
Abstract
Purpose:
To perform retrospective analysis of 75 post-operative disc space infections after open lumbar discectomy (OLD) and to assess the outcome of their medical and surgical management in a tertiary-level hospital.
Methods:
Records of 50 men and 25 women aged 26–65 (mean, 42.53) years who underwent treatment for post-operative discitis (POD) after single level OLD at L3–4 (n = 8), L4–5 (n = 42), L5–S1 (n = 25) level. The POD was diagnosed according to specific clinical signs, laboratory and radiographic investigations and all of them received initial intravenous antibiotics (IVA) for at least 4–6 weeks followed by oral ones. Successful responders (n = 55) were considered in Group-C and remainder [Group-S (n = 20)] were operated at least after 4 weeks of failure. Demographic data, clinical variables, hospital stay, duration of antibiotic treatment and post-treatment complications were collected from the hospital record and assessment before and after treatment were done by using visual analogue scale (VAS) and Japanese Orthopaedic Association (JOA) score. Comprehensive outcome was evaluated by modified criteria of Kirkaldy-Willis.
Results:
The mean follows up was 36.38 months. Significant improvement of mean VAS and JOA score was achieved in both conservative (76.36% satisfactory) and operative (90% satisfactory) groups although the difference was statistically insignificant.
Conclusion:
Although insignificant, early surgical intervention provided better results (e.g. functional outcomes, length of hospital stay and duration of antibiotic treatment therapy) than conventional conservative treatment in post-operative discitis.
Introduction
Discitis is an infection or inflammation of the intervertebral disc (IVD) space or vertebral end plate (VEP), first described by Frank Turnbull in 1953 as a clinical entity. 1,2 Nucleus pulposus is primarily affected along with secondary involvement of cartilaginous end plate and vertebral body following discectomies. 3,4 The incidence of post-operative discitis (POD) varies from 0.2% to 4%, 5 –7 and the cause is mainly iatrogenic and bacterial, with some descriptions of spontaneous discitis. 4,8,9 Whatever the source; either aseptic or infective, only 42–73% of organism could be isolated. 5,10 Early diagnosis is crucial, usually done by high index of suspicion. Persisted back pain after 1–8 weeks of surgery (ranging 2 days to 10 weeks), persistently raised C-reactive protein (CRP), raised ESR, corroborative X-ray/CT features and signal changes in disc spaces on MRI are pathognomic (Figures 1 and 2). 4,11,12

Discitis at L4–L5 level following fenestration and discectomy of 33 year old man. (a and b) T1 and T2 sagittal and (c) axial images of post-operative discitis with altered vertebral marrow signal intensity and associated end plate erosion. (d and e) T1 and T2 sagittal MRI after 3 months of conservative treatment, (f, g and h) follow-up plain X-ray at 3, 6, and 18 moths gradual narrowing of disc space and union occur.

(a and b) T1 and T2 sagittal and (c) axial images of post-operative spondylodiscitis. (a) and (b) showing acute stage with altered vertebral marrow signal intensity and associated end plate erosion. (d and e) Sagittal image with contrast (e) and (f and g) plain X-ray A-P, lateral view before operation showing reduced L5–S1 space with end plate irregularity, (h) shows narrowing of disc space with healing after 14 months of PLF with posterior instrumentation following transforaminal debridement.
Treatment option for POD is either conservative or operative. In cases of open lumbar discectomy (OLD), some author recommended 6–8 weeks of intravenous therapy alone, whereas others proposed 6–8 weeks of intravenous antibiotics (IVA) followed by 2 months or more of oral therapy, depending on clinical and laboratory parameters. 4,11,13,14 Some author advocates surgical intervention in the form of early debridement along with IVA instead of providing IVA alone. 15 Based on the differences in the available literatures, we retrospectively assessed the treatment outcome of POD after OLDs in our tertiary-level hospital to assess, when conservative treatment failed and what type of surgery was required and also to provide an outline about the appropriate treatment option for POD.
Materials and methods
We retrospectively evaluated the hospital records of 2680 patients from October 2003 to September 2018, 1000 patients were treated primarily by Limited Discectomy (LD) [e.g. removal of the offending disc fragment alone without or with little invasion of the disc space] 16,17 and 1680 patients underwent Aggressive Discectomy (AD) [e.g. removal of the offending herniated disc fragment as well as repeated invasion of disc space (curettage) to remove the loose or fragmented disc from normal disc]. 17,18 Out of these, POD patients were 69 (2.57%) [LD, n = 19 (1.9%) and AD, n = 50 (2.98%)]. Additional other institutional referral was 11 patients [AD, (n = 11)]. Finally, 75 out of 80 patients, were enrolled in our study. Among them 50 men and 25 women within the age range of 26–65 years (mean, 42.53) underwent treatment for POD after single level open discectomy [e.g. Level L3–4 (n = 8), L4–5 (n = 42), and L5–S1 (n = 25)]. Factors associated with discitis were chronic smoker (n = 32), obesity (n = 23), diabetes mellitus (n = 18) and malnourished (n = 2). Inclusion criteria were: (1) POD following single level OLD; and (2) POD with radiculopathy. Excluded were: (1) spontaneous discitis, (2) multiple-level OLD, (2) patients lost during follow-up after discharge. We eliminated (a) three patients from the study who were lost during follow-up; (b) two patients who died due to unrelated medical illness.
All POD patients were treated under the care of the same surgeon. The patients were diagnosed clinically, supported by appropriate radiological and laboratory investigations. All primary OLD patients underwent same IVA protocol from induction to discharge. All suspected patients had constant back pain that became worse at night. Typically, it was easily exacerbated by any motion, positive pseudo Gower sign and straight leg raising test (SLRT). The Blood parameters [i.e. complete blood count (CBC), erythrocyte sedimentation rate (ESR). C-reactive protein (CRP)] and other parameters i.e. blood culture, urine culture, blood sugar, seum albumin, liver and renal function test; were done routinely, and radiological assessment included plain X-rays of lumbosacral (LS) spine antero-posterior and lateral views, dynamic X-ray and gadolinium enhanced magnetic resonance imaging (MRI) were done for diagnosis as well as evaluation of treatment response. CT-guided aspiration of the disc space (using a needle or trocar) for microscopy and culture and biopsy were also performed to identify the bacterial pathogen. All patients received conservative treatment in the form of 4–6 weeks of IVA followed by an additional 4–6 weeks of oral forms or until symptomatic improvement of back pain or ESR and CRP values significantly improved.
The IVA was withdrawn on the basis of clinical improvement and normalization of CRP and ESR. If pain and the inflammatory markers (e.g., ESR and CRP) failed to reduce or CRP kept persistently raised above 30 mg/l, 19 even after 4–6 weeks of conservative treatment, operative treatment was advised. There were found 20 (26.67%) cases who remined symptomatic along with raised ESR and CRP or developed nerve roots impingement (n = 15), vertebral body destruction and progressive kyphotic deformity (n = 8), were treated surgically. The patients responded solely to conservative means were designated in Group-C (n = 55), and the operative cases were ensued in Group-S (n = 20). Interventions encompassed from the range of sole debridement [n = 9 (45%)], posterolateral fusion (PLF) and posterior instrumentation (PI) [n = 5 (25%)] (Figure 2(h)) to interbody fusion (IBF) with titanium banana cage and autogenous cancellous bone grafts (ACBG) and PI [n = 6 (30%)], depending on the duration of onset of symptoms, severity of pain, disc space reduction, degree of stenosis and kyphotic deformity. Notably discitis with posterior epidural abscess and without end plate erosion, were treated with simple debridement, intractable back pain, end plate erosion, neurologic compromise, disc space reduction and epidural abscess were treated with debridement along with PLF + PI and when associated with an unstable mechanical kyphotic deformity, were treated with IBF with banana cage + PI. Moreover, we considering the criteria for discontinuation of antimicrobial therapy when resolution of clinical symptoms as well as normalization of ESR (<20 mm/h) and CRP (<10 mg/L) occurs.
Results of surgical treatment were observed on the basis of symptomatic improvement with laboratory and imaging findings after 1, 3, 6, 12 months consequently and yearly thereafter. IBF status was evaluated at 6 and 12 months by radiography and or CT scan post-operatively. Demographic data, clinical variables, length of hospitalization, duration of IVA, Culture and Sensitivity report (CSR) and post-treatment complications were recorded and pre- and post-operative assessment were done by using VAS scale and JOA score. Comprehensive outcome of each patent was graded by modified criteria of Kirkaldy-Willis 20 as excellent, good, fair or poor. All the data were analysed statistically by using SPSS (version 25, Armonk, NY, IBM Corp.). The results were expressed as frequency, percentage and mean ± SD. Paired Student’s t-test and Z proportion test were performed as applicable. Level of significance was calculated at confidence interval of 95% and p < 0.05.
Results
The mean pain-free interval before development of symptoms of POD after primary OLD was 3.2 weeks (range, 1–8 weeks). Mean duration of symptoms prior to admission was 8.8 days (range, 5–21 days). All patients had moderate (n = 23) to severe back pain (n = 52), radiculopathy (n = 38), mild fever (n = 26), paravertebral muscle spasm (n = 65), positive SLRT (n = 64), pseudo Gower sign (n = 55) and the surgical site skin incision appeared to be normal in all patients, except local erythema, swelling, or a draining sinus were seen in three patients. Two of them resolved within 10 days after local debridement but last one required secondary closure on 14th post-operative day and had Pseudomonas aeruginosa (PA) resistant to Ceftriaxone. It was then treated by IVA regimen according to culture sensitivity.
Inflammatory markers (e.g. ESR and CRP) were increased in all patients and had significant improvement in both Group-C and Group-S. The values started to decrease in week 3 except in Group-S and majority of the patients returned to normal within 2–3 months, whereas within 6 months post-treatment it was nearly normal in all patients. In blood culture and CT-guided aspiration, 64% cases revealed the causative organism where Staphylococcus aureus (SA) was significant. Biopsy report did not reveal any granulomatous lesion.
Among Group-C most patients [n = 52 (69.34%)] required 28–42 days (4–6 weeks) IVA followed by 35 days (5 weeks) in oral forms. Mean duration of administration of both IVA and oral was 78.00 ± 5.35 (range, 69–92) days [Table 1]. The mean hospitalization time was 5.2 weeks (range 28–45 days). The mean improvement of VAS [from 7.16 (±1.98) to 2.47 (±1.93)] and JOA [from 8.82 ± (3.03) to 23.04 ± (2.87)] was significant with an estimated mean difference of −14.22 (95% CI −16.57 to −12.78, P < 0.001) [Table 2].
Inflammatory markers, blood culture, aspiration and tissue biopsy results.
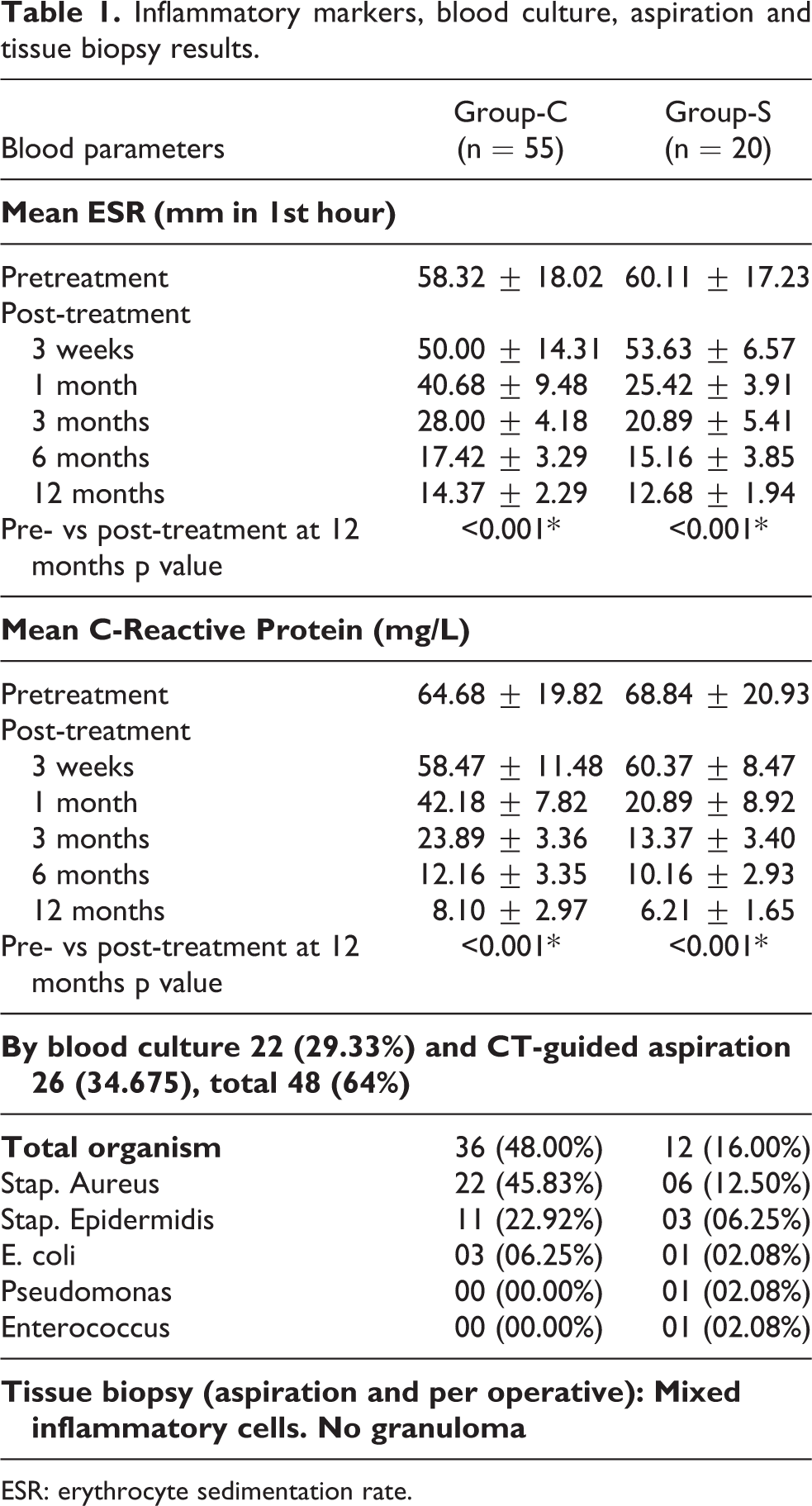
ESR: erythrocyte sedimentation rate.
Clinical and functional outcome assessment by VAS, JOA score and modified criteria of Kirkaldy-Willis. 20
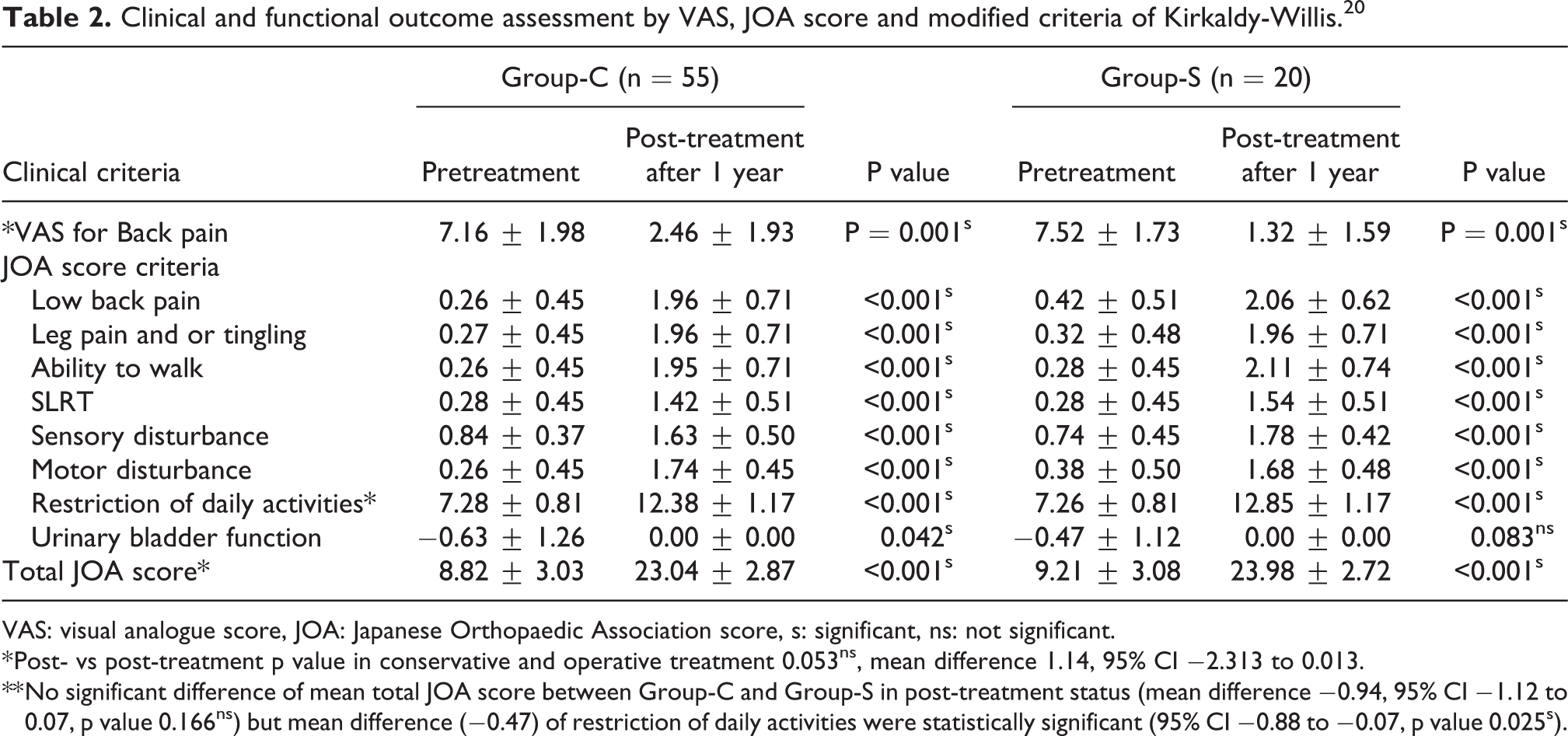
VAS: visual analogue score, JOA: Japanese Orthopaedic Association score, s: significant, ns: not significant.
* Post- vs post-treatment p value in conservative and operative treatment 0.053ns, mean difference 1.14, 95% CI −2.313 to 0.013.
** No significant difference of mean total JOA score between Group-C and Group-S in post-treatment status (mean difference −0.94, 95% CI −1.12 to 0.07, p value 0.166ns) but mean difference (−0.47) of restriction of daily activities were statistically significant (95% CI −0.88 to −0.07, p value 0.025s).
In Group-S, 14–21 days IVA was administered post-operatively followed by oral forms usually for 21–28 days. Mean duration of administration of both IVA and oral forms was 40.15 ± 3.48 (range, 34–50) days and the mean immobilization time was 4.4 weeks (range 28–45 days). Both VAS [from 7.52 ± 1.73) to 1.32 ± 1.59] and JOA [from 9.21 ± 3.08 to 23.98 ± 2.72] had significant improvement with an estimated mean difference of −14.77 (95% CI −16.58 to −13.00, P < 0.001) [Table 2]. Almost all the patients were mobilized within 48–72 hours after surgery. No reported post-operative adverse events leading to their normal daily activities within 6 months.
Based on CSR, Meropenem, Flucloxacillin, Linezolid and Fusidic Acid were sensitive for Staphylococcus aureus and Staphylococcus epidermidis. Additionally, Escherichia coli, Enterobacter species and Pseudomonas aeruginosa were sensitive to Ciprofloxacin and Tobramycin. Third-generation Cephalosporins (Ceftriaxone) was used empirically and during primary surgery but was resistant to Staphylococcus aureus, Staphylococcus epidermidis, Escherichia coli in 40% cases.
Although the wound infections 4 (5.33%), [Group-C, (n = 3); Group-S, (n = 1)] could be managed conservatively, neurological deterioration, kyphotic deformity and instability was reported with conservative treatment [n = 8 (14.54%)] and required surgical intervention. Prolonged IVA culminated in drug induced hepatitis [n = 3 (4%)], renal impairment (increased serum urea and creatinine) [n = 3 (4%)], hypersensitivity reaction [n = 1 (1.33%)], phlebitis (I/V canula site) [n = 3 (4%)] and consequently all IVA related complications gradually improved after either adjustment or changing of drug regimen over a period of 6 weeks. According to modified criteria of Kirkaldy-Willis, excellent result was significant with Group-S [n = 10 (50%)] whereas overall satisfactory rate (Group-C, 76.36%; Group-S, 90%) was also significant [Table 3].
Functional outcome according to modified criteria of Kirkaldy-Willis. 20

Discussion
Despite taking all the measures to reduce the incidence of POD following OLD, these remain a dangerous complication which increases the morbidity of the patient and the cost of healthcare. IVD are largely avascular structure with the outer layers receiving nutrients from the end arterioles and the central portion receiving nutrients by diffusion from the vertebral end plates. The majority of surgeons opined that direct inoculation is the most likely mode of pathogen seeding during interventional disc procedures. 4,10,21 Wide ranges of organism are responsible for postsurgical discitis, among them most common aetiological agent are Staphylococcus Aureus (60%) followed by Staphylococcus epidemidis and anaerobic organisms. Other less common organisms include Streptococcus viridians (SV), Escherichia Coli (EC), Pseudomonas Aeruginosa (PA), Mycobacterium tuberculosis (MT), fungus (candida, aspergillus) and others. 4,6,9,22 Although only 42–73% causative organism can be isolated by culture as mention in several studies. 4,5,10 In our study by blood culture and CT-guided aspiration from the disc space total 64% organism (29.33% by culture, 34.67% from CT-guided aspiration) were isolated, among them mostly (58.33%) were Staphylococcus Aureus [Table 1]. Fungal infections following discectomy is very rare and MRI finding of fungal infections showed multilevel bone destruction without any abscess formation. 23 and whenever there was no satisfactory response it was evaluated for atypical infections. Infection rate varies with the type of surgery, with or without internal fixation or instrumented fusion and site of surgery. 5 –7,24,25 But in this study following OLD the infection rate was 2.57% which were similar to other studies 5 –7
Most of the patients of POD could be managed conservatively with immobilization (bed rest, orthosis), analgesic along with intravenous antibiotic therapy. 26 –28 In our study 69.34% patients treated conservatively and 26.67% treated surgically. Despite the traditional conservative treatment ends with good outcome, the prolonged period of immobilization and long duration of antibiotic regimens sometimes lead to undesired medical and psychosocial consequences 14,29,30 and also antibiotic related major complications (e.g. colitis, renal failure, allergic reactions and phlebitis). 31 Even after successful control of infection by prolong antibiotic therapy, some patients may developed some degree of vertebral body destruction which may lead to instability and progressive kyphosis, nerve roots impingement, and persistent back pain. On the other hand, by doing early surgery, pain relief as well as infection control could be achieved early but patient may develop some operative procedure related complications. Following conservative treatment, the overall long-term prognosis is good, having reported success rates of 70–83%. 4,5,9 which is comparable to our study (76.36%). Study by Rawlings et al. 11 reported that following conservative treatment, 75% cases undergo either a bony ankylosis or stable fibrous union within 2 years period and 90% patients become pain free but in contrast there are also reports that only 35% cases end up with bony ankylosis by 2 years and most of them frequently complaint of residual mechanical back pain. 32,33 Study by Hadjipavlou et al. also showed medical means resulted mechanical back pain in 64% cases as opposed to 26% of patients treated surgically. 34 Furthermore, patient who did not respond to medical management, their infection usually progress with worsening of sign and symptoms and elevation of inflammatory markers or the progression of kyphotic deformity. These two clinical scenarios often go in favour of surgical treatment. Another recent study showed satisfactory results following operative treatment e.g. debridement, ACBG and IF in 17 consecutive patients at their mean follow-up of 30 months. 35 In our study success rate was 90% with surgical group and in comparison to conservative group, they required significantly shorter hospital stay, immobilization period and antibiotic administration and relatively better relief of symptoms of discitis with lesser complications rates similar to other studies. 4,19,36,37
Our observation in the patients with an early stage of pyogenic POD (within 3 weeks of onset of symptoms) treated surgically by immediate debridement after confirmed diagnosis gives better outcomes. In contrary to it, the late or advanced stage POD (associated with neural element compression, crossed endplate barrier to vertebral body, instability and kyphotic deformity) required radical and aggressive debridement along with IBF and PI for improvement and/or maintenance of sagittal balance. 27,34,38 –40 Some authors also recommended early surgical debridement followed by IVA is superior to traditional treatment with antibiotics alone. 38,41 Same was true in case of conservative treatment, if treatment starts within 2 weeks of the symptom onset, a 6 weeks treatment could be sufficient, but when delayed for a mean of 6–7 weeks after the appearance of symptoms, antibiotic treatment for 4–8 weeks is associated with an increased recurrence rate compared to treatment for 12 weeks and over. 14
The most important problem in the treatment of POD is the infection itself and the development of instability or deformity. In contrast, by surgery, all infectious foci of IVD could be removed, deformity corrected and stability was provided by putting pedicle screws and rods. Intraoperative smears and tissue sample were taken for histopathological and microbiological assessment. Therefore, surgery in combination with IVA provide better infection control, maintains spinal stability and results in better outcomes than antibiotic treatment alone. Nowadays, two different surgical procedures can be applied: one is less invasive surgery (LIS) and other one is classic open surgery. LIS can be done either by CT-guided or by endoscopically. Both are technically demanding but offer good results when applied early. 34
Open surgery, still the gold standard, particularly used in cases of large bone destruction and can be done preferably by posterior approach. Use of instrumentation in presence of active infection after radical debridement remains controversial but Korovessis et al. 42 showed no recurrence of deep infection in 14 operated cases of pyogenic infections. In our study we did not observe any relapse or persistence of infection following instrumentation. Moreover, instrumentation helped in stabilizing the infected spine more effectively and hastens the healing process. 39,40 Almost all the patients had significant pain relief immediately after surgery and returned to their normal daily activities within 6 months.
The incidence of fusion rate with bone graft is 97%, without bone graft is 90% after debridement and chemotherapy alone without surgery solid fusion may be achieved in 65–79% cases. 18 Other studies showed that debridement combined with PI and fusion using ACBG achieves a fusion rate 93–96% with excellent clinical outcomes. 4,33,41 We achieved 89.5% IBF within 12 months although there was delay [n = 2 (10.5%)] in operative group. In conservative group spontaneous IBF within a year was observed in only 26.3% cases probably due to less osteogenic potential to induce spontaneous fusion in pyogenic spondylodiscitis than tuberculous spondylodiscitis. 6
Conclusion
Although insignificant, early surgical intervention provided better results (e.g. functional outcomes, shorter hospital stay and shorter antibiotic therapy) and can be recommended over conventional conservative treatment in post-operative discitis.
Footnotes
Acknowledgements
The authors thank Dr Shahidul Islam Khan for his assistance in material collection and secretarial works. They are also grateful to Chairman, Department of Orthopaedic Surgery, BSMMU, for his technical support.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.