness, and accuracy manually during data collection time.
Pretest was done on 5% of study participants in a non-selected health facility.
Statistical analysis
Data were entered in Epi-data 3.1 version and exported into and analyzed by SPSS 23 version. Descriptive statistical methods such as central tendency and measures of dispersions are done to summarize the data. The PPE utilization status was dichotomized into good versus poor. The HCWs’ psychological preparedness questions were categorized into two grades of responses (agree vs disagree). The binary logistic regression was performed to identify the association between PPE utilization practice (good or poor) and independent variables, including psychological preparedness of HCWs. Odds ratio (OR) is used to determine the strength and direction of the association between the outcome and independent factors. Finally, the significance level was reported at the p-value < 0.05 at a 95% confidence interval.
Ethical statement
Haramaya University College of Health and Medical Sciences Institutional Health Research Ethical Review Committee (IHRERC) ethically cleared the project (protocol code: IHRERC/189/2020 and date of approval: 19 August 2020). The college of Health and Medical Sciences sent a letter of cooperation to local authorities and health facilities. Before obtaining the information, a participant/head of the institutions was asked to give a written, informed voluntary, and signed consent. Finally, all randomly selected HCWs were informed and signed written consent voluntarily. The study participant’s information was collected anonymously guaranteeing information confidentiality. The data collection process was conducted as per the Declaration of Helsinki.
Results
Socio-demographic characteristics
A total of 418 study participants were included in this study. The mean age of the study participants was 27.96 years with a ±5.6 standard deviation. Of the total HCWs who participated in this study, 258 (61.1%) were from the hospitals, and 160 (38.9%) were from health centers. The median experience of the study participants was 3 years with the inter-quartile range (IQR) of 2–6 years. Of a total of 418 participants, 196 (46.4%) were Muslims, (53.1%) were single in marital status, 117 (28.2%) were working in the inpatient departments, (58.6%) of them were bachelor’s degree holders, and professionally 193 (46.2%) of them were nurses (Table 1).
Socio-demographic characteristics of the health care professionals working in Harari region and East Hararghe zone health facilities from August to September 2020.
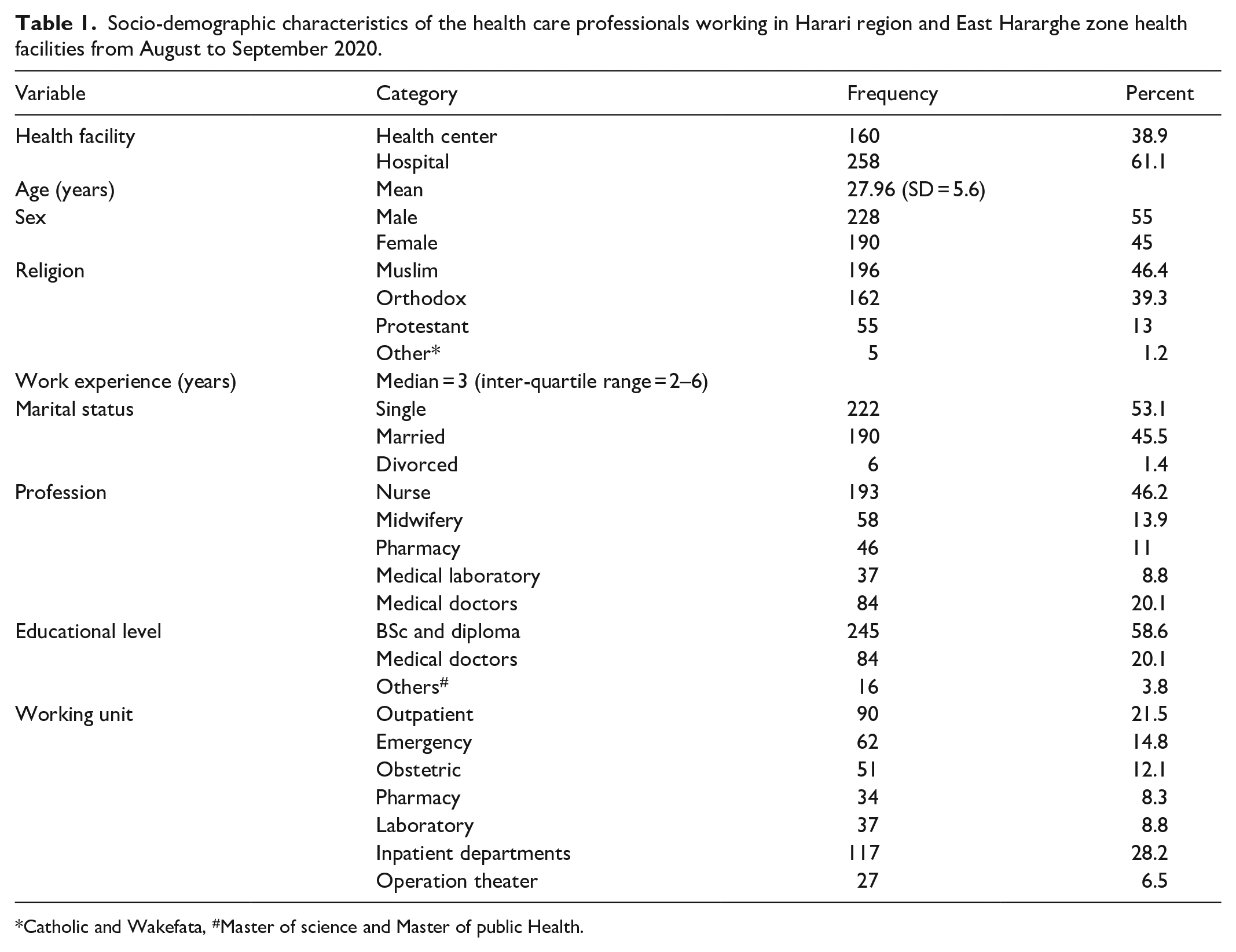
Catholic and Wakefata, #Master of science and Master of public Health.
Availability and practice of using PPE
Among a total of 418 HCWs, 261 (62.4%) practiced PPE use poorly, while the rest 157 (37.6%) had good practice of PPE use. Regarding PPE use, eye goggle, face mask, glove, apron, shoes, and other PPE were used by 122 (29.2%), 369 (88.3%), 230 (55%), 81 (19.4%), 76 (18.2%), and 29(6.9%) of HCWs, respectively. Each national guideline and booklet of COVID-19 was supplied to 269 (64.3%) of the HCWs. Moreover, about 259 (62%) workers received training on COVID-19 infection prevention and controls (Table 2).
PPE availability in Harari region and East Hararghe zone health facilities from August to September 2020.
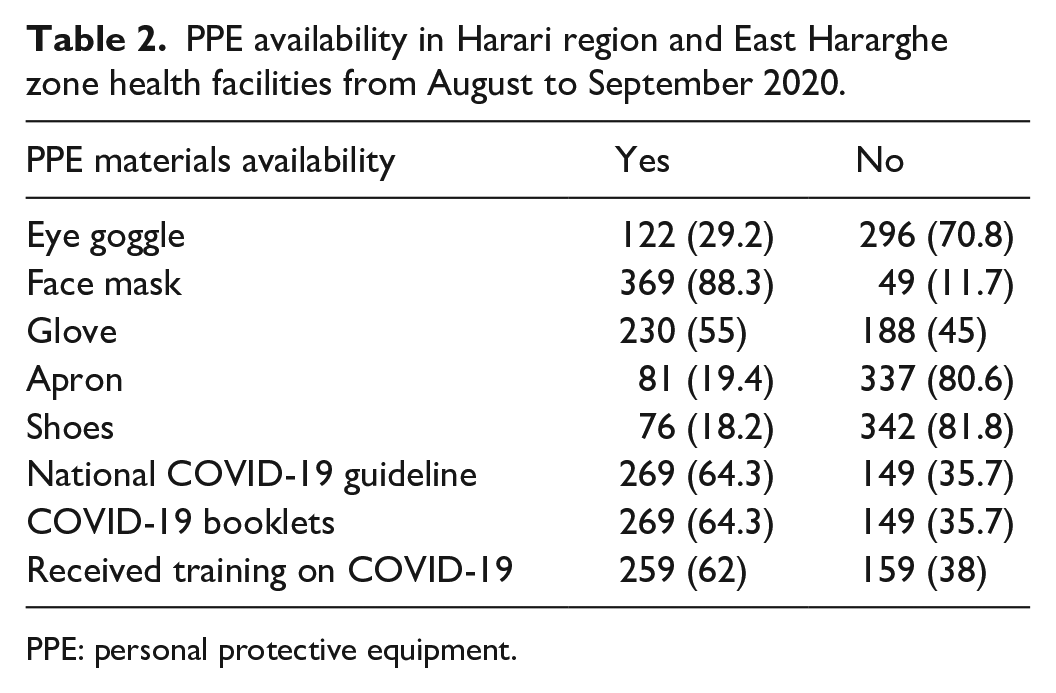
PPE: personal protective equipment.
Regarding the ways of COVID-19 prevention, hand hygiene, wearing a face mask, avoiding contact with an infected person, and avoid attending overcrowding areas were reported by 319 (76.3%), 330 (78.9%), 234 (56%), and 222 (53.1%) HCWs, respectively. While performing CPR for COVID-19 patients, 181 (43.3%), 155 (37.1%), and 104 (24.9) of the HCWs believed that getting rid of disposable equipment, removing PPE, and rubbish double-bagged should be taken into consideration. Safety measures that the participants practiced during work were sanitizing phone, stethoscope, badge, bed, and room (255, 61%); hand washing/hygiene before and after dealing with every patient (291, 69.6%); avoiding handshake (222, 53.1%); always wearing appropriate PPE when indicated (223, 53.2%), respectively. Also, safety measures such as washing bag, clothes, and sanitize staff (255, 61%); leaving shoes at work or outside of home (198, 47.4%); taking bath immediately at home (176, 42.1%); and doing any sports activity (95, 23%) were practiced by HCWs after finishing work, respectively (Table 3).
COVID-19 prevention practices among health care professionals working in Harari region and East Hararghe zone health facilities from August to September 2020.
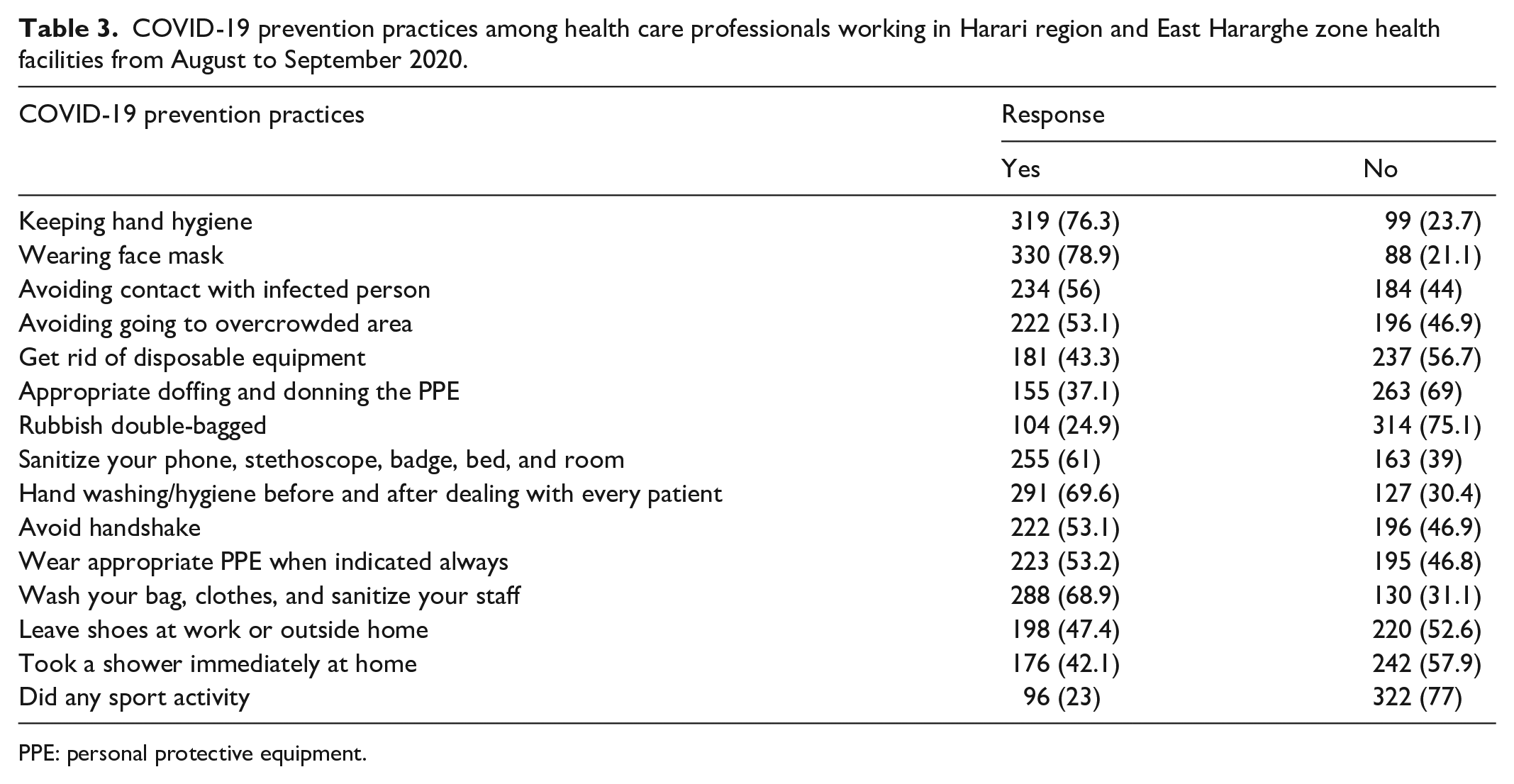
PPE: personal protective equipment.
Health care providers’ level of psychological preparedness against COVID-19 pandemic
Among a total of 418 HCWs, 225 (61%) felt anxious when treating any febrile patients. Nearly half of the HCWs felt that their working place is not safe from contracting COVID-19. Nearly two-thirds of HCWs agreed that they had a high risk of contracting COVID-19 and were obliged to provide care for COVID-19 infected patients. Half of the participants, 210 (50.2%), felt hopeless about eventually getting COVID-19 at work. Nearly half of the participants agreed that they did not feel confident to get employees’ care if they get COVID-19 (Table 4).
Psychological preparedness against COVID-19 pandemic among health care professionals working in Harari region and East Hararghe zone health facilities from August to September 2020.

Factors associated with practices of PPE use
Variables that had a p-value less than 0.15 were transformed to multivariable logistic regression. In multivariable logistic regression, independent variables such as gender, profession, accessing national COVID-19 management guidelines, receiving training targeted to COVID-19 prevention methods, sanitizing medical equipment regularly, feeling hopeless of eventually getting COVID-19 at work, and feeling safe at work when using standard precautions had a statistically significant association with PPE use practice (p < 0.05)
In this study, odds of using PPE were higher among male HCWs 2.21 times more likely than females (AOR = 2.21, 95% CI: 1.29–3.79). HCWs who were nursing/midwifery professionals had good PPE using practice 3.7 times more likely than physicians (AOR = 3.7, 95% CI: 1.8–7.7). HCWs who accessed a national COVID-19 management guideline practiced good PPE using skills were 2.8 times more likely than their counterparts (AOR = 2.83, 95% CI: 1.46–5.47). HCWs who received training targeted to COVID-19 prevention methods had 2.6 times more likely than those who did not take the training (AOR = 2.6, 95% CI: 1.4–4.7). Health professionals who regularly practiced the sanitizing of phone, stethoscope, badge, bed, and room had good PPE using skill 6.16 times more likely than their counterparts (AOR = 6.16; 95% CI: 3.32–11.4).
The HCWs who felt hopeless of eventually getting COVID-19 at work were 1.9 times more likely than their counterparts (AOR = 1.9, 95% CI: 1.13–3.28). Moreover, the study participants who did not feel safe at work when using standard precautions practiced PPE using by 54% less likely compared to those who felt safe when using standard precautions (AOR = 0.46, 95% CI: 0.27–0.79) (Table 5).
Factors associated with PPE utilization practice among health care professionals working in Harari region and East Hararghe zone health facilities from August to September 2020.

COR: Crude Odds Ratio; PPE: personal protective equipment; AOR: adjusted odds ratio.
Discussion
The contagiousness characteristic of COVID-19 makes its prevention and control challenging both in developed and developing countries, including Ethiopia. Moreover, a very swift contagion of the viruses diffused over 220 countries, including Ethiopia causing more than 161 million cases and 3.5 million deaths within a period of less than 1 year.
This study revealed that HCWs practiced different types of PPE during the COVID-19 pandemic; 369 (88.3%) used face masks, 230 (55%) gloves, 122 (29.2%) eye goggles, 81 (19.4) apron, and 76 (18.2) shoes, respectively. This was higher than a study finding in North Shewa which showed that health care providers used face mask (27.4%), gloves (31%), goggles (15.9%), apron (14.2%), and shoes (11.5%). 13 This difference could be due to the time elapsed and variation of the geographical distribution of COVID-19; the present study was conducted among HCWs working in health facilities found on main roads to the capital city of Ethiopia. However, it was lower than a study conducted in Northwest Ethiopia, 140 (93.3%) goggles. 43 Also, it was lower than a study conducted in Latin America where (91.1%) gloves and (67.3%) gowns were practiced, respectively. 44 This discrepancy might be related to less accessibility of information, and less availability and accessibility of PPE in low-income countries like Ethiopia. In addition, the variation of PPE items used from setups to another setup can be due to the possibilities of using different types of PPE recommendations by Centers for Disease Control and Prevention/World Health Organization (CDC/WHO). 45
This study revealed that being a male HCW was two times more likely to have a good practice of PPE than females. The finding is comparable with a report from Debre Tabor. 46 Since COVID-19 morbidity and mortality were higher among males, males may be alert about the risk of contracting the disease. Thus, they might practice PPE utilization than females. Moreover, the majority of COVID-19-related deaths are caused by male-exercised behaviors than women. For instance, a higher level of smoking and drinking among men than women may cause the difference.47,48 Therefore, this burden of COVID-19 among males may cause significant differences in the prevention practices.
Nurses/midwives had practiced good PPE using 3.7 times more likely compared to physicians. This finding is in line with the studies conducted in Nigeria and Ghana.14,49 It might be due to that nurses/midwives are relatively more exposed to infectious diseases as they stay longer with the patients. Hence, HCWs should be reinforced and supported by health institutions for addressing their PPE needs.50–54
HCWs who had a national COVID-19 management guideline were almost three times more likely to have a good practice of PPE use. This report is supported by the studies conducted in Northwest Ethiopia, 43 Amhara, 55 and Bangladesh. 41 The National management guideline reminds and guides HCWs about preventive mechanisms and how to apply them to prevent infections at working places and accessing the required infection prevention equipment. If HCWs have infection prevention guidelines and know the risk of not practicing preventive strategies, they will apply all the possible preventive mechanisms to avoid infections.42,56
HCWs who received COVID-19 infection prevention and control training had a higher rate of good PPE using skills. HCWs who are well-informed about the severity of the pandemic are more likely to adhere to infection prevention methods like PPE use. Regular updating of HCW’s skills and availing infection prevention and control guidelines through training are important.50,57–59
Participants who felt COVID-19 transmission at work were two times more likely to have a good practice of PPE use. This may be due to high accidental exposure of HCWs to droplets during close contact to treat COVID-19 patients. COVID-19 highlights the need to address occupational health and safety within health facilities, including through adequate resourcing and appointing implementation focal points to enable regular assessment and control of occupational health and safety hazards, and medical surveillance of health workers.
Participants who agree with not feeling safe at work when they use the standard precautions were 38.7% less likely to have a good practice of PPE. This is supported by a study done in Northwest Ethiopia 56 and Bangladesh. 38 It needs facility leaders to provide training for HCWs regarding the strategies and advantages of obeying infection prevention and control. This study could reveal the HCWs’ preparedness level through a face-to-face interview that might minimize the inaccuracy of information from web-based online data collection methods compared to the previous studies. Besides, the randomness of subjects’ enrollment may also enable the finding to be generalized for HCW providing services in other similar health facilities. Even though this study has its strength, it is not without limitations. Purposive selection of health facilities on the main road to the capital city (Addis Ababa) may affect the representativeness of findings. Despite that the subjects were pleased to be genuine and assured their responses were anonymous, we suspected that the information from the self-report may not always unveil the actual activities of the respondents.
Conclusion
The study demonstrated that being a male, being a nurse/midwifery professional, regularly sanitizing hands/medical equipment, having national COVID-19 management guidelines, taking COVID-19 training, and feeling of eventually getting COVID-19 at the workplace had a positive association with PPE utilization. Besides, the study revealed that not feeling safe at work when using standard precautions was negatively associated with PPE utilization of the HCW. The prevention strategies and measurements should be strictly followed and implemented on the COVID-19 high-risk professionals like HCWs. Therefore, the government needs to strengthen the efforts of mobilizing the stakeholders, and upbeat the prevention practices of the HCWs through different communication forms by enforcing already stated rules and making them strict, especially in all health facilities preventing the health system from collapsing and tackling the virus’s transmission from the community at large.
Supplemental Material
sj-docx-1-smo-10.1177_20503121211051925 – Supplemental material for Personal protective equipment utilization practice and psychological preparedness of health care workers against COVID-19 pandemic in Eastern Ethiopia
Supplemental material, sj-docx-1-smo-10.1177_20503121211051925 for Personal protective equipment utilization practice and psychological preparedness of health care workers against COVID-19 pandemic in Eastern Ethiopia by Abdi Birhanu, Bikila Balis, Tesfaye Assebe Yadeta and Miesso Bayu in SAGE Open Medicine
Footnotes
Acknowledgements
We gratefully acknowledge Haramaya University College of Health and Medical Sciences for the financial support of this project. We would also like to thank all study health facilities for their assistance and help in facilitating the data collection. Finally, our gratitude goes to our study participants, data collectors, and supervisors for their commitment throughout the data collection process.
Author contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the manuscript is submitted; and agree to be accountable for all aspects of the work.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded by Haramaya University.
Data availability
The data used to support the findings of this study are available from A.B. upon reasonable request.
Ethics approval
Ethical approval for this study was obtained from Haramaya University College of Health and Medical Sciences Institutional Review Board (or Ethics Committee) (protocol code: IHRERC/189/2020 and date of approval: 19 August 2020).
Informed consent
Written informed consent was obtained from all subjects before the study.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.