
Abstract
Aim:
To report our experience with the Masquelet concept in a pediatric upper extremity following an open injury to the elbow.
Methods:
A case report and literature review.
Results:
An 11-year-old boy was transferred to our institution after a motor vehicle collision. There was a primary loss of the ulnohumeral articulation and the surrounding soft tissues as well as the ulnar nerve. Reconstruction used the Masquelet-induced membrane technique and a soft tissue flap. At the 30-month follow-up, the extremity was pain free and functional.
Conclusion:
This case highlights the value of the Masquelet technique in pediatric extremity injuries, where there is a loss of a major articular segment, as well as significant soft tissue compromise.
Introduction
After an extremity injury, the repair of missing and devitalized tissues can be problematic. The limb is considered mangled if more than three of four tissue components are affected (bone, soft tissue, nerves, and vessels). 1 Segmental bone loss has been traditionally managed with vascularized and non-vascularized autogenous bone grafts, 2 allografts, 3 Ilizarov bone transport, 4 acute shortening, and at least for the upper extremities, amputation as the last resort. In an evolution from open bone grafting with an external fixator of Papineau et al., 5 Masquelet et al. 6 proposed a two-stage reconstruction process, also known as the induced membrane technique. First, a polymethyl methacrylate (PMMA) spacer is placed for 1–2 months and combined with internal or external stabilization. Second, the PMMA is replaced with a bone graft with or without a bone graft expander. Histologic examination of the so-called pseudo synovial membrane that forms around the spacer has revealed a high concentration of osteoinductive factors. 7
Reports of the success of this technique are on the rise, but have predominantly described meta-diaphyseal bone loss in adults. Here, we present a pediatric case of a massive bone loss, which included articular cartilage that was reconstructed with the Masquelet technique.
Case report
An 11-year-old boy presented with an extensive comminuted open fracture of the left elbow associated with massive primary bone loss, measuring more than 10 cm in length. The patient lost the distal articular surface of the humerus, a 7 cm segment of the ulnar nerve, and ended up with a soft tissue defect over the medial elbow measuring about 7 by 10 cm. Other nerves and major vessels were intact. Limited internal fixation and an external fixator were used prior to his referral to our institution. The fixator pins were placed in the radius instead of the ulna, and the forearm was in neutral pronation. He arrived 3 weeks after the injury (Figure 1(a) and (b)). The radiographs showed subtotal articular cartilage loss, an injured distal humerus growth plate, and missing olecranon apophysis. Computerized tomography angiography revealed patent brachial, radial, and ulnar arteries. To ensure a sterile surgical bed, the child underwent several trips to the operating room for debridement and placement of antibiotic beads. Intraoperative tissue cultures were done because of late presentation and grew Enterobacter cloacae. Broad-spectrum antibiotics were initially started and then changed to culture-specific antibiotics that were administered for 40 days. Once the pouch was clean, PMMA block mixed with gentamicin was placed as the first stage of the induced membrane procedure and covered with a pedicled radial forearm flap and skin graft. The original fixator was left in place.
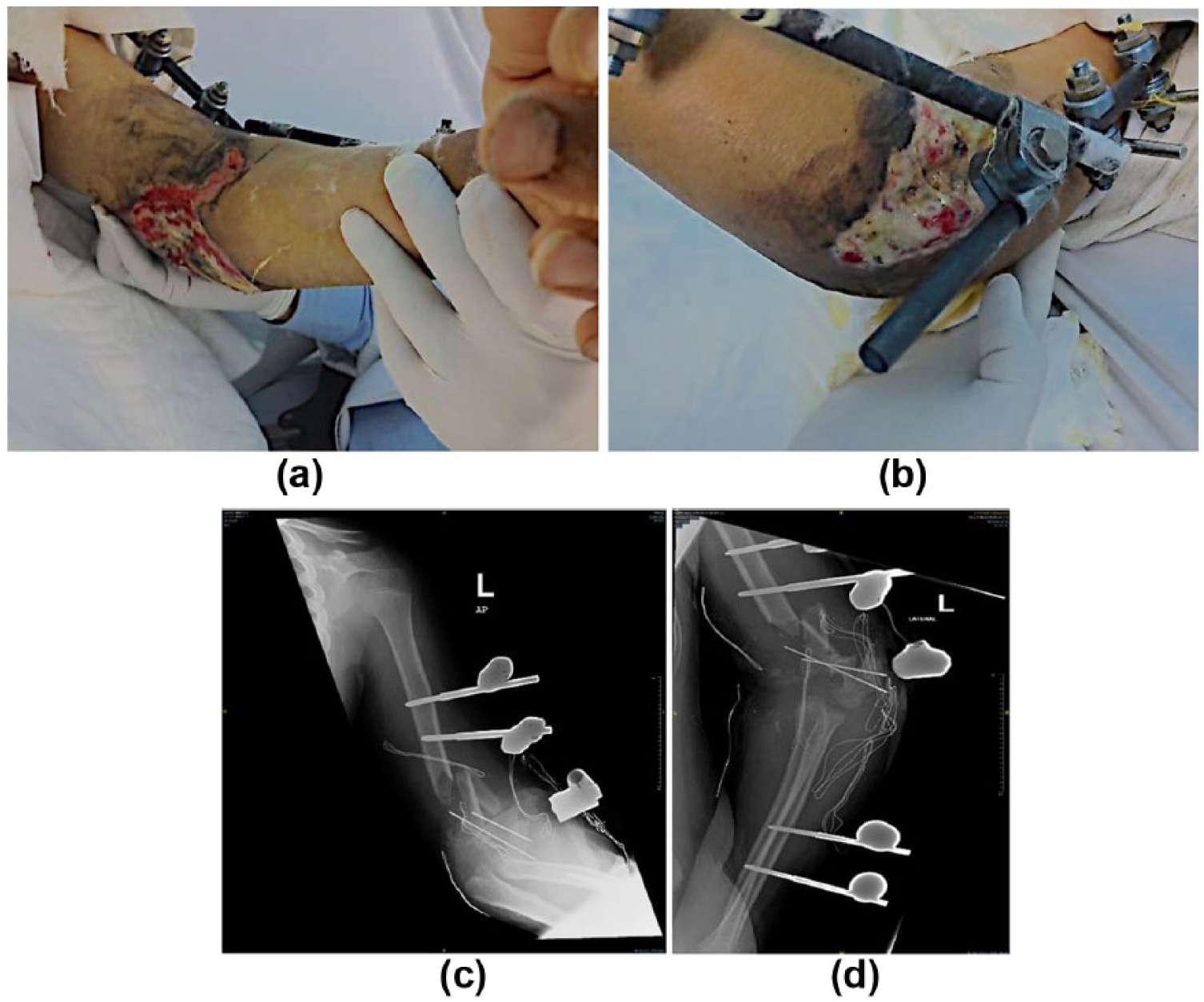
Clinical and radiographic pictures at presentation in our emergency department: (a,b) clinical photographs demonstrating the zone of injury, (c,d) plain radiographs in two planes; the pins and the external device were placed at the referring hospital.
Three months later, the soft tissue had healed, and serum inflammatory markers were normal. Therefore, treatment proceeded to the second stage. The flap was lifted followed by identification of the ulnar nerve stumps. The membrane was sharply opened, and the thick membrane was preserved. We then removed PMMA piecemeal. To fill the void, 50 cm 3 of ipsilateral iliac crest morselized cancellous autograft mixed with 45 cm 3 of allograft chips and 10 cm 3 of demineralized bone matrix was added. The cavity was closed watertight in a running fashion (Figure 2). For long-term stability after removal of the fixator, we placed a spanning locking reconstruction plate medially. Based on the child and his family preference, we kept the flexion at 65°. The ulnar nerve gap was reconstructed with sural nerve grafts. The patient was observed for another 11 months before we removed the fixator after consolidation of the transplanted bone. The patient’s wounds healed without surgical-site incidents.
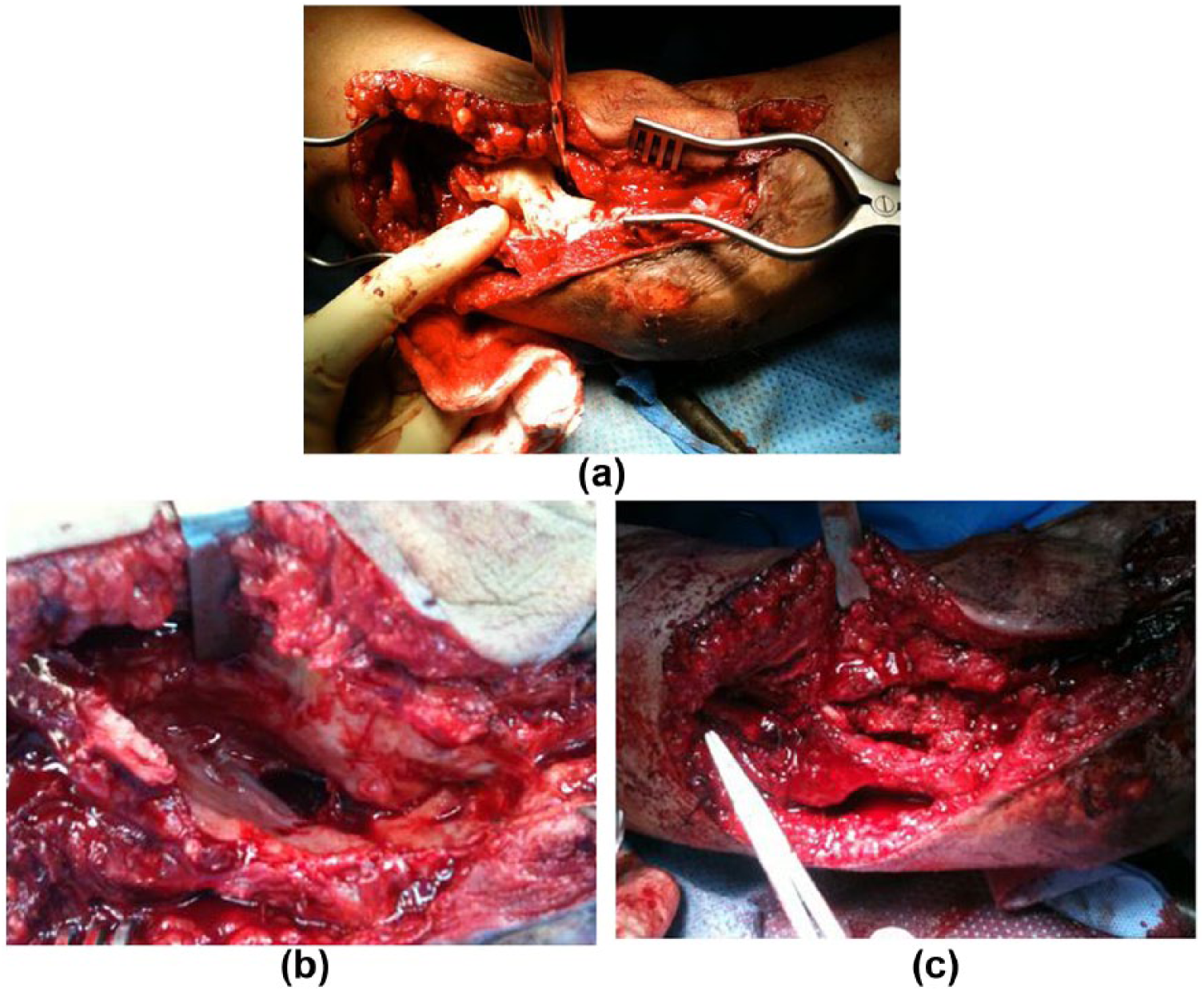
Intraoperative pictures during the second stage: (a) PMMA spacer, (b) showing the induced membrane, and (c) during closure after mixed bone graft placement.
During the follow-up assessment 30 months after the injury, the patient was satisfied with the appearance of the limb and had no pain or limitations when performing activities of daily living. There was mild residual clawing of the ring and little fingers, but near symmetric grip strength. He had partial recovery of the ulnar nerve. Radiographs confirmed healing (Figure 3).

Clinical pictures (a,b) and orthogonal radiographs (c,d) 3.5 years after the injury. Note corticalization and lack of bone resorption in (c).
Discussion
Segmental bone loss is typically the result of high-energy trauma. Elbow arthrodesis using an induced membrane technique in this patient did not affect growth as the physical plates were severely injured at presentation. This is expected to cause a growth discrepancy of less than 2.5 cm at skeletal maturity. 8 The long-term outcome of pediatric elbow arthrodesis is unknown.
In addition to the mechanical protection of the recipient cavity from collapse, the induced membrane strategy allows a clinician to ensure the readiness of the soft tissue for bone grafting. The surrounding inflammatory cells are believed to be from a foreign body reaction created by PMMA. 7 There are no known limits to the amount or structure of bone that can be reconstructed using this method; and defects up to 25 cm have been treated with this technique. 6
Because of the delayed presentation in this case and positive deep tissue cultures, we performed serial debridements along with a repeated application of antibiotics beads before initiation of the actual induced membrane technique. The bone graft expander in this case was at just over 50%, which is more than the 30%–50% mark empirically established by Masquelet. 9
Masquelet and Begue described an initial series of 35 patients who underwent reconstruction of segmental defects (5–24 cm long) between 1986 and 1999. Bone graft incorporation was successful in 31 patients (89%). Unprotected weight bearing began at 8.5 months (range, 6–17 months). Four patients who sustained late fractures were treated successfully with cast immobilization. 10 Karger et al. found a 90% union rate at a mean of 14.4 months after the first stage in 84 diaphyseal defects among various age groups. In one patient, the ankle was arthrodesed using the induced membrane method. 11 Gouron et al. 12 reported a 65% union rate using this technique in 14 pediatric patients with congenital and acquired pathologies. Additionally, Yi-Loong Woon et al. 13 and Ronga et al. 14 have used this method for open meta-epiphyseal fracture of the distal tibia to obtain a solid ankle fusion. Other authors have reproduced this technique and obtained similar results, with a union rate of between 85% and 92%.15,16
Microvascular tissue transfer of the fibula has notable donor site morbidity. A classic paper by Weiland et al. reported on 22 vascularized fibular grafts: for massive segmental bone losses following trauma, 8 were on the upper extremities, and the average length of the grafts was 16.2 cm. Weight bearing was allowed on average, 15 months after implantation. In addition to numerous complications, 12.5% of extremities ended up with amputation. 2 Cavadas et al. 17 reported on five skeletally mature patients who underwent vascularized bone transfer for massive bone loss in the elbow and all required second stage ligamentous reconstruction. Zafra et al. 18 reported on elbow reconstruction using a vascularized fibula flap after an open injury to the distal humerus and subsequent osteomyelitis requiring multiple debridements that mandated bone loss. Earlier, Hattori et al. 19 used a vascularized iliac crest and Nthumba et al. used a pedicled scapular flap for similar patients.
We were not in favor of vascularized bone transfer for this patient; largely because of the high functional demand and concerns about long-term stability since the trochlear notch was deficient. Total elbow arthroplasty was not a feasible option because of the patient’s age, massive bone loss, and the risk of infection.
Another reconstruction strategy would be Illizarove’s intercalary bone transport, which also entails a long course using the fixator and would require intense patient compliance. In one study of 17 patients, the average fixator time was 9.6 months, and the cohort did not have a regenerate length of more than 14.5 cm. The average number of operations per patient was 3.2. 4
Conclusion
In combination with microvascular tissue transfer, the Masquelet technique may be considered in mangled upper extremities in children with massive bone loss. Compared to alternatives, it is less technically demanding and provides predictable results. Additionally, it can be helpful in obtaining solid elbow fusion in salvage situations.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval to report this case was obtained from King Fahad Medical City, Institutional Review Board (log number 17-073).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from a legally authorized representative(s) for anonymized patient information to be published in this article.