
Abstract
Background:
Defining the appropriate threshold at which to initiate a fever workup is imperative to promote patient safety, appropriate resource utilization, and antibiotic stewardship. Our group performed a systematic review of the available literature on perioperative fever (POF) workups in orthopaedic patients to evaluate the frequency, timing and utility of blood cultures (BC) and other investigations in the POF workup, to determine the clinical relevance of any infections and to evaluate their cost effectiveness.
Methods:
Studies were identified by searching MEDLINE, EMBASE, Pubmed, Cochrane and Google Scholar for articles through September 2016. Forty-nine articles were retrieved and 22 articles met the pre-determined inclusion criteria. Proportions of positive studies were noted and averaged using random effects analysis.
Results:
Post-operative pyrexia ranged in prevalence between 8.1% and 87.3%. The studies routinely performed during a fever workup had wide ranges of diagnostic yield, including chest X-rays from 0% to 40%, urinalyses from 8.2% to 38.7%, urine cultures from 0% to 22.4% and BC from 0% to 13.3%. Only two patients with positive BC developed clinical sepsis. Cost per fever evaluation ranged from $350 to $950.
Conclusion:
The findings of this review suggest that early post-operative fever is an expected event following orthopaedic surgery. Based on the available literature, any kind of workup in the absence of localizing symptoms in the third post-operative day or before is unwarranted and is an inappropriate use of hospital resources.
Introduction
Post-operative pyrexia is a well-described and yet continually vexing phenomenon. Surgeons and intensivists are often at odds about the appropriate workup and treatment of post-operative fevers (POFs). In general, surgeons have observed that pyrexia in the first few days post-surgery is common, and only very rarely associated with an infectious condition. 1 –23 Intensivists, on the other hand, are more familiar with systemic illness in which a fever indicates a significant finding which merits intervention.
The discrepancy is important not only from an appropriate use perspective but also in a larger public health perspective. As antibiotic resistance among common pathogens grows, 24 –26 often our options shrink for caring for the sickest groups of patients. We must restrict antibiotics to situations where we are reasonably sure an infection exists and pursue workup for infection only when there is a reasonable chance that we may find one. Blood cultures (BC) and other studies are often ordered on post-operative orthopaedic surgery patients who are in the intensive care unit, and it has been our observation that these studies only rarely provide a meaningful contribution to patient care, but more often result in the patient being placed on antibiotics in anticipation of the study results.
The first aim of this study was to determine the frequency, timing and utility of BC and other investigations for POF in the early post-operative period following orthopaedic surgery. The second aim was to determine whether any of these cultures revealed clinically significant infections. The final aim was to collect data on the cost effectiveness of the perioperative fever workup.
Methods
Two of the authors (BA and KB) independently carried out a comprehensive search of the MEDLINE, EMBASE, PubMed, Google Scholar and Cochrane computerized literature databases (through September 2016) for level 1–4 studies which looked at pyrexia in the early post-operative period in patients having major orthopaedic surgery. The medical subject headings (MeSH terms) used were ‘post-operative fever’ or ‘post-operative pyrexia’ and ‘orthopaedic’ or ‘orthopedic’. Reviewers traced the bibliographies of the retrieved articles, including review articles, for citations missed by the electronic search. The senior investigators (KB and PJC) also reviewed their personal files and associated bibliographies for additional citations.
Study selection
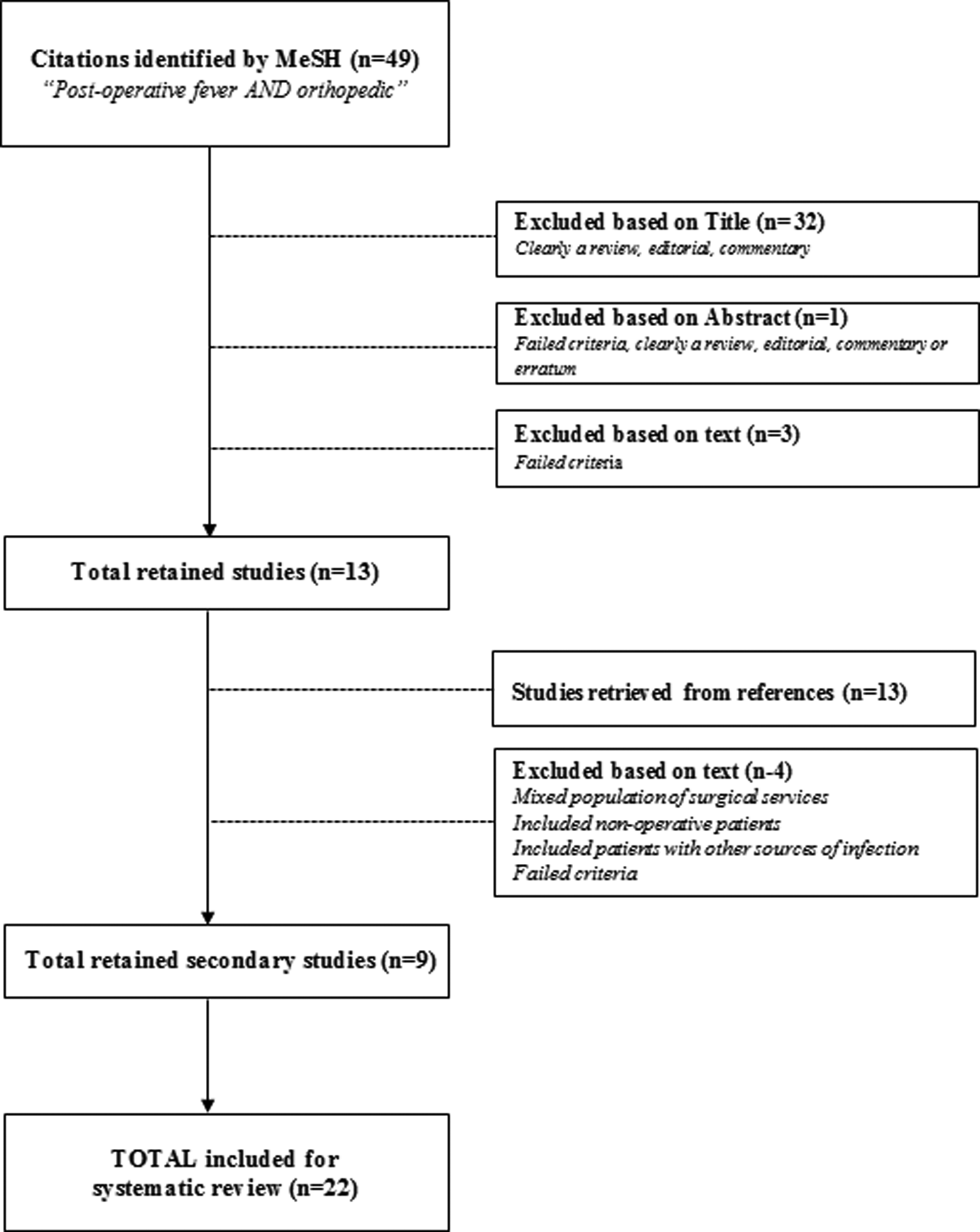
Two of the authors (KB and BA) reviewed the abstract titles for relevance and determined which articles potentially contained relevant information. If an article was deemed eligible by either reviewer, the abstract was retrieved and reviewed in full. Only studies published in English were reviewed. Studies were included if they described (1) a minimum of five subjects (i.e. not a case report); (2) patients underwent major orthopaedic surgery in which there was a hospital admission; (3) data regarding post-operative pyrexia and workup; (4) patients were followed a minimum of 3 days; (5) studies were a level-I–IV therapeutic or prognostic study design. Studies were excluded if they (1) did not meet the above inclusion criteria; (2) were not performed on human subjects; (3) did not perform additional workup for fevers or did not include pyrexia as an outcome; (4) orthopaedic patients could not be separated from non-orthopaedic patients. The review of pertinent abstracts was performed by two of the authors (BA and KB). If any abstract was deemed relevant by any reviewer, the full text of the article was reviewed by the same reviewers. All disagreements were resolved by consensus and if necessary consultation with a tie-breaking reviewer (PJC). Details of the search are included in Figure 1.
Data extraction
Two of the authors (KB and BA) independently extracted data, including general information (author and year of publication), type of study, type of patients, details of hospital course and fever workup, along with results if available of any fever workup performed. These datapoints were extracted from the papers and placed in a database. No assessment of methodologic quality was performed as these studies were largely uncontrolled case series. Forty-nine studies were identified by the primary search. Of these, 36 were eliminated by title or abstract as an editorial, review, commentary or papers which had nothing to do with the topic. Three studies were reviewed by two reviewers (BA and KB) and determined not to be appropriate for the study. Two of these studies were not in English and the full text article of the third paper was no longer available. Thirteen more studies were identified by secondary search of the selected papers’ references, but four were discarded because they did not meet inclusion criteria for reasons including a mixed population of surgical services, including non-operative patients and including patients with pre-existing sources of infection. A total of 22 papers were selected for review.
Data analysis and synthesis
We recorded simple percentages and proportions of patients with POF and those who were worked up with each type of study (BC, urine cultures (UC), urinalysis (UA), chest X-ray (CXR) and wound cultures). We assessed for the general prevalence of a positive study within each of the member studies. These were added together to formulate a fixed effects proportion of each. Data on positive BC were also presented. Raw proportions were assembled for each subpopulation of patients (total joints, paediatrics and trauma) using fixed effects adjustment. Total raw proportions for all orthopaedic populations were assembled using random effects modelling to account for inter-study variation and funnel plots showed minimal publication bias with respect to our primary interest (BC), as highlighted in Figure 2. A heterogeneity analysis was performed which showed minimal study heterogeneity I2 p value (0.4884). We performed random effects modelling for the data which included the Yoo study 23 because of the large N relative to the other studies. Meta-analysis was performed using MedCalc for Windows, version 15.0 (MedCalc Software, Ostend, Belgium).

Results
Details of the member studies are highlighted in Table 1. Post-operative pyrexia ranged in prevalence from 8.1% to 87.3% (adjusted mean 40.9%). 2,4 –9,11 –18,20 –23,27 –29 Tables 2 –5 highlight test characteristics of the fever workup. CXRs were associated with a diagnostic yield of 0–40% (adjusted mean 0.3%). 2,4,6,14,15,22,23,28 UA was associated with a diagnostic yield of 8.2–38.7% (adjusted mean 28.5%). 2,4,6,14,15,22,23,28 UC were associated with a diagnostic yield of 0–22.4% (adjusted mean 10.9%). 2,4,6,14,15,22,23,28 BC were associated with a diagnostic yield of 0–13.3% (adjusted mean 3.5%). 1,2,5,6,11,14 –16,21 –23,28 Of the 686 BC drawn, only 24 were positive (see Appendix 1 for summary table; out of 686 drawn). 5,6,14,16,21 –23,28 Only two patients with positive BC had clinical sepsis, two BC were specified to be contaminants in the study and one was found on post-operative day (POD) 16. The remainders were not well described in the studies. The raw proportions and fixed effects adjustment data for our primary interest, BC in the setting of POF, are detailed in Table 6. Most studies did not include information on associated costs; however, based on the data available, the cost associated with each fever evaluation ranged between $350 and $950. 5,22,23
Prevalence of fever.

BC: blood cultures; NR: not recorded; –: no data; peds/peds ortho: pediatric orthopaedics.
Test characteristics of CXR for POF.a

CXR: chest X-ray; NR: not recorded; –: no data.
aNote only studies with full data included in totals.
bStudies by Ghosh and Guinn had three + CXR both but neither had a denominator.
Test characteristics for UA for POF.a

UA: urinalysis; NR: not recorded; –: no data.
aNote only studies with full data included in totals.
bGhosh had one + UA and Guinn had eight + UA no denominator and no other data were available.
Test characteristics for UC for POF.a

UC: urine cultures; NR: not recorded; –: no data.
aNote only studies with full data included in totals.
bGhosh had one + UC acted on but no denominator.
Test characteristics for BC for POF.a
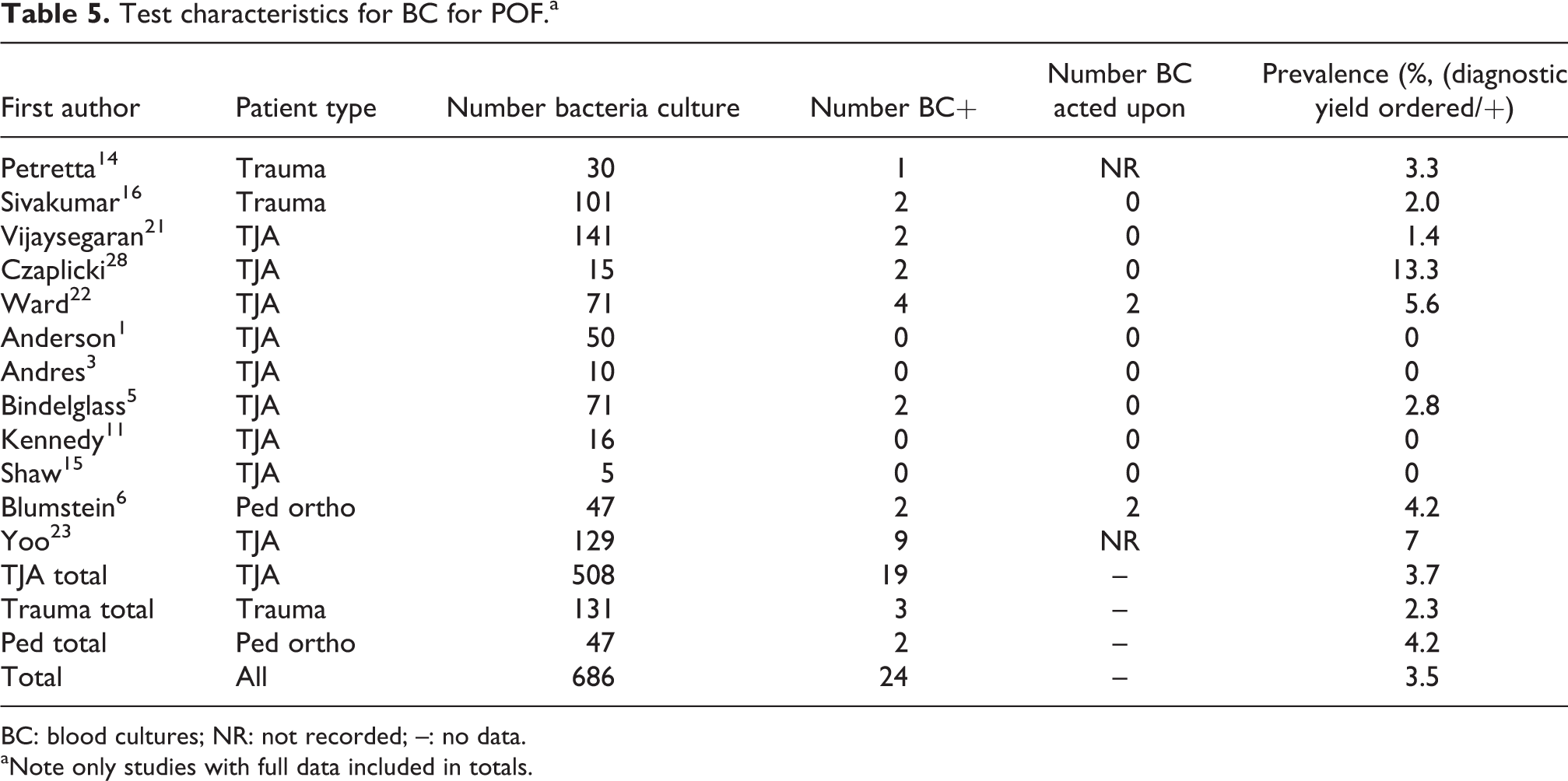
BC: blood cultures; NR: not recorded; –: no data.
aNote only studies with full data included in totals.
Details on patients in studies with BC.

BC: blood cultures; CNS: coagulase negative staphylococcus; FNF: femoral neck fracture; NR: Not recorded; –: no data; PSF: posterior spinal fusion; SSI: surgical site infection; TJA: total joint arthroplasty.
Discussion
Post-operative pyrexia is an exceedingly common event, and its significance in the early post-operative period has been debated. Post-operative fever has been postulated to be secondary to the inflammatory cascade initiated by surgery, 2,29 the physiologic stress of surgery, 30,31 the presence of infectious processes, as well as non-infectious processes such as DVT, phlebitis, atelectasis and acute post-operative anemia. 4,27,32 These post-operative febrile events initiate a generalized fever workup in adult and paediatric orthopaedic patients following a myriad of procedures, even in the absence of patient symptoms. However, the execution of a generalized fever workup increases the cost of hospitalization and potentially prolongs hospital stay, despite having low diagnostic yield. In addition, normative data concerning the clinical correlates of the post-operative host inflammatory response, such as temperature, are unavailable for orthopaedic surgical procedures, making it difficult to predict normal from abnormal. The purpose of our systematic review was to critically evaluate the significance of the early post-operative fever, the utility of the diagnostic workup and the cost effectiveness of the tests typically ordered.
Fever workups, in general, were very low yield in the published literature. Previous studies have shown that the positive rate of a routine diagnostic workup is as low as 2.4–14.8%. 3,19,22,23 BC yielded a very low percentage of positive results. Based on our review, of the 24 positive BC, only 4 were definitively acted upon, 8 were known to be contaminants and the rest were unaccounted for. 1,5,7,11,16,21,28 Other diagnostic studies ranged in yield with BC being on the low end (0–13.3%; inverse variance average 3.5%) and UA being on the high end (8.2–38.7%; inverse variance average 28.5%). Studies were unclear as to whether or not the positive results were acted upon; as such the sensitivity and specificity of these tests are impossible to calculate. However, because the prevalence of positive BC was so low, it is likely that any positive result is likely to be a contaminant (false positive), and not helpful in patient management. This is further supported by the observation that there were no instances of positive BC being associated with a subsequent superficial or deep surgical site infection. As such, it is our observation that BC are not predictive of long-term sequelae related to the orthopaedic procedure, or even of a short-term clinically significant event which requires medical management.
In addition to being low yield from a diagnostic perspective, fever workups generate a significant cost to the healthcare system. 5,19,22,23 CXRs are a costly element of the routine diagnostic workup, and Yoo et al. estimated that over $4 million dollars was wasted over a 12-year period due to negative CXRs alone. 23 Yoo et al. estimated an annual hospital savings of $386,000 if these workups were not performed. 23 Of note, all cost estimates are likely underestimated because they only account for the cost of the studies performed and do not take into consideration the expense of prolonged hospital stays secondary to waiting for lab results. Finally, antibiotic resistance may occur when broad spectrum antibiotics are reflexively given in response to early post-operative fever or in fear of future surgical site infection. 24 This result may constitute an ‘unforced error’ on the part of the treating physician as continuing antibiotics past the 24-h prophylactic period has been shown to be ineffective. 24 –26,33
Adopting a more stringent approach to the management of perioperative fever will minimize the number of unnecessary tests endured by patients while also reducing costs. Febrile events during the first 3 post-operative days, in the absence of localizing symptoms, do not merit a diagnostic workup as they occur in 50–87% of patients. 4,6,7,14,17,20,23 Ishii et al. found that post-operative fever in the first 3 days following total joint arthroplasty is exceptionally common. 9 The rate of post-operative fever drops precipitously after that, but does not become zero. 9,17,18 Febrile events occurring after POD 3, in patients undergoing revision total joint arthroplasty, and encompassing temperatures greater than or equal to 102°F should be treated with increased suspicion. 10,12,14,15,18,22,23 Additionally, patients who experience multiple febrile episodes were found to be more likely to have a positive finding upon diagnostic workup. 22,23 Finally, unless patients exhibit pulmonary symptoms, a CXR need not be obtained as part of the initial diagnostic workup given the expense of the test and its exceedingly low yield. 4,23
Certainly, this review has several limitations, mostly due to weaknesses of member studies. Primary of which is the inability to identify true or false positives and negatives in the member studies. Were this possible, we could derive test parameters for each part of the fever workup to better inform decisions regarding which studies are worth the cost and potential downside. As mentioned, the absence of normative data or post-operative temperature curves for a variety of procedures in adults and children clouds the matter further. Additionally, studies utilizing CXRs depend on radiologist reads, and urine and BC suffer different vulnerabilities depending on the lab in which they are performed. Even with these weaknesses, we feel our review provides a comprehensive review of this commonly encountered clinical scenario and can guide treatment decisions.
Conclusion
In conclusion, our systematic review supports the notion that early post-operative fever is an expected event following orthopaedic surgery as part of the usual inflammatory cascade which occurs due to acute injury. We feel that any kind of workup in the absence of localizing symptoms under the third post-operative day is unwarranted based on the available literature. At that time, patients who experienced multiple febrile episodes, febrile episodes with temperatures ≥102°F or who underwent revision surgery are at the greatest risk of having an underlying infection. The efficient utilization of hospital resources including inpatient services, costs and antibiotics is contingent upon a symptom-specific workup of early post-operative fever in a stepwise fashion. Further research is suggested to (1) characterize post-operative temperature curves following commonly performed procedures to identify which value are outliers and (2) determine if there is any correlation between magnitude of temperature and post-operative infections.
Footnotes
Authors’ note
Research performed at The Children’s Hospital of Philadelphia (CHOP).
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article: No funding was necessary to support our investigation.
Appendix 1
Meta-analysis proportion for test characteristics of BC in POF.a

| Study | Sample size | Proportion (%) | 95% CI | Weight (%) | |
|---|---|---|---|---|---|
| Fixed | Random | ||||
| Petretta et al. 14 | 30 | 3.333 | 0.0844–17.217 | 1.49 | 1.49 |
| Sivakumar et al. 16 | 101 | 1.980 | 0.241–6.971 | 4.92 | 4.92 |
| Vijaysegaran et al. 21 | 141 | 1.418 | 0.172–5.030 | 6.85 | 6.85 |
| Czaplicki et al. 28 | 15 | 13.333 | 1.658–40.460 | 0.77 | 0.77 |
| Ward et al. 22 | 71 | 5.634 | 1.556–13.801 | 3.47 | 3.47 |
| Anderson et al. 1 | 50 | 0.000 | 0.000–7.112 | 2.46 | 2.46 |
| Andres et al. 3 | 10 | 0.000 | 0.000–30.850 | 0.53 | 0.53 |
| Bindelglass et al. 5 | 71 | 2.817 | 0.343–9.808 | 3.47 | 3.47 |
| Kennedy et al. 11 | 16 | 0.000 | 0.000–20.591 | 0.82 | 0.82 |
| Shaw et al. 15 | 5 | 0.000 | 0.000–52.182 | 0.29 | 0.29 |
| Blumstein et al. 6 | 47 | 4.255 | 0.520–14.541 | 2.31 | 2.31 |
| Yoo et al. 23 | 129 | 6.977 | 3.240–12.831 | 6.27 | 6.27 |
| TJA total | 508 | 3.740 | 2.267–5.779 | 24.54 | 24.54 |
| Trauma total | 131 | 2.290 | 0.475–6.547 | 6.36 | 6.36 |
| Ped total | 47 | 4.255 | 0.520–14.541 | 2.31 | 2.31 |
| Total | 686 | 3.499 | 2.254–5.161 | 33.12 | 33.12 |
| Total (fixed effects) | 2058 | 3.639 | 2.875–4.538 | 100.00 | 100.00 |
| Total (random effects) | 2058 | 3.639 | 2.877–4.488 | 100.00 | 100.00 |
BC: blood cultures; POF: post-operative fever; ped: paediatric.
aNote only studies with full data included in totals.