
Abstract
Introduction:
Reconstruction of complex, open-grade distal femur fracture with bone defect presents an orthopaedic surgeon with a distinctive challenge as they are often associated with contaminated, compromised soft tissue and poor host condition. Conventional techniques like vascularized fibula transfer, autologous bone grafting or distraction osteogenesis focus mainly over bone union without taking infection control into consideration. The aim of this study is to evaluate the outcome of induced membrane technique in the reconstruction of open distal femur fracture with bone defect.
Methods:
10 such patients were retrospectively evaluated. Union was considered when a minimum of two cortices were seen on a radiograph. Knee Society Score was used to evaluate the functional outcome.
Results:
The average length of the defect was 5.7cm (3–10 cm) with mean interval period between the two stages being 42.7 days (34–51 days). Internal fixation was carried out in all cases. In 7 patients we used a mixture of cancellous autograft and cancellous allograft mixed in a ratio of 3:1. In the remaining 3 patients we used only cancellous autograft. Radiological union was achieved in all patients with mean union time of 8.5 months (7–11 months). Mean knee score was 79 (69–86) and mean function score was 71.5 (60–80).
Conclusion:
The induced membrane technique is an economical, technically less demanding technique for reconstruction of distal femur fracture with bone defects. The results are reproducible with a high success rate and without the need of any special instrumentation. It bestows infection control and prevents graft resorption. Long reconstructive period and donor site morbidity are matters of concern.
Introduction
Management of a high velocity, complex, open-grade distal femur fracture with bone defect presents a unique challenge for an orthopaedic surgeon. These fractures are often complicated due to compromised soft tissue, contamination and poor host condition. 1,2 Despite the recent advancements in technology and surgical techniques, infection and non-union are often encoutered. 1 The management principles for such fractures include fracture stabilization, adequate soft tissue coverage and infection control. Autologous bone grafting, vascularized bone grafts, distraction osteogenesis and induced membrane technique by Masquelet are the various contemporary techniques currently available for reconstruction of such defects. 3 Autologous bone grafts have been considered gold standard for such scenarios, but usually result in donor site morbidity and are insufficient in defects larger than 4 to 5 cm. Vascularized bone grafts are technically demanding 4,5 whereas distraction osteogenesis requires long reconstructive period with increased risk of infection. 6
Masquelet and Begue described a two-stage induced membrane technique for the reconstruction of larger defects (5–18 cm) with satisfactory results. 7 Stage one consists of radical debridement, cement spacer application, bone stabilization and soft tissue reconstruction; followed by sharp dissection of biomembrane, cement spacer removal and filling the biomembrane with autologous non-vascularized bone graft in the second stage. 3,7,8
We extensively searched the literature, but there is paucity of literature focusing solely on the efficacy of induced membrane technique in the reconstruction of distal femur fractures with bone defects.
The objective of this study is to evaluate the functional and clinical outcome of Masquelet’s induced membrane technique in reconstruction of complex, post-traumatic, open-grade distal femur fractures with bone defects.
Material and methods
All adult patients admitted in our level 1 tertiary trauma care centre between June 2015 to June 2017 with post traumatic, complex, open-grade distal femur fractures with bone defects and reconstructed with two-staged induced membrane technique were included in this study. Patients having distal neuro-vascular deficit (DNVD) were excluded from this study. Details such as demographic data, mechanism of injury, injury type, defect type, defect length, antibiotics used in the cement and the mode of fixation were documented (Table 1). Defect length was calculated as the vertical distance between the viable bone ends following debridement (Figure 1). All patients were treated by the lead author. They were taken for the 1st stage surgery within 3 days of injury.
Case details.
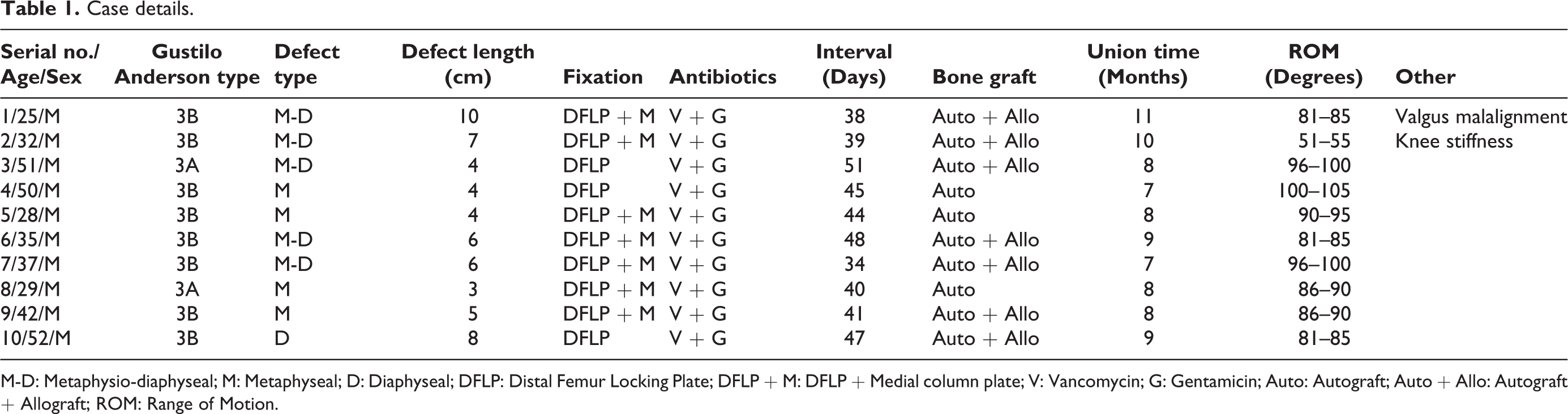
M-D: Metaphysio-diaphyseal; M: Metaphyseal; D: Diaphyseal; DFLP: Distal Femur Locking Plate; DFLP + M: DFLP + Medial column plate; V: Vancomycin; G: Gentamicin; Auto: Autograft; Auto + Allo: Autograft + Allograft; ROM: Range of Motion.
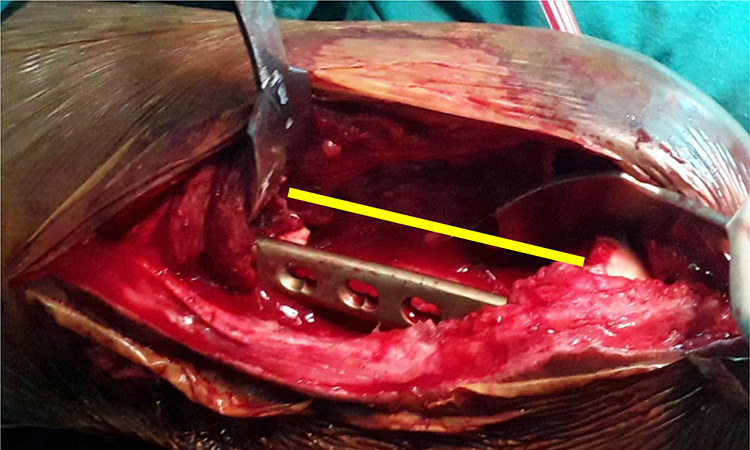
Measurement of the defect length following debridement.
Stage-1: The affected limb was prepared in a routine manner. Thorough soft tissue debridement was carried out. Loose and devitalized bone fragments were removed. The bone margins were freshened till bleeding bone was visualized. The defect length was then calculated and documented. Internal fixation was carried out with an anatomic locking plate after achieving acceptable reduction, alignment and length. The bed of the defect was then packed with absorbable gelatin sponge (Figure 2). This created a partition between the soft tissue and the cement spacer; providing protection to the underlying soft tissue from exothermic heat generated by the cement spacer. The defect was then filled with an antibiotic impregnated cement spacer made by mixing 4 g of Vancomycin and 6 ml Gentamicin to 40 g polymethylmethacrylate cement (Surgical Simplex P, Stryker, Michigan, USA). The antibiotic cement spacer was placed in the defect in it’s working phase. Care was taken to prevent overstuffing of the defect. Once the defect was filled; constant saline irrigation was carried out to prevent soft tissue thermal necrosis. Hemostasis was achieved and wound closure was done. Soft tissue coverage procedures were carried out if required.
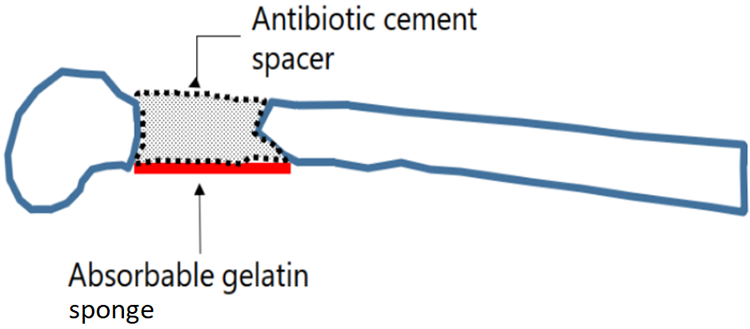
Diagramatic representation showing creation of an absorbable gelatin sponge bed at the base of the defect to protect the underlying neurovascular structures from the exothermic heat generated by the cement spacer.
Post-operative intra-venous (I.V) antibiotics prophylaxis of 1gm Cefixime and 0.5gm Amikacin till the 2nd post operative day. From the 3rd day, oral Cefixime 200 mg tablet twice a day was prescribed till suture removal. Patients were encouraged to perform active and passive knee mobilization as and when tolerated. Regular assessment of the local area for any signs of infection or inflammation was carried out. Weekly Total Count (TC), Erythrocyte Sedimentation Rate (ESR) and C-Reactive Protein (CRP) estimation was done. Once the incision site healed and ESR, CRP levels dropped within normal limits; stage-2 was planned. If ESR, CRP levels did not decrease or if there were clinical signs of infection; debridement and exchange of the antibiotic cement spacer was carried out.
Stage-2: The cement spacer was removed in a piece-meal fashion following sharp dissection of the biomembrane encapsulating it. Once the cement spacer was removed, thorough irrigation of the biomembrane was carried out to remove any debris. The medial column was fixed when required. Autograft harvested from the ipsilateral and/or contralateral iliac crest was then used to fill the defect. As all the patients in this case series were operated in supine position, the use of posterior iliac crests for autologous bone graft harvest was avoided. In cases with large defects (>4 cm); we used a mixture of fresh cancellous autograft and freeze-dried cancellous allograft mixed in a ratio of 3:1. The allograft was freeze dried, cancellous bone graft procured from a bone bank. It was allowed to thaw in a warm saline solution. It was then immersed in 0.2 mL of 2% (20 mg/mL) antibiotic solution containing gentamicin and vancomycin for 30 minutes as described by Shah et al. 9 The entire defect was then filled with this mixture. The biomembrane was then closed with absorbable 2–0 vicryl sutures. Tight closure of the remaining layers was done in a routine manner.
Post-operative rehabilitation: All the patients were given a knee brace. Active and passive mobilization of the knee was encouraged as soon as possible. Partial assisted weight bearing in the form of toe-touch walking with a walker was allowed after 8–10 weeks following second stage. Full weight bearing was allowed only after radiological union.
Regular clinical and radiological evaluation of the patients was carried out. They were assessed for union, range of motion or any complications that may arise. Radiological union was considered when a minimum of two cortices demonstrated union (Figures 3 and 4). All patients were followed up for a minimum of 3 years. The Knee Society score 10,11 was used to evaluate the final outcome. Owing to the small sample size statistical analysis was not carried out.
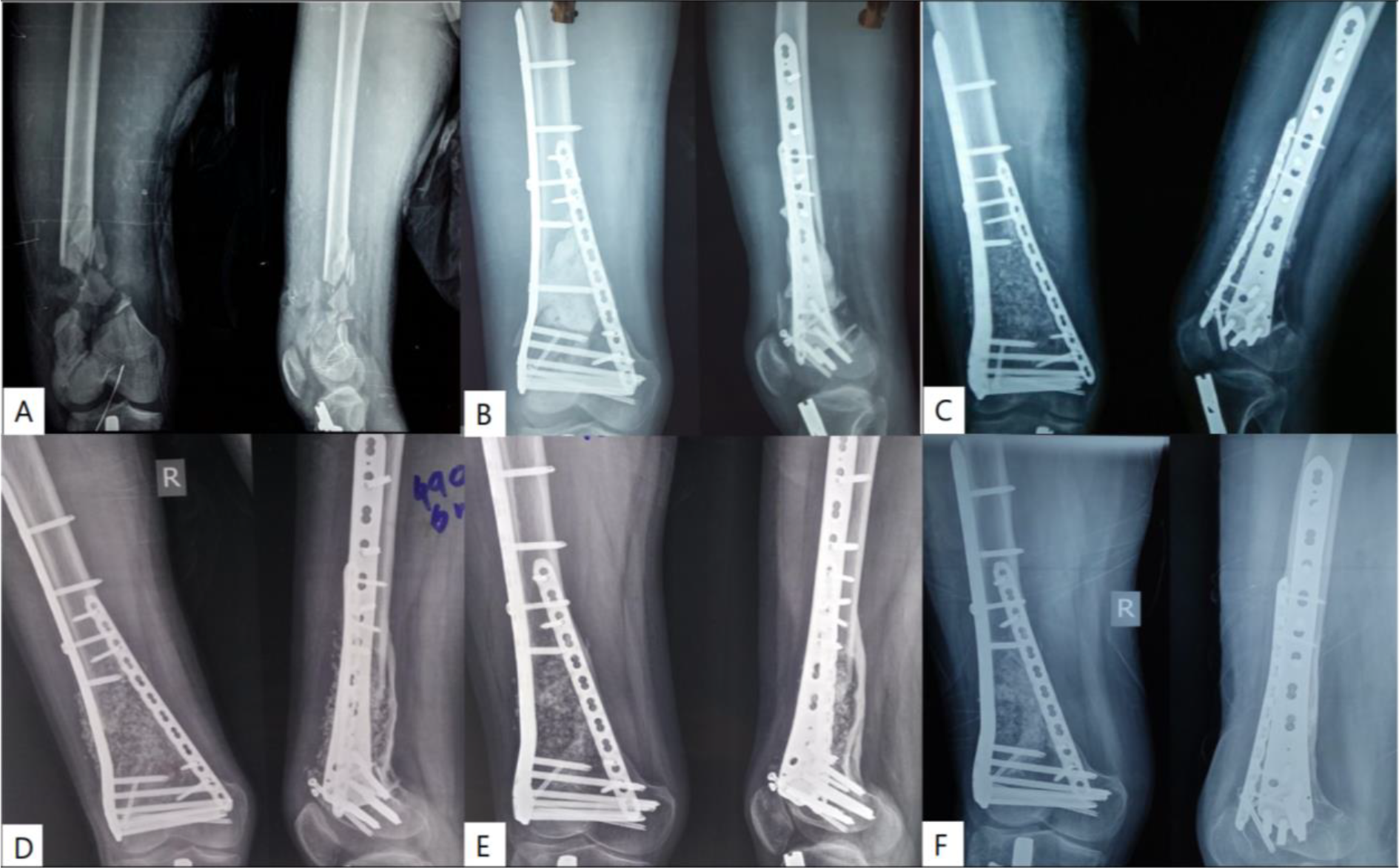
Case-1 A) Pre-op radiograph B) Radiograph following debridement, antibiotic spacer placement and internal fixation. C) Radiograph following antibiotic cement spacer removal and bone grafting. D, E, F) 6, 9 and 24 month follow-up radiograph.
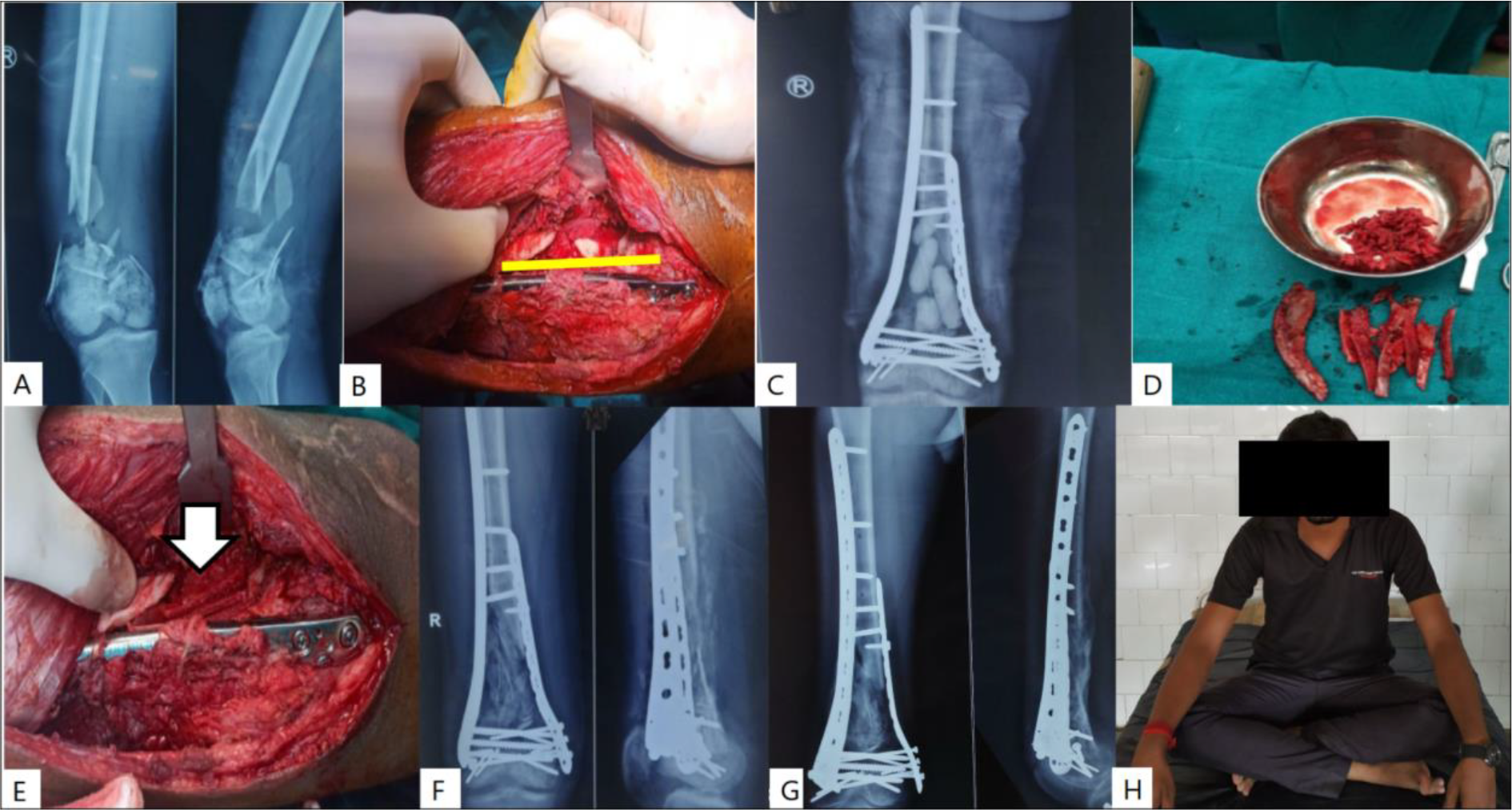
Case-6 A) Pre-op radiograph B) Defect following debridement C) Radiograph following stage-1 D) Cancellous bonegraft harvested from the iliac crest E) Bone grafting of the defect within the biomembrane (arrow) F) Radiograph following Stage-2 G, H) Radiological and clinical follow-up at 18 months post injury.
Results
10 patients who were admitted to our level 1 tertiary trauma care centre with complex, open grade, distal femur fracture with bone defect and treated with induced membrane technique were retrospectively analysed for this study. All patients were males; with mean age of 38.1 years (range 25–52 years). Road traffic accidents (RTA) was the cause of injury in 9 patients, whereas 1 patient suffered from farm machine injury. 8 (80%) patients suffered from Gustillo-Anderson (GA) type IIIB fractures; whereas 2 (20%) patients suffered from GA type IIIA fractures. 4 (40%) had associated fractures of ipsilateral tibia. Following debridement, the mean defect length was 5.7 cm (range 3–10 cm). 4 (40%) patients suffered from metaphyseal defects; whereas the meta-diaphyseal and diaphyseal defects were found in 5 (50%) and 1 (10%) patient respectively. Internal fixation with Distal Femur Locking Plate (DFLP) was the preferred method of fixation in all the cases. None of the patients required revision of stage-1. The mean interval between the two stages was 42.7 days (range 34–51 days). A mixture of cancellous autograft and freeze-dried, cancellous allograft mixed in a ratio of 3:1 was used in 7 (70%) patients. In the remaining 3 (30%) patients cancellous autograft harvested from the anterior iliac crests was enough to fill the defect. Medial column fixation was carried out in 7 (70%) patients. Average time for radiological union was 8.5 months (range 7–11 months). 2 (20%) patients suffered from delayed union (union time > 9 months). Both these patients had defect length greater than 9 cm. No surgical intervention was required for these patients. No cases of non-union and donor site morbidity were reported.
Mean knee flexion following the second stage surgery as measured at the final follow-up was 86.6 degrees (range 53–103 degrees) with a mean 5 degree (range 0–10 degree) extension lag. 1 (10%) patient suffered from valgus mal-alignment. He had a metaphysio-diaphyseal defect of 10 cm. The patient refused any surgical intervention. 1 (10%) patient was unable to flex knee beyond 10 degree. 10 months following the second stage, open knee joint adhesiolysis and quadriceps release was performed. His final knee R.O.M was 51–55 degrees. Knee Society Score was used to evaluate the final outcome. The mean knee score was 79 (range 69–86) whereas; the mean patient function score was 71.5 (range 60–80).
Discussion
We reconstructed 10 patients with complex, open-grade distal femur fractures with bone defects using the induced membrane technique. The two-stage induced membrane technique by Masquelet and Begue is a well established method for the reconstruction of long bone defects of any etiology. 12,13 The first stage comprises of radical debridement, skeletal fixation, insertion of cement spacer and soft tissue reconstruction. The second stage involves removal of the cement spacer keeping the biomembrane encapsulating it intact. The defect is then filled with morsellised, cancellous autograft. 7
The use of induced membrane technique for the reconstruction of complex, open grade distal femur fractures with bone defects offers several advantages. The antibiotic impregnated cement spacer elutes high doses of antibiotics locally. This prevents any chances of infection, which has been reported to occur in 10–50% cases of open fractures. 14 –16 None of the 10 cases in this study suffered from infection. In addition; it maintains a well-defined void which allows for placement of bone graft at a later stage along with providing structural support and thereby offloading the implant. 17 Further, the cement spacer induces a foreign body reaction resulting in the formation of a highly vascularized biomembrane encapsulating it, which secretes high concentrations of growth factors like Vascular Endothelial Growth Factor (VEGF), Transforming Growth Factor (TGF) Beta-1 and Bone Morphogenic Protein (BMP)-2. These improve the chances of graft consolidation and prevent graft resorption. 7,8 Masquelet and Begue reported a prospective study of 35 patients with bone defects who underwent reconstruction using the induced membrane technique. They reported union in 89% of the patients. Other studies in this direction have also reported a success rate ranging from 85% to 92%. 18,19
Masquelet et al. in their study; used external fixators for providing stability, but various other authors have utilized several variations of internal fixation methods with satisfactory results. 1,17,18 Stafford et al. described a series of 25 patients having lower extremity non-unions with bone defects treated with Reamer-Irrigator-Aspirator (RIA) bone graft. They used either a plate-screw construct or an intramedullary nail in all their cases and reported a union rate of 90% at 1 year follow-up. 20 In our study; all the 10 cases had intra-articular extension of the fractures and all cases were primarily fixed with anatomic locking plates. Radiological union was achieved in all the cases. No cases of infection were reported.
The optimal time for second stage surgery according to Masquelet et al. is 1 month after the insertion of the cement spacer. 7 Other studies have reported that the optimal timing for the second stage is 4 to 6 weeks after placement of the antibiotic cement spacer, with 1 month-old membrane showing the highest expression of VEGF and 2 month-old membranes expressed less than 40% of the VEGF levels. 21 –23 The mean interval period between the two stages in our study was 42.7 days (range 34–51 days).
We used morselized cancellous autograft harvested from iliac crest in 3 (30%) patients to fill the defect, while in remaining 7 (70%) patients, we used the mixture of freeze dried, cancellous allograft and morcelized cancellous autograft mixed in a ratio of 1:3. All 10 (100%) patients showed radiological union in our study. The original technique suggests that the allograft and autograft should be mixed in a ratio of 1:3. They reported an average union time of 4 months. In our study; the average union time was 8.5 months. This stark difference of average union time between the study by Masquelet et al. and this study can be pinned down to the fact that Masquelet et al. evaluated the time for union from the moment of second stage surgery and not from the completion of stage 1 surgery; as in our study. 7,13,24 One recent study by Kasha et al. has reported an average union time of 280 days in their series of 27 patients with post-traumatic bone. They mixed the allograft and autograft in a ratio of 1:2. 1
In this study the freeze dried, cancellous allograft was allowed to thaw in a warm saline solution. It was then immersed in 0.2 mL of 2% (20mg/mL) antibiotic solution containing gentamicin and vancomycin for 30 minutes as decribed by Shah et al. 9 This allowed us to achieve antibiotic concentration of 5 times higher the minimal inhibitory concentration (MIC) values in the cancellous allograft. This modification provides prophylaxis against any resurgence of infection following the second stage.
There was no use of additional growth factors like Bone Marrow Concentrated Aspirate (BMCA), Platelet Rich Plasma (PRP) and Bone Morphogenic Protein-7 (BMP-7) in this study. Studies carried out by Piacentini et al., 3 Friedlaender et al., 25 Hakimi et al. 26 and Takemoto et al. 27 have not been able to establish their synergistic effect when used together with autogenous bone graft.
Despite the reported success of induced membrane technique, some concerns have been raised pertaining to the infection, donor site morbidity and prolonged reconstruction period. 3,8,12 The original study by Masquelet et al. described the use of PMMA spacer without antibiotics in the stage-1 surgery. 7 The efficacy of antibiotics impregnated cement spacer in prophylaxis and treatment of infection is well documented; therefore its use in stage-1 surgery along with radical debridement can help ward off this complication. 28 In our study, we used anitibiotic impregnated cement spacers in stage-1 and bone allograft soaked in warm antibiotic saline solution in stage-2 to act as a local antibiotic depot and thereby elute high concentrations of local antibiotics to prevent infection. Regarding the prolonged reonstruction period required; it should be considered that for the extensive reconstruction of large defects with a possibility of infection, two surgical steps are inexorable in order to remove infection and necrotic tissues and prevent its resurgence.
This study demonstrates successful reconstruction of complex, open-grade distal femur fractures with bone defects using Masquelet’s induced membrane technique. But there are some limitations to this study. It is a non comparative study with small sample group. Statistical analysis was not performed owing to the small sample size.
Conclusion
Masquelet’s induced membrane technique has been used successfully for over two decades for the reconstruction of bone defects of any etiology. This technique of delayed bone grafting in a biological membrane induced by the placement of an antibiotic impregnated cement spacer provides a rational alternative for the reconstruction of complex, open grade distal femur fractures with bone defect. It is an economically viable, safe and reliable method which does not require any special instrumentation.
Footnotes
Patient declaration statement
The authors declare that written consent of all the patients were taken for the above mentioned procedure. Also they were informed that clinical images and images of their radiographs will be taken for educational purposes. They were also assured that at no stage and under no circumstances will their identity be revealed.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.