
Abstract
Study Design
Prospective Study.
Objectives
There are numerous techniques for performing lumbar discectomy, each with its own rationale and stated benefits. The authors set out to evaluate and compare the perioperative variables, results, and complications of each treatment in a group of patients provided by ten hospitals and operated on by experienced surgeons.
Methods
This prospective study comprised of 591 patients operated between February-2017 to February-2019. The procedures included open discectomy, microdiscectomy, tubular microdiscectomy, interlaminar endoscopic lumbar discectomy, transforaminal endoscopic lumbar discectomy and Destandau techniques with a follow-up of minimum 2 years. VAS (Visual Analogue Score) for back and leg pain, ODI (Oswestry Disability Index), duration of surgery, hospital stay, length of scar, operative blood loss and peri-operative complications were recorded in each group.
Results
Post-operatively, there was a significant improvement in the VAS score for back pain as well as leg pain, and ODI scores spanning all groups, with no significant distinction amongst them. When compared to open procedures (open discectomy and microdiscectomy), minimally invasive surgeries (tubular discectomy, interlaminar endoscopic lumbar discectomy, transforaminal endoscopic lumbar discectomy, and Destandau techniques) reported shorter operative time, duration of hospital stays, better cosmesis, and lower blood loss. Overall, the complication rate was reported to be 8.62%. Complication rates differed slightly across approaches.
Conclusion
Minimally invasive surgeries have citable advantages over open approaches in terms of perioperative variables. However, all approaches are successful and provide comparable pain relief with similar functional outcomes at long term follow up.
Keywords
Introduction
A lumbar discectomy is one of the most common spine surgery performed by spine surgeons worldwide. Mixter and Barr1,2 reported their surgical findings at the New England Surgical Society Annual Meeting in 1933, which transformed the management of lumbar disc herniations. Endoscopic lumbar discectomy was first proposed by Kambin and Savitz 3 in 1973. M. Gazi Yasargil, 4 in 1977, published his findings on 105 patients with herniated lumbar discs operated using a microscope. In the same year, Caspar 5 presented his findings in 102 individuals, who were operated by adding a medial facetectomy to the decompression surgery. In the late 1970s, Robert Willians 6 popularised this surgery, replacing the conventional incision with a minuscule one and by utilising specialised sophisticated instruments. The surgeons were awarded with exceptional magnification of the operating field with the aforementioned techniques, owing to which they could seamlessly perform surgeries using a smaller incision, without causing significant soft tissue injury. In 1997, Foley and Smith 7 introduced an operative endoscope with the tubular system, and they dubbed it “endoscopic discectomy.” Subsequently, in 2003, Foley updated the tubular retractors to include a microscope, coining the term “microtubular discectomy” for these techniques. Since the late 1990s, multitude of endoscopic treatments have been carried out, including transforaminal and interlaminar approaches, both of which involve the use of continuous water irrigation. There is a plethora of known lumbar discectomy methods, with each having its own justification and purported advantages.8-11 Each method is intended to alleviate symptoms with minimal risk of complication(s). There is a widespread notion of “one technique being better than the other,” despite the fact that existing literature shows poor evidence regarding the claim. The pros and cons of each method are different, and so are the complexities they entail. 12 In addition to documenting the results of individual procedures, the literature13-15 also includes few scattered comparison studies.9-11,16-20 The present study serves as an extended prospective analysis wing to a similar retrospective analysis published in 2021. 21 The authors ventured to assess and compare the perioperative factors, outcomes and complications of each procedure in a population of patients contributed by 10 centres and operated by experienced surgeons.
Methods
Ethics clearance was obtained after thorough discussion with the Ethics Review Board at Bombay Hospital and Medical Research Centre, Mumbai (approval number BH-EC-0137). Informed consent was obtained from all participants before participating in the study and regarding publishing their data.
Salient Features of Each Surgical Technique.
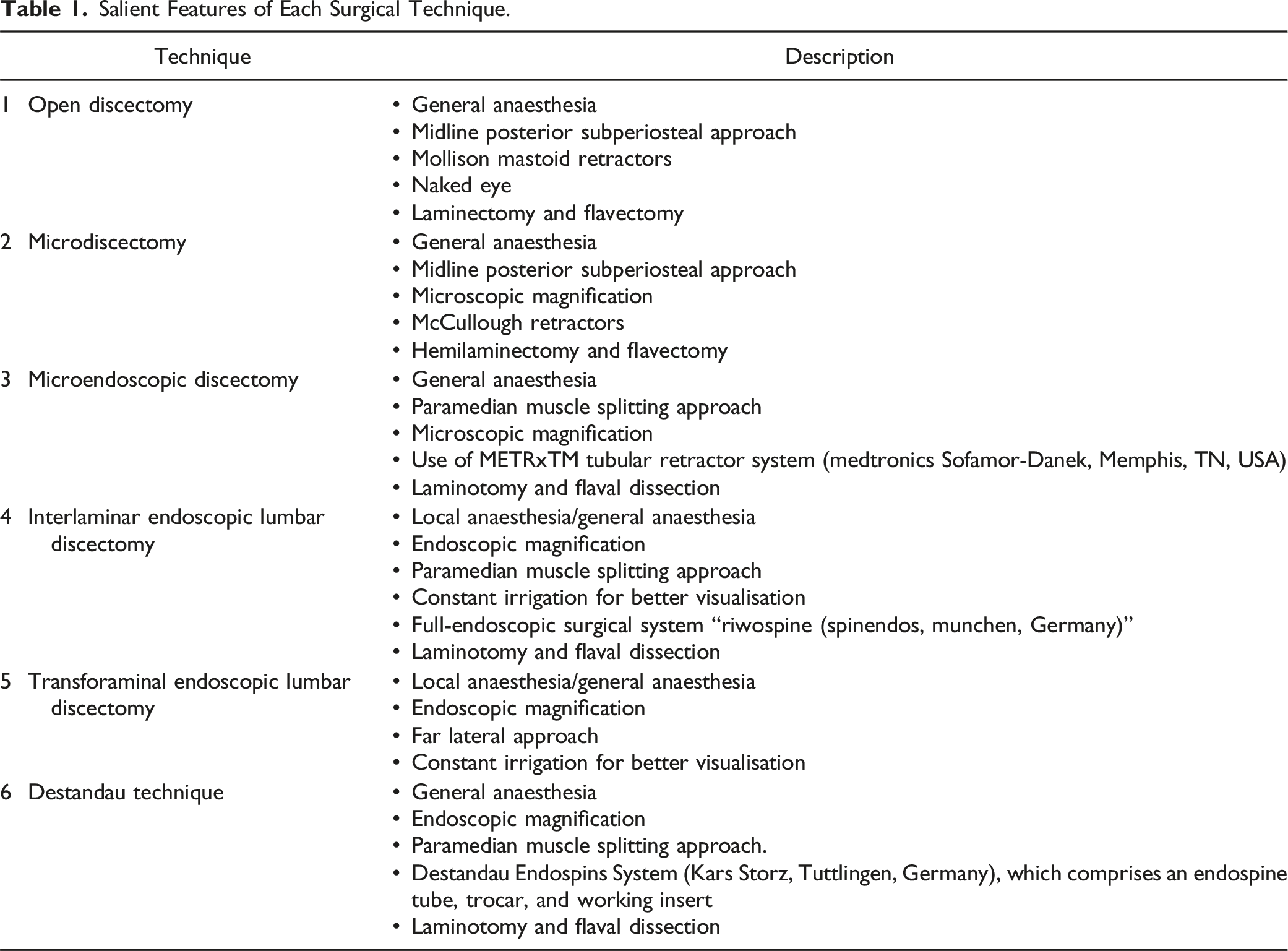
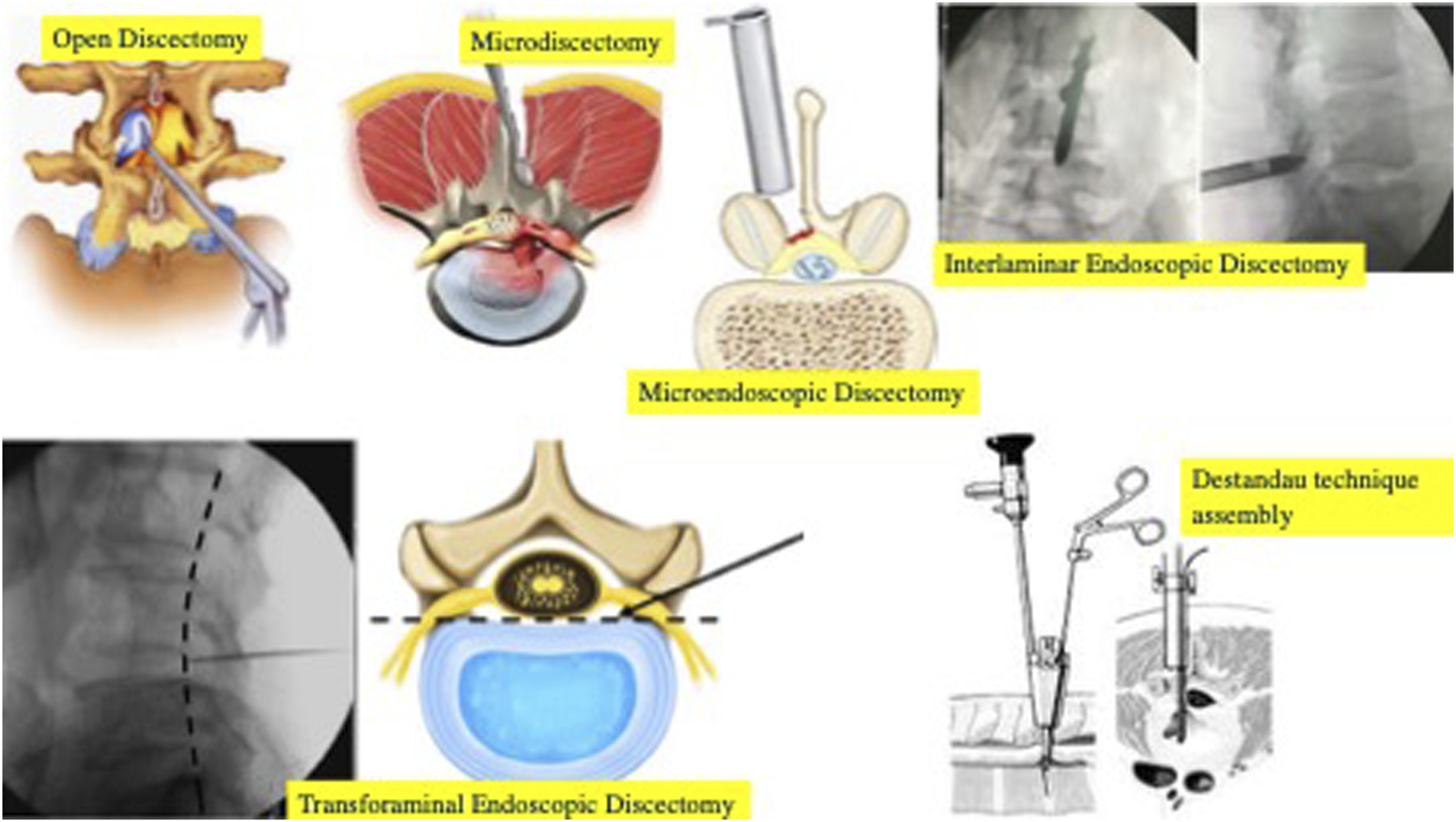
Illustration depicting the differences in the assembly and approach of each technique. 21
Inclusion criteria included lumbar segment involvement at a single level, in a person greater than 15 years of age, with symptoms and signs indicating radiculopathy, and failure of any form of conservative treatment for at least 6 weeks in.
Exclusion criteria included the presence of concomitant instability in the form of translation and angulation as seen on dynamic plain radiographs, spondylolisthesis and/or stenosis with or without claudication symptoms, and radiological evidence of stenosis on magnetic resonance imaging (MRI). The Visual Analog Scale (VAS) of leg and back pain, and the Oswestry Disability Index (ODI) were noted in the pre-operatively and at 6 month, 1 year, and 2 years post-operatively. Peri-operative variables such as operative time, blood loss, duration of hospital stay, and size of incision were recorded and compared across groups. The incidence of total and individual complications was assessed during the peri-operative and follow-up period. Data was summarised using descriptive statistics, while categorical data was represented using frequency and percentage. The X2 test with the Pearson test was used for comparative analysis. All analysis was performed with SPSS (Version 25.0., IBM Corp, Armonk, NY, USA), and a P value <.05 was considered as statistically significant.
Results
Demographic Data.
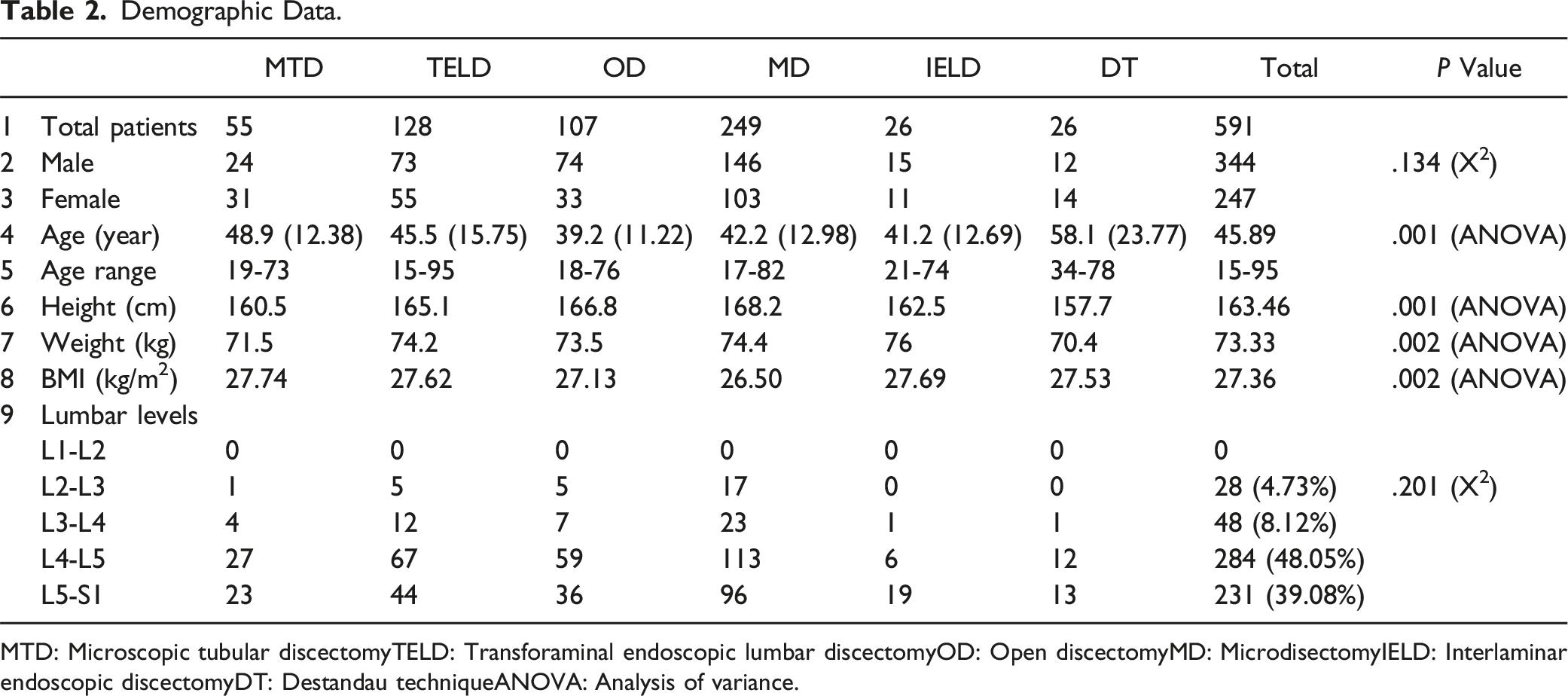
MTD: Microscopic tubular discectomyTELD: Transforaminal endoscopic lumbar discectomyOD: Open discectomyMD: MicrodisectomyIELD: Interlaminar endoscopic discectomyDT: Destandau techniqueANOVA: Analysis of variance.
Functional Outcome.
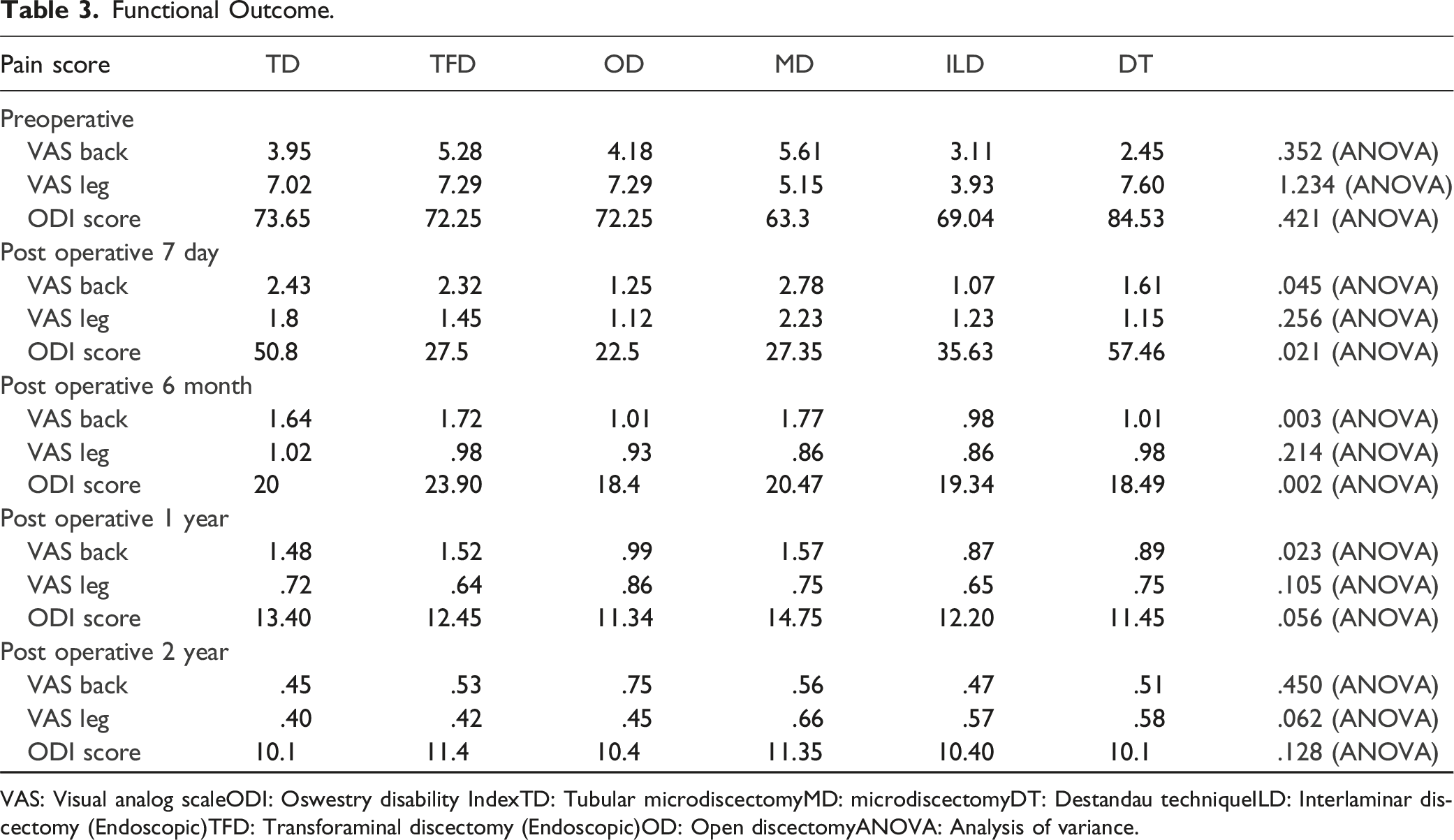
VAS: Visual analog scaleODI: Oswestry disability IndexTD: Tubular microdiscectomyMD: microdiscectomyDT: Destandau techniqueILD: Interlaminar discectomy (Endoscopic)TFD: Transforaminal discectomy (Endoscopic)OD: Open discectomyANOVA: Analysis of variance.
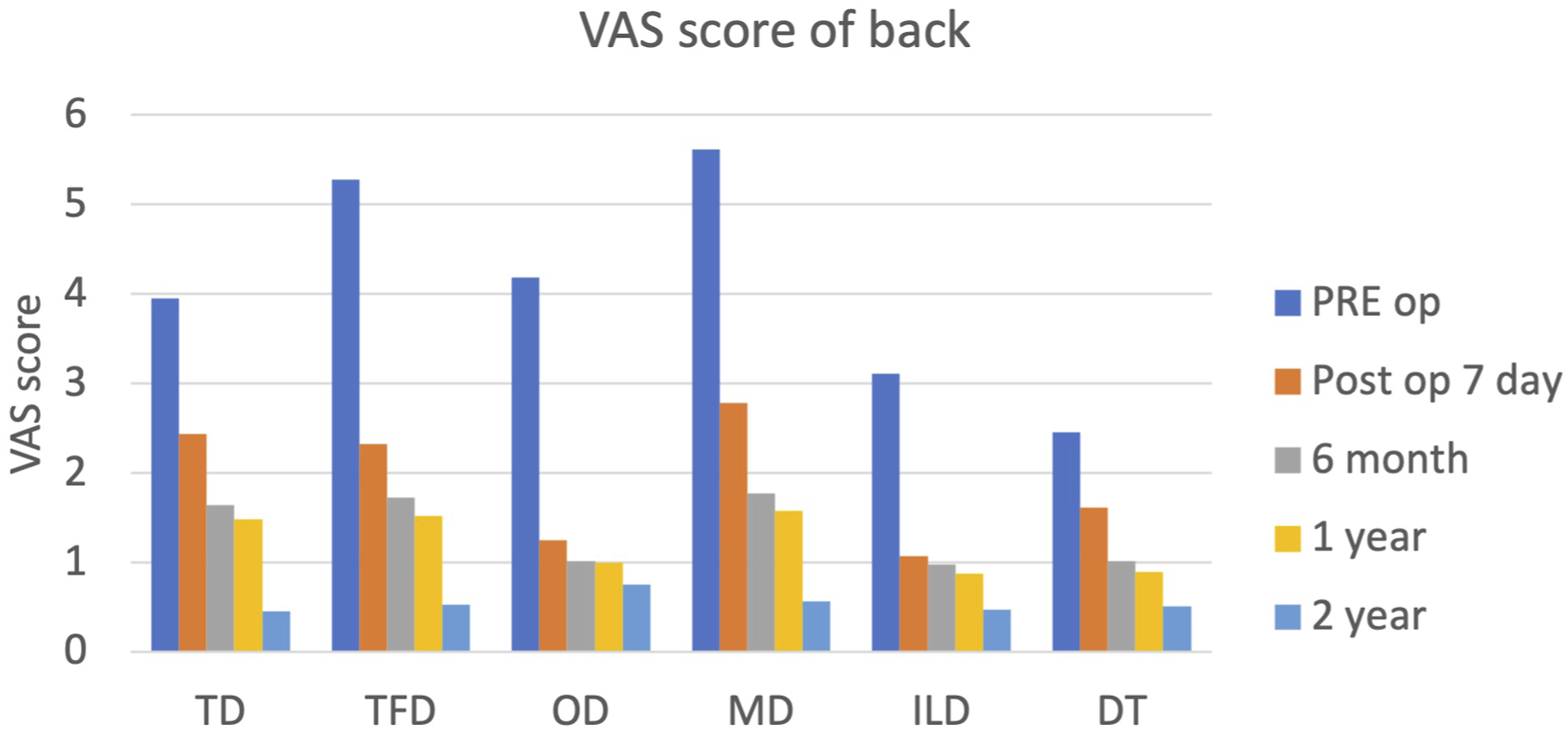
Shows VAS score of back pre-operatively and post operatively at 1 week, 6 months, 1 year and 2 years follow-up. All techniques fared well with relief in back pain at the end of 2 years.
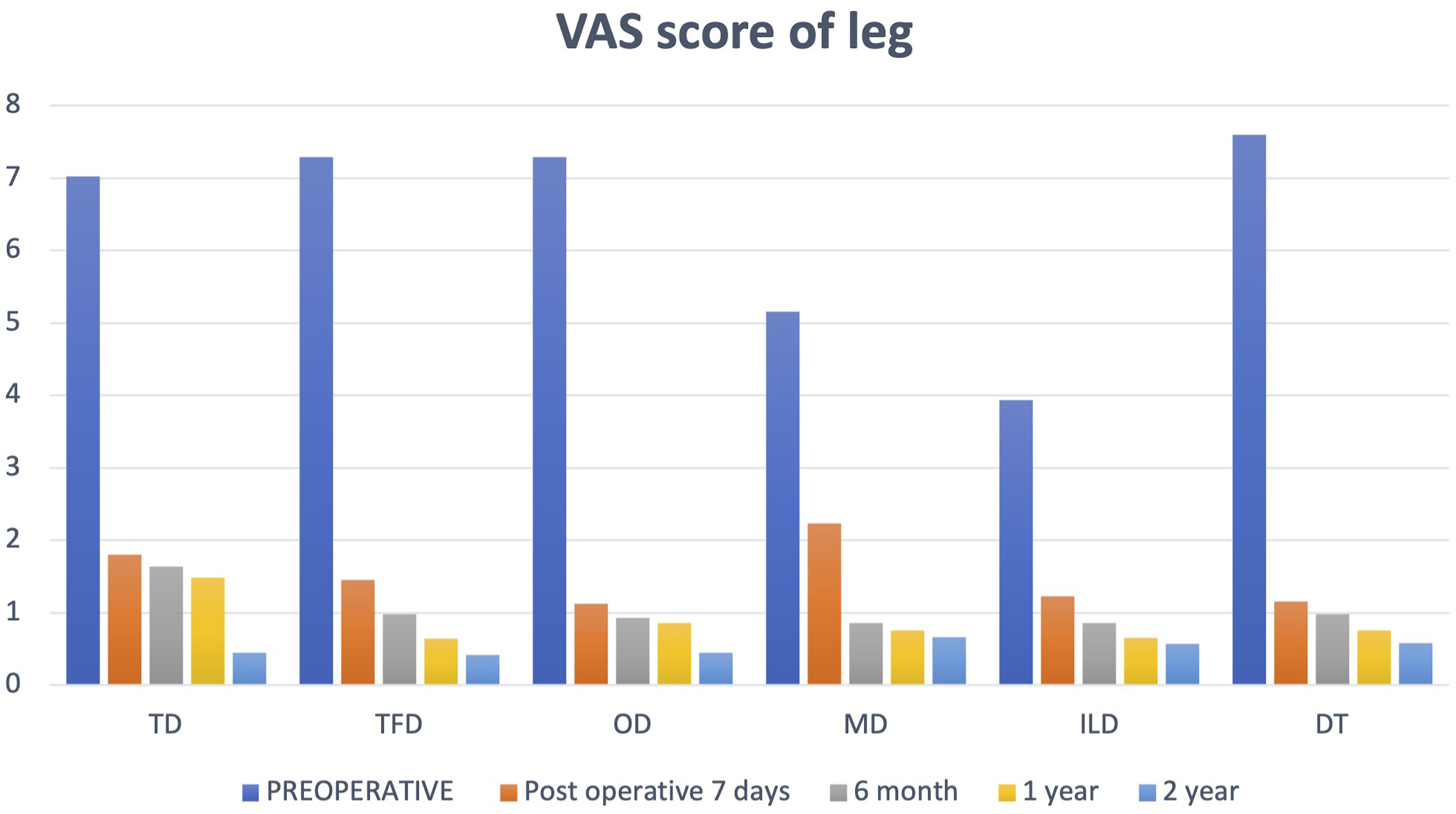
Shows VAS score of leg pre-operatively and post-operatively at 1 week, 6 months, 1 year and 2 years follow-up. Almost similar outcome was observed with each technique in terms of relief in leg pain.
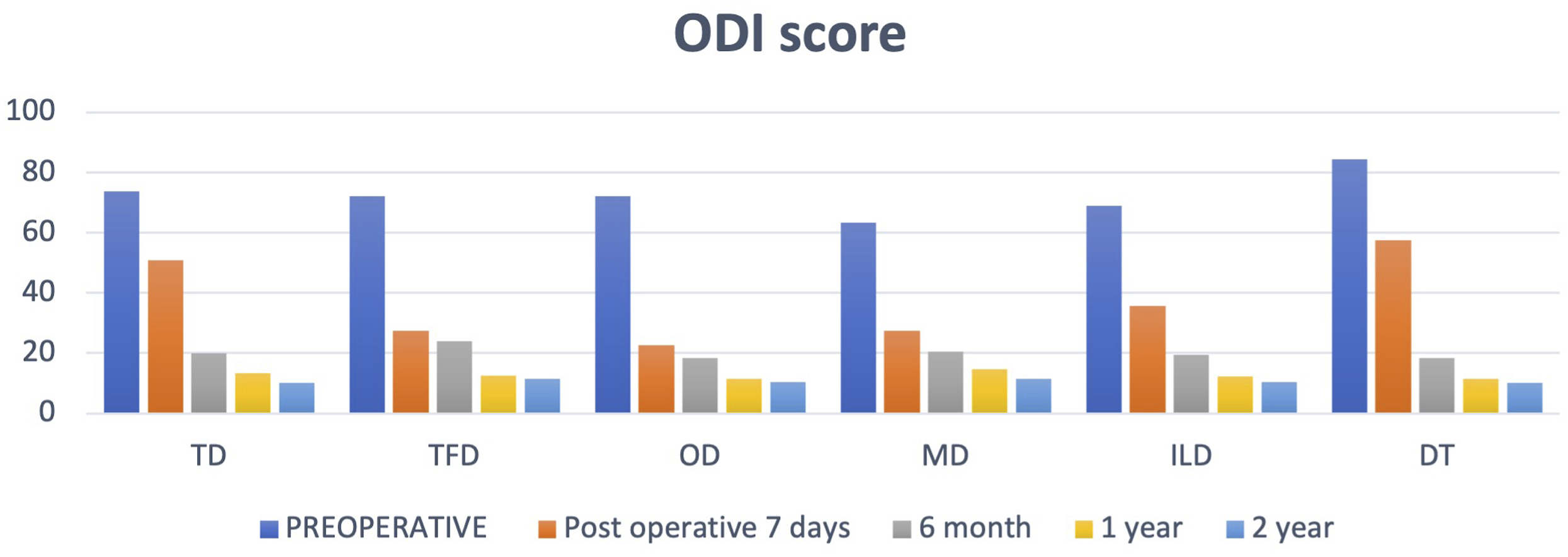
Shows ODI score pre-operatively and post-operatively at 1 week, 6 months, 1 year and 2 years follow-up. There was no clinical and statistically significant difference between the outcomes of each technique in terms of ODI score.
Surgical Outcome.
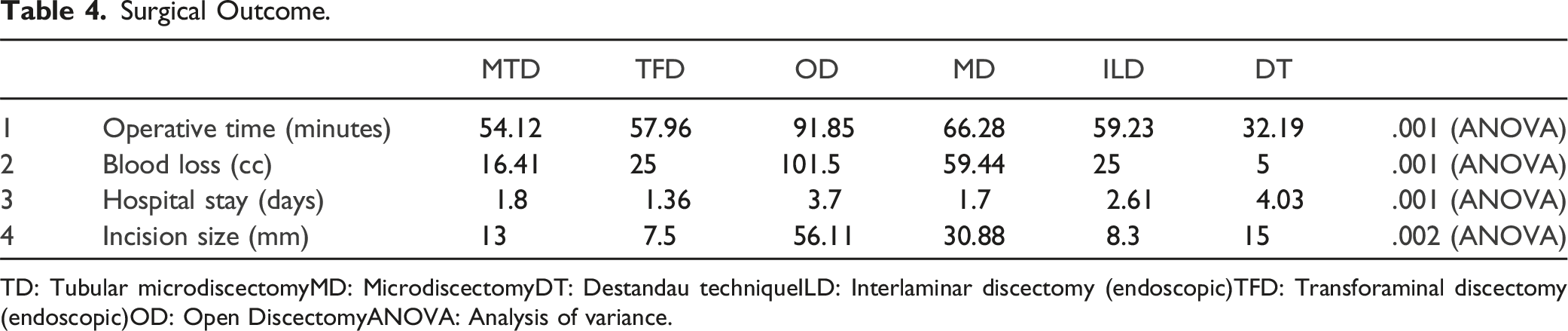
TD: Tubular microdiscectomyMD: MicrodiscectomyDT: Destandau techniqueILD: Interlaminar discectomy (endoscopic)TFD: Transforaminal discectomy (endoscopic)OD: Open DiscectomyANOVA: Analysis of variance.
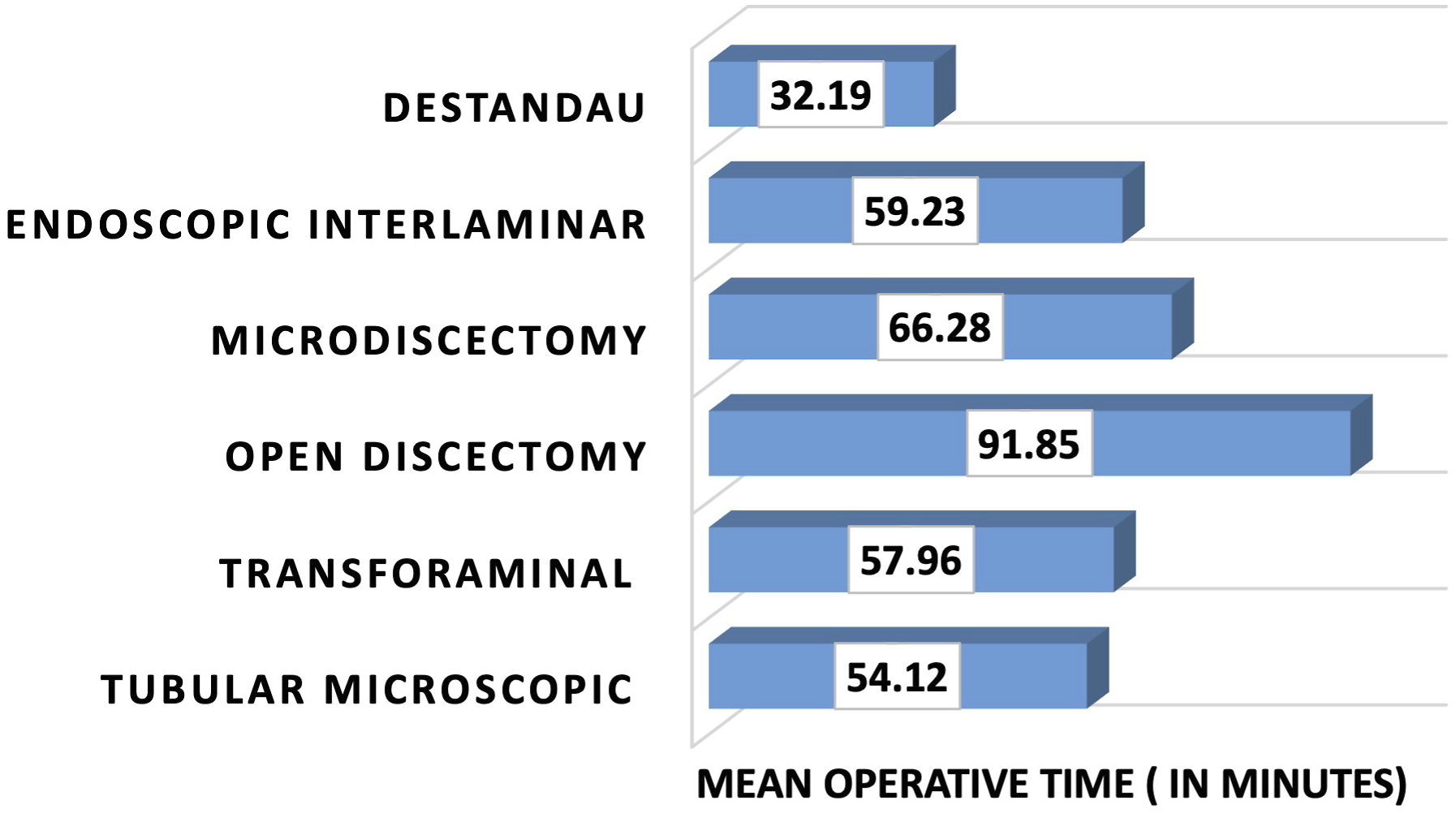
Shows mean operative time (in minutes) required for each technique. Mean operative time was maximum in Open discectomy group (OD) (91.85 min) and was minimum in Destandau technique group (DT) (32.19 min).
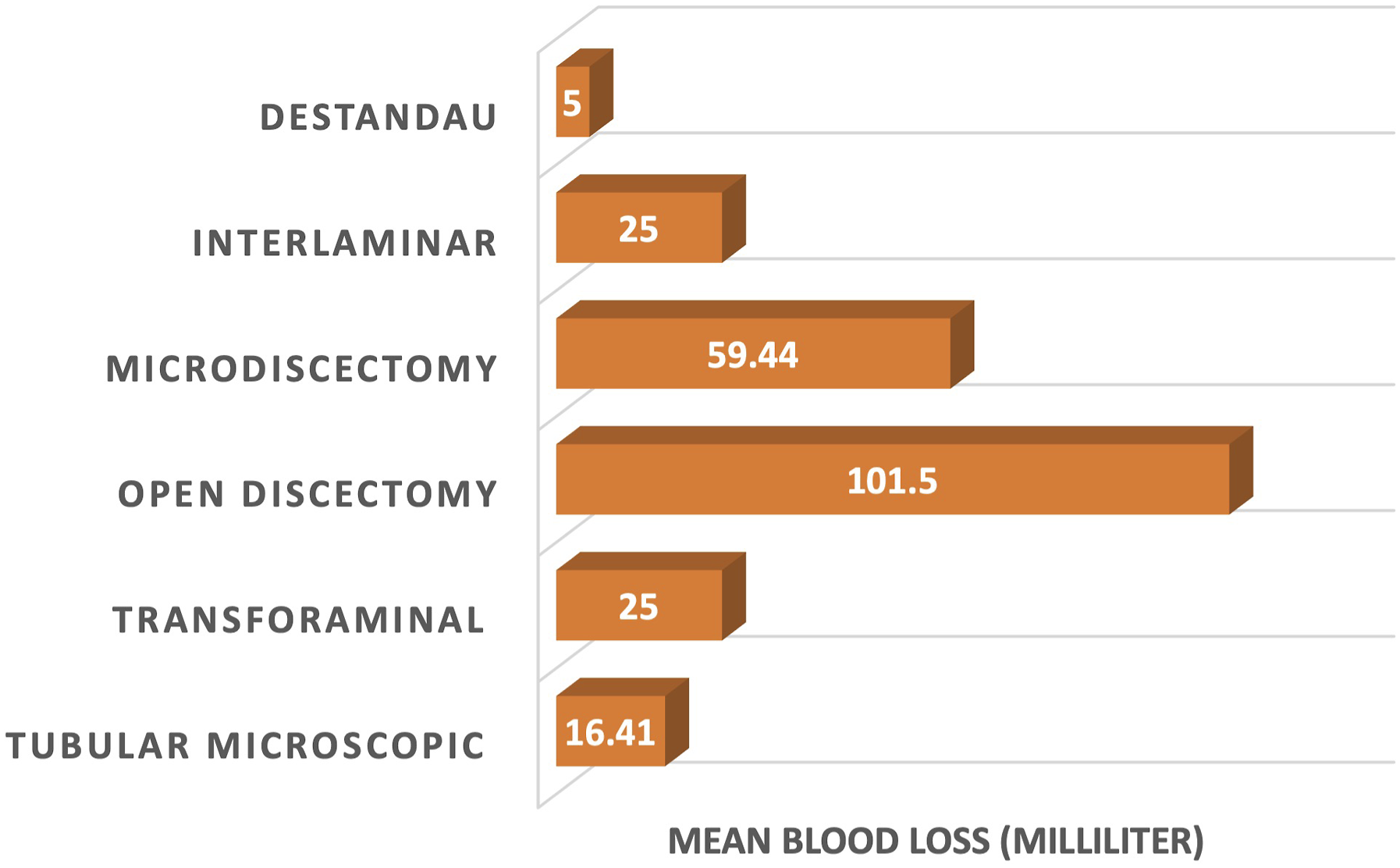
Mean intra-operative blood loss (in mL) in different groups. Blood loss was maximum in open discectomy group (OD) (101.5 mL) and least with Destandau technique (DT) (5 mL).
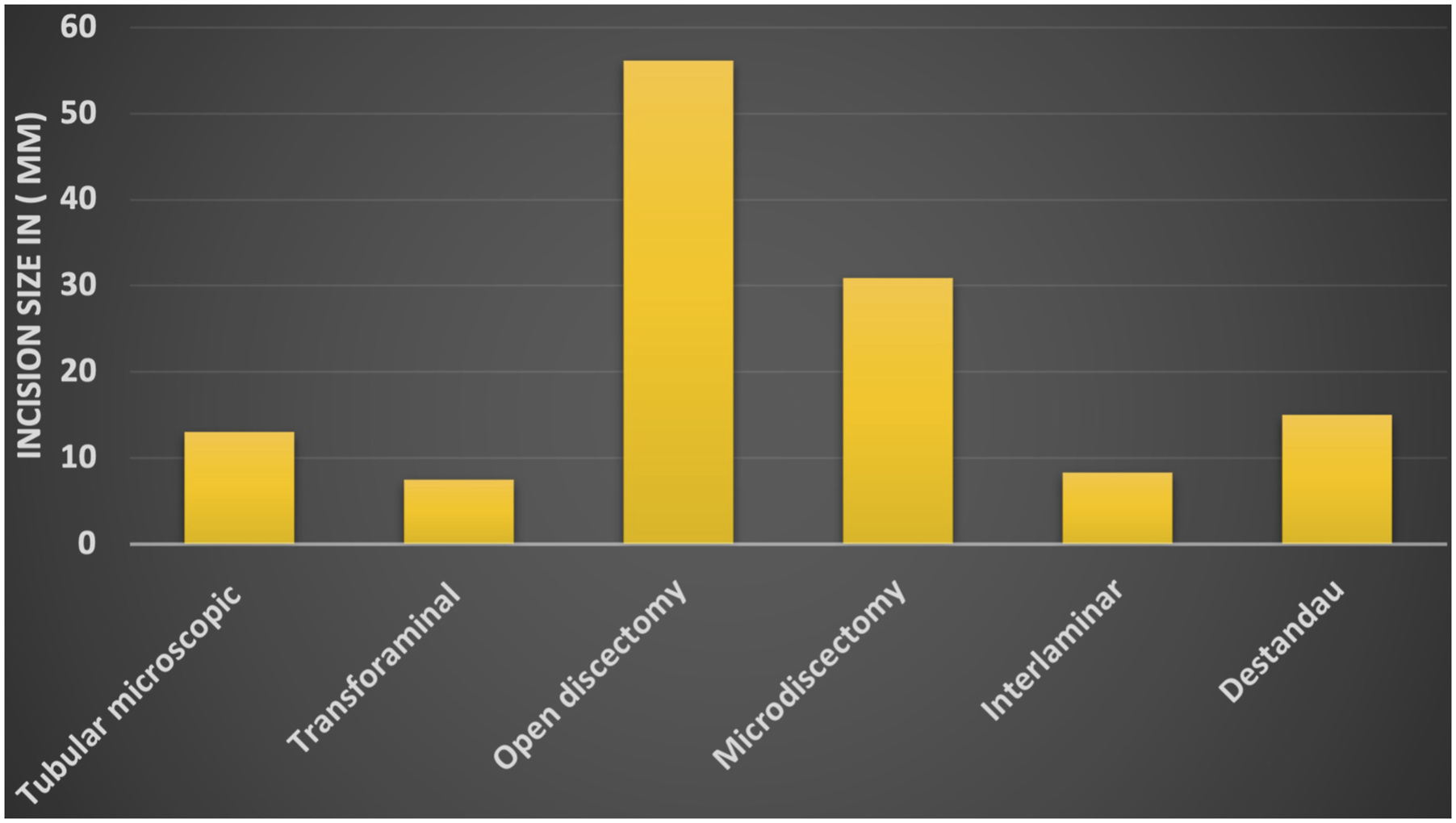
Shows mean incision size in different groups. As expected, incision length was maximum in open discectomy group (OD) followed by other minimal invasive techniques.
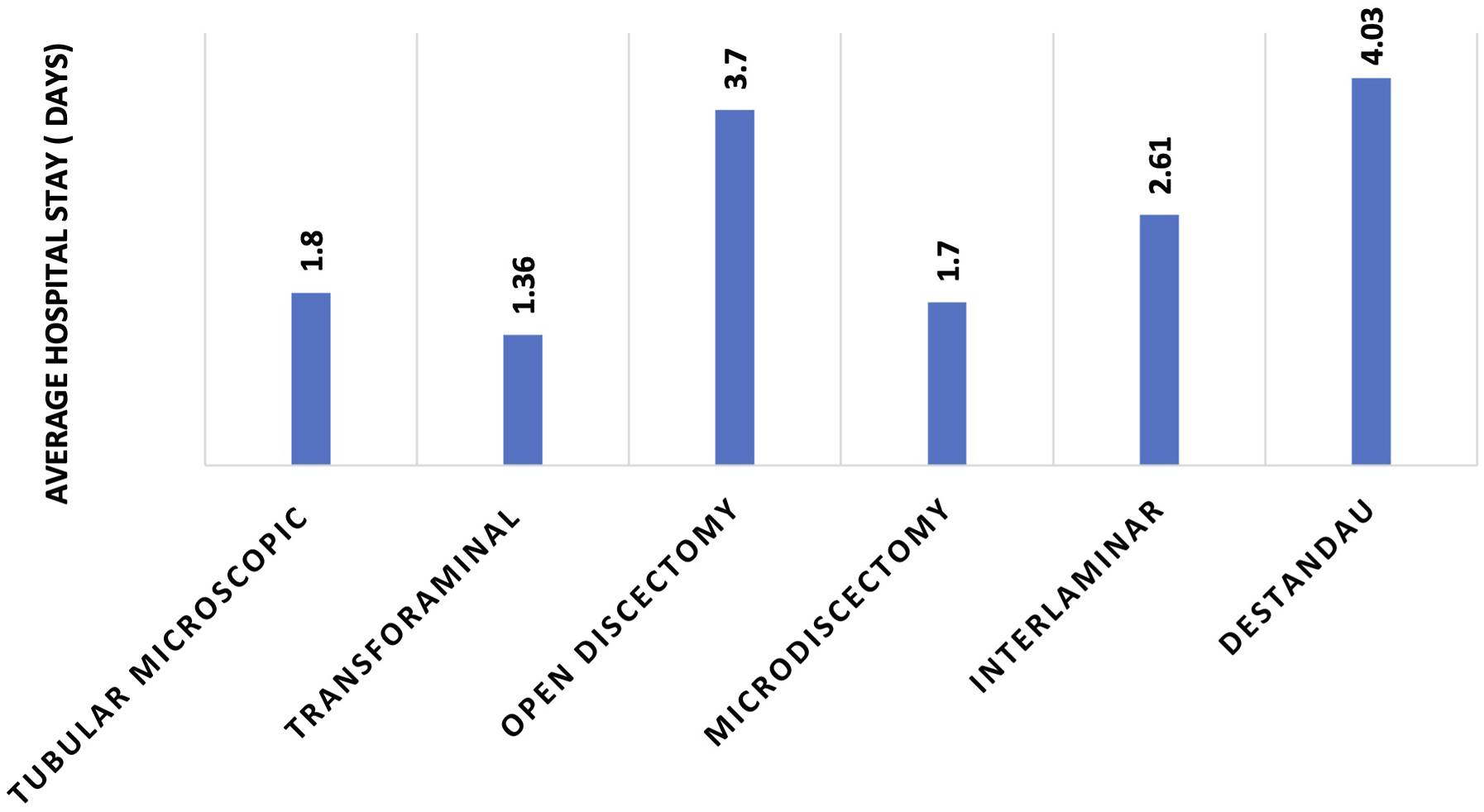
Shows mean hospital stay (in days) in different groups. Hospital stay was highest in Destandau technique (DT) (4.03 days) followed by open discectomy (OD) (3.7 days). However, this was also influenced by the local practices and patient preferences at each centre across India.
Total Complications.
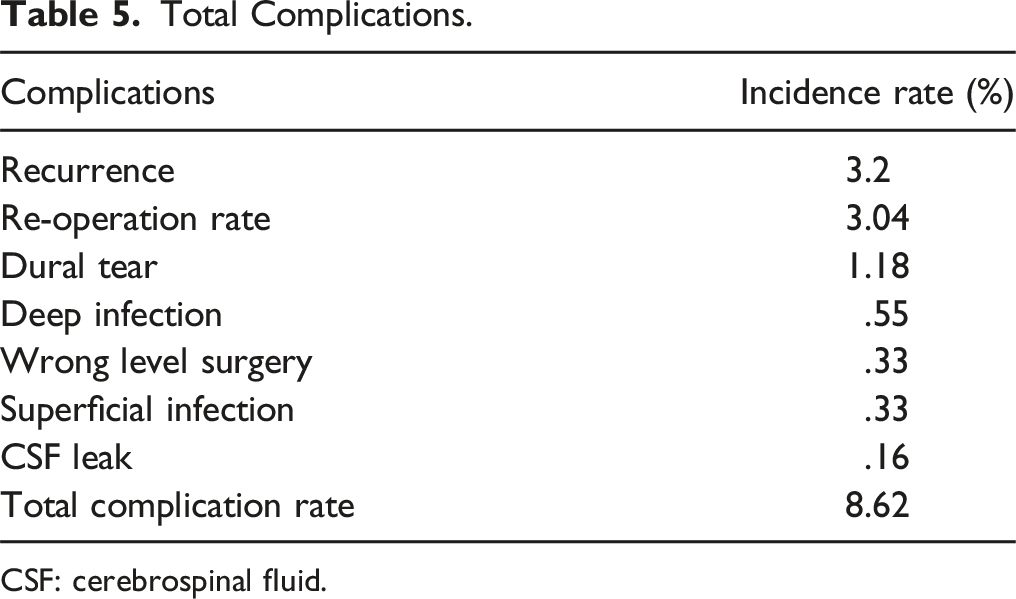
CSF: cerebrospinal fluid.
Individual Complications.
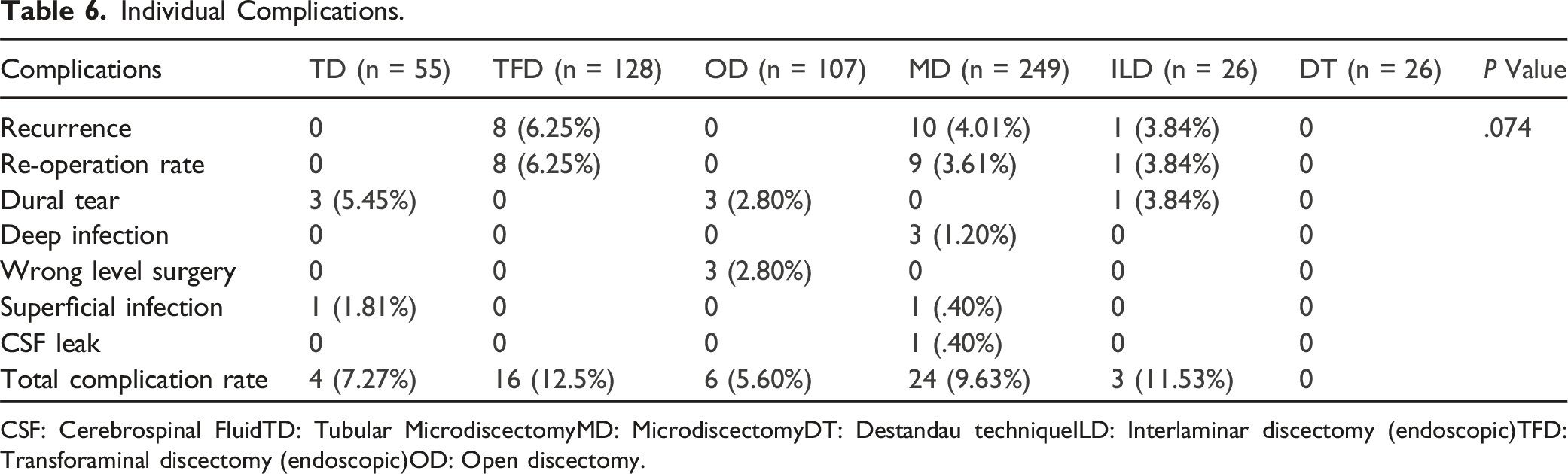
CSF: Cerebrospinal FluidTD: Tubular MicrodiscectomyMD: MicrodiscectomyDT: Destandau techniqueILD: Interlaminar discectomy (endoscopic)TFD: Transforaminal discectomy (endoscopic)OD: Open discectomy.
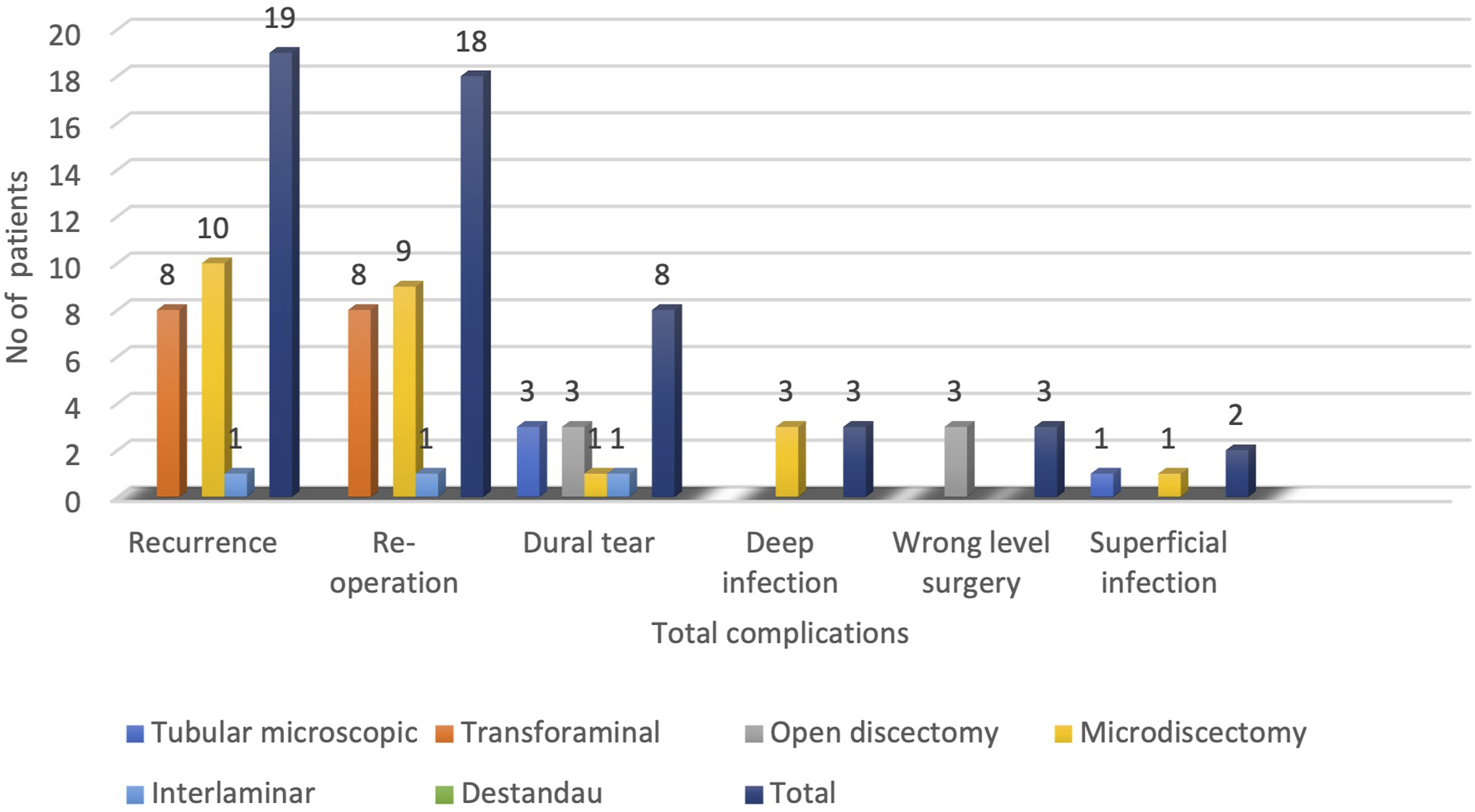
Shows the distribution of individual complications within each technique. There was no statistically significant association between surgical technique and complications.
Discussion
Lumbar discectomy can be performed in a variety of methods. 19 There are a number of advantages that minimally invasive techniques have over the conventional substitutes.8-11 Outcomes of each technique have been documented in the literature,13-15 along with comparative studies of a select number of techniques in various permutations and combinations.9-11,16-19 In the present study, patients received enrolment from ten different centres across India, and they were operated on by surgeons with at least 5 years of experience, thereby enhancing the external validity of the study. It is thereby safe to assert that the present study provides substantial evidence regarding the outcomes and complications of various discectomy techniques. Table 2 shows that the Microdiscectomy (MD) technique was used the most frequently in the present study, while Inter-laminar endoscopic discectomy (IELD) and Destandau (DT) techniques were used less frequently. This was simply because more spine surgeons are familiar with MD than with more recent techniques like IELD and DT. Instead of outcome superiority, this is solely explained by the latter’s longer learning curve. Since most spine surgeons receive basic surgical skill training in the MD approach at the beginning of their careers, many surgeons still prefer to follow it. As mentioned previously, to ensure the external validity of the study, all surgeries were performed only by surgeons who had a minimum of 5 years’ experience in their practice of choice. The present study found no evidence that the surgeons’ affinity to the approach they used while operating was influenced by their age.
At the end of the 2-year follow-up period, there was no statistically significant difference between VAS (back), VAS (leg), and ODI scores (Table 2). The current study demonstrated that all surgical techniques result in a favourable outcome at long term follow-up, with no clinically or functionally significant differences between the groups.10-12,17,19 At the end of 2 years, VAS (back) reduction was comparable across all groups. However, there was slight superiority in the VAS (back) in Minimally Invasive groups in the initial post-operative period. These findings directly corelate with the corresponding reduced soft tissue injury. These findings are consistent with those found in previous research data.10,11,17,19,22,23 At the end of the final follow-up 2 years after surgery, there was no statistically significant difference between the groups with regard to ODI score improvement.10,11,16,17,19,22,24 Maximal recovery was observed within the first 6 months post-surgery.
Our research indicated that the “Minimally Invasive group” had similar efficacy in terms of surgical outcome, with certain advantages in terms of operative time, blood loss, duration of total hospital stay, and cosmesis when compared to the “Open group” (Table 3). The operational time for the “Minimally Invasive group” in the current investigation was cut down by the use of a tubular retractor and/or endoscope. While this is in line with certain previous studies,8,17 it also contradicts few others. 13 The clearer surgical field made possible by the magnification of the microscope and/or endoscope and precise use of direct bipolar coagulation in the minimally invasive group surgeries, may in fact logically account for the shortened operative time. On the other hand, the “Open group” may have had a longer operative time due to the additional steps of exposure, haemostasis, and closure. According to our findings, the Destandau technique had the shortest operating time. 19 The remaining techniques fell in the middle of the spectrum. In this study, the OD group experienced substantially greater blood loss than the MD group (insert Figure 6). 25 Tubular (TD) and endoscopic (TFD and ILD) surgeries have minimal incision size as compared with OD and MD techniques (insert Figure 7). This can be a significant deciding factor for an individual’s choice between two techniques. In the present study, patients who underwent minimally invasive surgical techniques involving TFD/ILD or TD procedures had a shorter duration of hospital stay than those who underwent OD techniques (insert Figure 8).19,26 However, this was not due to the invasiveness of the surgery or the patient’s recuperation time, but rather due to non-medical factors such as the insurance system and the institute’s postoperative protocols. 26 Academically, the advantages of using a microscope or endoscope for discectomy were superior as the residents and fellows could visualise the surgical field in the same way as the operating surgeon, which was not feasible with the OD technique. This unquestionably accelerated the students’ surgical knowledge acquisition and clarified their conceptual understanding.24,27
As shown in Table 5, various complications were observed with each technique used in this study, with the total complication rate being 8.62% (Table 5).
Recurrence was the most common complication observed across all techniques (3.2%); and it was safe to conclude that regardless of the invasiveness of the procedure, recurrence may occur. Higher rate of recurrence was seen in TFD group as compared to MD group (P > .05). However, this is most likely related to the segment’s stability and other risk factors, such as patient characteristics, the size of the annular defect, the volume of the disc, etc. 26 Reoperation was the second most prevalent complication following recurrence (3.04%). Regardless of technique, the incidence of reoperation was between 12% and 20%. 28 Recurrence, instability, wrong-level surgery, lingering residual symptoms, and non-surgical factors like patient age and lack of compliance with post-operative precautions were among the many hypothesised causes for the same. 28 Dural tears (incidence 1.18%) were another common set of complications leading to cerebrospinal fluid (CSF) leakage peri-operatively. It was noteworthy that the incidence of this frightful complication was nil in the endoscopic trans-foraminal (TFD/ILD), microdiscectomy (MD) and Destandau approach groups and was highest in the tubular discectomy (TD) group. The statistical evidence, however, was not robust enough to conclude that solely microscope magnification was critical in avoiding Dural tears. The incidence of both deep and superficial infections was relatively low (.55% and .33%). This could be due to the approach’s low morbidity, the comparatively shorter duration of surgery resulting in less soft tissue retraction time, and the absence of implants in the surgery. Potential sources of infection in minimally invasive surgeries performed with a microscope or endoscope include the drapes used for covering the image intensifier and procedural equipment(s), 29 while in open surgeries, the greater dead space and wider tissue exposure may pose a greater threat of infection.29,30
Despite the profound medico-legal consequences of wrong-level surgery being more apparent in specific surgical techniques, there was no true statistically significant difference between the two groups. The ghastly complication of a wrong-level surgery typically occurred in open discectomies where the level was checked before the skin incision was made. Due to the need for repeated imaging guidance until the endoscope or tubular retractor was positioned over the targeted field of interest, minimal access procedures can almost eliminate the possibility of carrying out the discectomy at the incorrect level. 31 In this study the least common complication was CSF leak (.16%).
The study's undeniable strengths were its large sample size and an extensive 2-year post-operative follow-up, both of which made it possible to efficiently compute incidences and outcomes in a single study and also ensured strong external validity.
Among the limitations acknowledged by the authors, first is the absence of an analysis of peri-operative cost incurred. The inclusion of cost-benefit and cost-effective analyses, as well as a comparison of techniques in these terms, may influence the patient’s choice of procedure. The inclusion/exclusion criteria did not specify the anatomical location of the disc herniation, which was another important limitation of the study. The study included foraminal and extraforaminal herniations as well as posterolateral, central, cranially, and caudally migrated herniations. One of the primary reasons for including this assortment was to assure a high number of cases. The authors later saw value in classifying foraminal and extraforaminal herniations as distinct entities because the transforaminal endoscopic technique is a straightforward solution to the latter group of herniations. Due to the non-uniform availability of patients fitting in the defined inclusion criteria, there was disparity in the total number of cases operated by each technique. However, as mentioned earlier this was done to include as many patients as possible and assure a large sample size to reduce the window for a statistical error. It is indirectly inferred in the study that the most common technique used by spine surgeons is MD technique. Lastly, the authors acknowledge that the study did not reflect the incidence of disc prolapse at various lumbar levels; upper lumbar disc herniations are occasionally treated with fusion. Additional research in this area could contribute to a more thorough analysis and improved decision-making.
Conclusion
This is the first prospective comparison of all presently utilised lumbar discectomy techniques. Although minimally invasive techniques have certain advantages over open techniques in terms of peri-operative variables, all techniques are equally effective and provide comparable pain relief and functional outcomes in the long run. The varying rates of individual complications serve as a benchmark for future research.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.