
Abstract
Aeromonas hydrophilia can cause soft tissue infection in both immunocompromised and healthy persons. A healthy 15-year-old adolescent fell into a ditch after a scooter accident and sustained a right distal tibial shaft closed fracture, a right femoral shaft closed fracture, and a dirty laceration over the medial aspect of the distal thigh above the right knee. After empiric antibiotics and radical debridement of the contaminated wound, a femoral interlocking nail and tibial external fixator were applied. However, acute osteomyelitis later presented in his femur and tibia, and Aeromonas hydrophilia grew in cultures from the knee wound and the fracture sites. During the follow-up, his tibia became an infected nonunion, and was successfully treated with the induced membrane technique. In an otherwise healthy patient with a closed fracture, Aeromonas hydrophilia can cause acute osteomyelitis and necrotizing fasciitis by spreading from a nearby contaminated wound. Exposure to water is a risk factor for Aeromonas hydrophilia infection.
Introduction
Aeromonas hydrophilia causes soft tissue infection in both immunocompromised and healthy individuals, and related severe infections including necrotizing fasciitis and osteomyelitis in healthy people were reported. 1 –6 Acute osteomyelitis after a closed fracture is rare and has been reported as a hematogenous infection in the literature. 7,8 First, we report a healthy adolescent who developed acute osteomyelitis and necrotizing fasciitis at his tibial and femoral closed fracture sites as Aeromonas hydrophilia spread from a laceration wound around his knee via local soft tissue. The tibial fracture eventually progressed into an infective nonunion and was successfully treated with the induced membrane technique. Second, we reviewed the literature associated with Aeromonas hydrophilia-induced necrotizing fasciitis and/or acute osteomyelitis in patients with fractures. Written informed consent was obtained from the patient and his mother for the publication of this report and any accompanying images.
Case report
A previously healthy 15-year-old adolescent had an accident while riding a scooter and fell into a ditch. He presented at our emergency department with stable vital signs and multiple injuries: a grade II liver laceration, a right lung contusion with hemo-/pneumo-thorax and fourth to fifth rib fractures, a right femoral shaft fracture (AO A3), a right distal tibial fracture (AO A2) with lateral malleolar fracture (AO C2), and a deep and dirty laceration over the medial aspect of the distal thigh above the right knee, but without communication into the knee joint (Figure 1). All fractures were closed fractures, as there was no communication between the laceration wound and the fractures. After initial surveys and managements (including insertion of a chest tube, wound irrigation and coverage with wet dressing, and empiric intravenous cefazolin), he was taken to the operating room for radical debridement of the dirty laceration around his right knee and fracture fixation 5.5 hours after the accident. Marginal excision of the contaminated skin, subcutaneous fat, and fascia, followed by copious lavage with large volume of saline, the laceration was left open and temporarily isolated with wet gauze covered by a Tegaderm transparent dressing (3M, St Paul, MN, U.S.A.). To avoid cross contamination between the fracture fixation and the debridement of the dirty laceration, re-scrubbing, re-gowning, re-disinfection, and re-draping were ensured. Under the concept of damage-control orthopedic surgery, closed reduction and internal fixation with a reamed antegrade interlocking nail for his right femur and an external skeletal fixator (ESF) for his right tibia were performed later with a new set of instruments. The surgery lasted for 2.5 hours, and the laceration was covered with wet dressing at the end of the surgery. He was then transferred to the intensive care unit for further care, and experienced intermittent high fever and tachycardia after the initial operation. The wound cultures of his medial aspect of the distal thigh laceration showed Aeromonas hydrophilia 2 days later, but his blood culture reports were negative; his antibiotics were then shifted to ciprofloxacin with gentamycin according to the susceptibility test. The dirty wound around the knee showed turbid discharge during wet dressing care after the initial operation. On day 4, remarkable skin erythema and swelling were observed in the lateral thigh around the femur fracture site and in the anterior leg around the tibia fracture site. Therefore, debridement for the dirty laceration around the right knee, and the erythematous areas of the right thigh and leg were performed on day 5. Necrotizing fasciitis with pus accumulation presented on the leg over the tibial fracture site and on the thigh over the femoral fracture site. Cultures from the fracture sites matched previously cultured Aeromonas hydrophilia. In response, the femoral nail was replaced with an ESF, and all debrided wounds were treated openly. After repeated debridements, the local condition improved with well-granulated tissue, from which follow-up cultures revealed eradication of Aeromonas hydrophilia. Because the clinical findings indicated that the infection was well-controlled, osteosynthesis using plates for the femur via the previous lateral approach for debridement and lateral malleolus via the direct lateral approach from the healthy skin were performed on day 24. Three days later, split-thickness skin grafts were performed for coverage of the debridement wounds in the lateral thigh and anterolateral leg, as well as the laceration wound around the knee. All skin grafts took well. However, on day 31, a discharge sinus showed on the medial aspect of the leg over the tibia fracture site. Meanwhile, the other post-skin-graft wounds healed without any signs of infection. The tibia ESF was kept due to the exposed bone and the poor local soft tissue condition further infected by oxacillin-resistant Staphylococcus aureus (ORSA) and Escherichia coli with extended-spectrum β-lactamase (ESBL). After serial debridements and prolonged intravenous antibiotic treatment, the tibial fracture was successfully covered with an ipsilateral free gracilis myocutaneous flap after the local muscle flap and the ipsilateral free sartorius flap failed. The patient was discharged on day 92 and prescribed oral antibiotics. During the follow-up, a discharge sinus tract over the thigh scar was noted. Debridement, plate removal, and ESF application were performed due to the delayed union of the femur on day 194 and the intraoperative culture showing Bacteroides fragilis. Following the prolonged oral antibiotics treatment, the femur and lateral malleolus eventually united (Figure 2). However, for the tibia, there remained evidence of nonunion on the plain film plain films, and two episodes of recurrent discharge sinus occurred over the previously healed scar of the flap. An osteomyelitis scan suggested chronic osteomyelitis of the tibia, which was compatible with the clinical findings. Radical debridement and reconstruction were strongly recommended, but the patient refused.
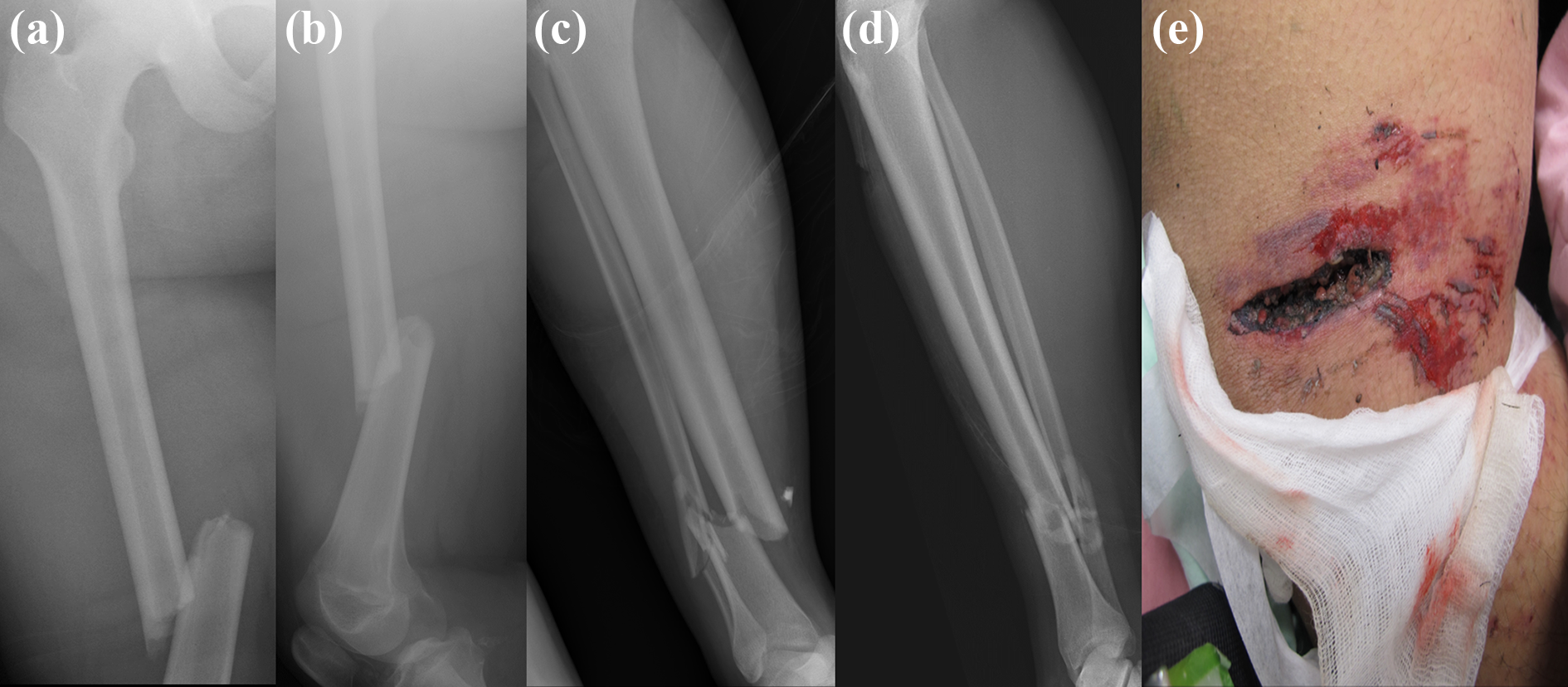
An otherwise healthy 15-year-old adolescent had a motorcycle collision, fell into a ditch, and sustained multiple traumas. Radiographs showed a right femoral shaft fracture, an AO/OTA A3 type ((a) and (b)), and a right distal tibial shaft fracture, an AO/OTA A2 type, with lateral malleolar fracture, an AO/OTA C2 type ((c) and (d)). All fractures were closed. There was a deep, dirty laceration over the right medial knee but no communication into the knee joint (e).

The right femur united ((a) and (b)) 20 months post-injury. The distal tibia still showed infected nonunion and bone defects ((c) and (d)).
On day 619, he agreed to undergo surgery for the prolonged infected nonunion of his right tibia (Figure 2(c) and (d)), for which we used the induced membrane (IM) technique. In the first stage (Figure 3(a) and (b)), radical debridement was performed until the paprika sign showed. A gentamycin- and vancomycin-impregnated polymethyl-methacrylate bone cement spacer was placed in the 4-cm bone defect, and 2 cm of both ends of the tibia were wrapped to create a better IM envelope. 9 The ESF was kept with a change of Schanz screw configuration. Because of the same ORSA and E. coli pathogen in the intraoperative culture, the fusidic-acid, trimethoprim, and sulfamethoxazole oral antibiotics were kept. The level of C-reactive protein gradually decreased and became stationary but mildly elevated (10.6–17.0 mg/L) 4 weeks after the first stage surgery. The second stage procedure was conducted 12 weeks after the first stage. The IM envelope formed well in the second stage, and the bone bled well at both ends after the spacer was removed. The cancellous bone graft was composed of 75% autologously harvested bone from the right iliac crest and 25% allogenously harvested bone. The antibiotic treatment was halted because the intraoperative culture during the second stage showed no pathogens. Touch weight-bearing was suggested for the first 6 weeks after grafting, after which protected weight-bearing was permitted. Radiographs 5 months post-graft showed good bone consolidation and bridging union (Figure 3(c) and (d)). Pain-free full weight-bearing was then achieved, after which the ESF was removed. There was no re-fracture or infection flare-up after the 2-year follow-up (Supplementary Figure & Video).

The first-stage of the induced membrane (IM) technique was done for the distal tibia on day 619 ((a) and (b)). Bone graft consolidation and bridging union occurred 5 months after the second-stage bone graft procedure ((c) and (d)).
Discussion and conclusions
Aeromonas hydrophilia is a motile gram-negative bacillus with polar flagella, and is frequently found in aquatic environments and creatures. In humans, Aeromonas hydrophilia primarily cause gastrointestinal tract infections followed by soft tissue infections. Aeromonas hydrophilia occasionally causes necrotizing fasciitis in immunocompromised individuals, which rapidly progresses with a reported mortality rate of 60–75%. 10 Related necrotizing fasciitis in healthy individuals have been reported recently (Table 1), 1 –6 and may lead to amputation due to unreconstructable soft tissue defects. 1,2,4,6 Wounds exposed to a moist environment carry the risk of Aeromonas hydrophilia infection. 11 Therefore, in our practice, an open fracture with exposure to water is managed with an external fixator, broad-spectrum empiric antibiotics, and urgent, thorough debridement. If there are signs of rapid progressive soft tissue infection, Aeromonas hydrophilia should be considered as one of the possible leading pathogens. Third or fourth generation cephalosporin in combination with a tetracycline or gentamicin, piperacillin-tazobactam, or fluoroquinolone are choices of empiric antibiotics for suspicious Aeromonas hydrophilia soft tissue infection, 12 while a susceptibility test for all Aeromonas isolates is highly recommended as their potential of resistance to ESBLs, AmpC cephalosporinases, carbapenemases, and ciprofloxacin. 12 –16 As the laceration wound was exposed to ditch water in our case, initial empiric antibiotic with cefazolin alone was inadequate to prevent possible Aeromonas hydrophilia soft tissue infection. With respect to Aeromonas hydrophilia leading to necrotizing fasciitis in a patient with a closed fracture, only one case was reported by Abuhammour et al. in the literature. A healthy adolescent presented a closed tibial fracture with local minimal abrasions in a muddy field, which further developed Aeromonas hydrophilia-induced necrotizing fasciitis. 5 Local spreading of Aeromonas hydrophilia from minimal abrasions is highly suspected in this case. In our case, the skin around the tibial and femoral fracture sites was intact. The deep and dirty laceration over the ipsilateral medial knee, exposed to ditch water, is strongly suspected to be the source of the local infection of Aeromonas hydrophilia, as verified by culturing. According to Abuhammour et al.’s and our cases, even in closed fractures, Aeromonas hydrophilia may lead to necrotizing fasciitis, and even acute osteomyelitis, via local minimal abrasion or a nearby contaminated wound exposed to a moist environment.
Literature review on Aeromonas hydrophilia-induced necrotizing fasciitis and/or osteomyelitis in patients with fractures. All listed cases had no reported systemic disease, except the case reported by Hong et al., in which the patient had alcoholic liver cirrhosis.

N.M., Water exposure history was not mentioned in the literature; IM, induced membrane; NF, necrotizing fasciitis; OM, osteomyelitis; LSTS, local soft tissue spreading; BSS, blood stream spreading; AKA, above-knee amputation; BKA, bellow-knee amputation; EF, external fixator.
* The Gustilo classification of the open fracture was not mentioned in the case report.
a The patient had alcoholic liver cirrhosis with normal baseline liver function.
b The blood culture results were not mentioned in the case report.
c The final outcome was not mentioned in the case report.
The tibia is the most common site of infective nonunion and chronic post-traumatic osteomyelitis. 17 A critical bone defect (>2 cm) can be managed with different bone reconstruction methods 18 ; for example, an autogenous bone graft, an allograft and bone graft substitutes, the IM technique, distraction osteogenesis, or a vascularized fibular graft transfer. Usually, the decision depends on the clinical scenario, surgeon preference, and facilities. Recently, the IM technique has garnered attention because of its effectiveness and low incidence of complications. 19 –21 The IM technique has a high success rate (85–92% in different series), 19,22,23 and led to the success in our case, in which the prolonged interval between stages did not negatively affect the outcome. 9,24 The second stage should be performed only after the infection and the soft tissue have healed. 9 If there is any suspicion of infection during the surgery, re-debridement and repetition of the first stage are suggested. 20 In our case, the paprika sign showed during the second stage without any sign of infection. It should be noted that the IM technique itself cannot cure infections.
In an otherwise healthy patient with a closed fracture, Aeromonas hydrophilia can cause acute osteomyelitis and necrotizing fasciitis by spreading from a nearby contaminated wound. Risk of cross contamination during a synchronous treatment of a contaminated open wound and a fracture cannot be eliminated although careful surgical techniques were employed. Exposure to water is a risk factor for Aeromonas hydrophilia infection.
Supplemental material
Supplemental Material, sj-tif-1-osj-10.1177_23094990211001587 - Aeromonas hydrophilia-infected nonunion of a closed tibial fracture in a healthy adolescent: A case report
Supplemental Material, sj-tif-1-osj-10.1177_23094990211001587 for Aeromonas hydrophilia-infected nonunion of a closed tibial fracture in a healthy adolescent: A case report by Wei-Kuo Hsu, Yi-Chuan Chou, Chang-Han Chuang, Chia-Lung Li and Po-Ting Wu in Journal of Orthopaedic Surgery
Footnotes
Acknowledgments
We are grateful to the Skeleton Materials and Bio-compatibility Core Lab, Research Center of Clinical Medicine, National Cheng Kung University Hospital, and Ms Yu-Ying Chen for the assistance in this study.
Author contributions
WKH, YCC, and PTW: study conception and design. WKH, YCC, CHC, and PTW: Data collection and literature review. WKH, PTW: wrote the manuscript. YCC, CHC, CLL, PTW: critical revision of the manuscript. All authors have read and approved the final submitted manuscript.
Availability of data and materials
All data concerning the case are presented in the manuscript.
Informed consent for publication
The case report was approved by the Institutional Review Board of National Cheng Kung University Hospital (NCKUH).
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by National Cheng Kung University Hospital (grants: NCKUH-10603023 and NCKUH-10702024). The funder had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.