
Abstract
Background
This retrospective study was conducted to assess the clinical outcome and complications between tension band wiring (TBW) with eyelet wire and locking plate fixation used for the treatment of displaced olecranon fractures.
Methods
A total of 58 patients (36 males and 22 females; mean age: 63 years) were reviewed between April 2014 and September 2020. TBW with Ring Pin (RP group) was applied in 24 patients, including 15 Mayo type ⅡA and 9 Mayo type ⅡB patients. Anatomical locking plate (ALP group) was used in 34 patients, including 22 Mayo type ⅡA and 12 Mayo type ⅡB patients. Clinical outcome was evaluated using the Mayo Elbow Performance Score (MEPS), and active range of motion of the elbow and forearm and postoperative complications were reviewed.
Results
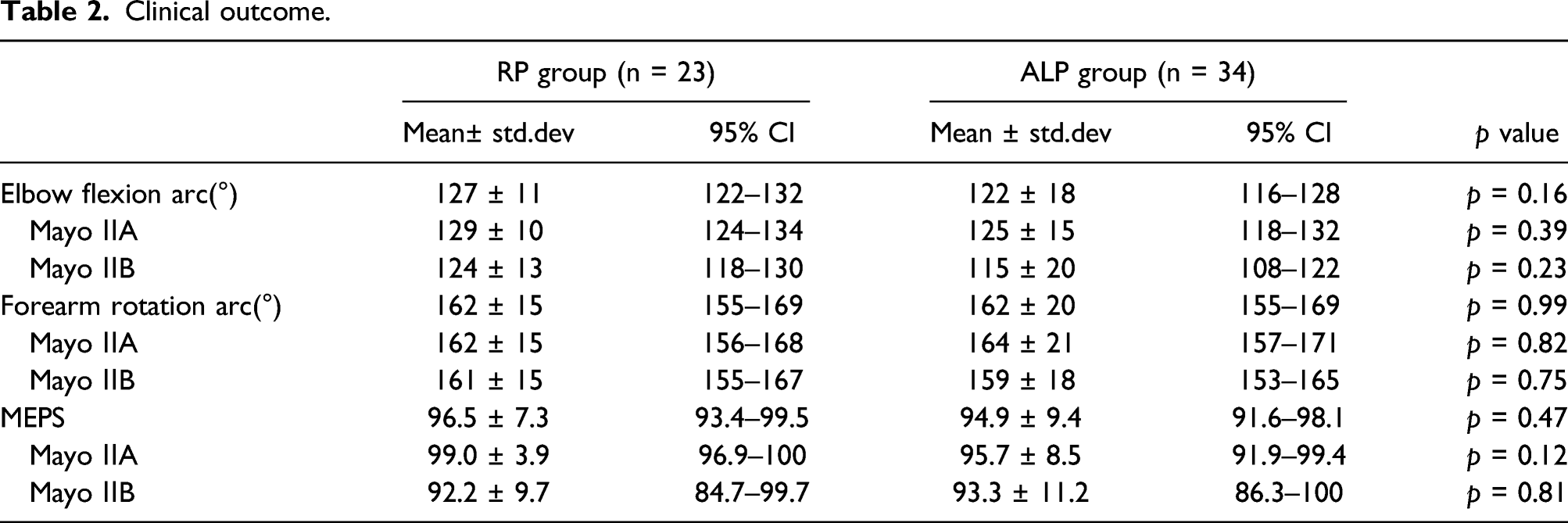
General characteristic of the patients and the fracture type were similar in the two groups. The mean MEPS values were 96.5 ± 7.3 in the RP group and 94.9 ± 9.4 in the ALP group. The mean elbow flexion arc was 127°±11 in the RP group. The mean elbow flexion arc was 122°±18 in the ALP group. No significant differences in clinical outcomes were observed between the two groups. Complication rates were significantly higher in the ALP group (19/34: 56%) than in the RP group (6/24: 25%).
Conclusion
Although there were no statistically significant differences in clinical outcomes between the two groups, the ALP group had a higher proportion of any complication than the RP group.
Keywords
Introduction
Although tension band wiring (TBW) for displaced olecranon fractures is a gold standard surgery, some authors1-4 have recently reported the efficacy of plate fixation. They demonstrated that there were no significant differences in clinical outcomes between TBW and plate fixation; however, high complication rates due to back out of Kirschner wire (K-wire) and metalwork removal in TBW were indicated. Therefore, plate fixation was recommended for displaced olecranon fractures. On the other hand, some studies have demonstrated good clinical results and low complication rates for olecranon fractures treated by TBW with eyelet wire instead of K-wire.5,6 However, to our knowledge, no clinical study has compared the outcomes between anatomical locking plate (ALP) fixation and TBW with eyelet wire. Therefore, we conducted this retrospective study to evaluate the clinical outcome and complications between TBW with eyelet wire and ALP fixation for the treatment of displaced olecranon fractures.
Materials and methods
A total of 72 patients with displaced olecranon fractures were treated between April 2014 and September 2020. The inclusion criteria of this study were (1) acute (within 2 weeks) and isolated, (2) Mayo classification type ⅡA or type ⅡB, (3) open reduction and internal fixation using either TBW with eyelet wire or ALP, and (4) at least 6 months of follow-up. Based on these inclusion criteria, eight patients with concomitant fractures, two patients with Mayo classification type ⅢB, and four patients with follow-up periods of <6 months were excluded from this study. Proximal ulnar comminuted fractures involving the coronoid process fracture were excluded from this study.
We retrospectively evaluated the data of the remaining 58 patients (36 males and 22 females; mean age: 63 years; range: 22–88 years). Surgery was performed at a mean of 3 days (range: 1–6 days) after injury. This study was approved by the local institutional review board, and informed consent was obtained from each patient. Patients with displaced olecranon fractures were treated by either TBW with eyelet wire (Ring Pin; Teijin-Nakashima Medical: Okayama, Japan) or ALP fixation. A total of 12 orthopedic surgeons performed surgeries, all of whom were supervised by the first author (HS). The choice of the Ring Pin (RP) or the ALP was dependent on the surgeons. A total of 24 patients with a mean age of 66 years (range: 22–88 years) consisting of 15 Mayo type ⅡA and nine Mayo type ⅡB patients were included in the RP group. In the ALP group, there were 34 patients with a mean age of 61 years (range: 35–82 years), including 22 Mayo type ⅡA and 12 Mayo type ⅡB patients. The A.L.P.S Elbow Plating System (Zimmer Biomet, Warsaw, USA) was used in 23 patients, and the 3.5-mm LCP olecranon plate (DePuy Synthes J&J, West Chester, USA) was used in 11 patients. Body mass index (BMI), smoking status, and the presence of diabetes mellitus were reviewed as general characteristics of the patients using electronic medical records. BMI was expressed as a person’s weight in kilograms divided by the square of the person’s height in meters.
All patients were evaluated using the Mayo Elbow Performance Score (MEPS) at a mean follow-up of 12 months (range: 6–30 months). The active elbow extension and flexion and forearm pronation and supination values were measured using a goniometer at the final follow-up. Complications were classified as major or minor. Major complications were defined as nonunion, deep incisional infection, neuropathy, heterotopic ossification, articular implant penetration, implant failure, and prominent implant with revision surgery. Minor complications were defined as delayed union (>6 months), superficial incisional infection, redisplacement (>2 mm) without revision surgery, and prominent implant without revision surgery. Asymptomatic implant removal done based on the patient’s request was not considered as a complication. Bone union was defined as the disappearance of the fracture line on plain radiographs. According to the World Health Organization (WHO), obesity implies a BMI value ≥30, overweight is defined as a BMI value ≥25, and underweight implies a BMI value <18.5 for adults. Prominent implant removal rate was evaluated between patients with a BMI value ≥25 and those with a BMI value <25.
Statistical analysis
Quantitative data were represented as mean ± standard deviation. General characteristics of the patients and complication rates between the RP group and the ALP group were analyzed using Fisher’s exact test and independent t-test. Mayo Elbow Performance Score and ROM of the elbow and forearm were analyzed by an independent t-test between the two groups. Differences were considered to be statistically significant when p values were <0.05, and two-tailed p values were reported.
Surgical technique
All surgeries were performed under general anesthesia using an arm table and C-arm in the lateral position. The C-arm was inserted parallel to the surgical bed from the patient’s foot side, and the lateral views of the elbow were confirmed by rotating the shoulder externally without moving the C-arm. The fracture site was exposed by a posterior skin incision along the ulnar axis by a radial curved incision on the olecranon. We avoided placing the implant just under the skin incision. In patients with Mayo type ⅡB fracture, the intermediate fragment was reduced at first, and then we filled the cancellous cavity with granule type of β-tricalcium phosphate (OSferion, Olympus, Tokyo, Japan). A horizontal grasping stitch by a strong suture was placed at the insertion of the triceps tendon, and fracture fragment was reduced by pulling the strong suture distally. The Ring Pin system consists of the wire with eyelet and 1.2-mm cable wire and cable fastener, and they were specially designed for TBW as a treatment approach for olecranon and patellar fractures (Figure 1). The diameter of this wire is 2.0-mm, and it is made of stainless steel. 80-mm wires were usually used for olecranon fracture; the wire has a 2.9-mm eyelet to prevent its proximal migration. In the RP group, the fracture fragment was reduced and fixed using two 2.0-mm Ring Pins. The Ring Pins were inserted to support the subchondral bone of the trochlea notch of ulnar, and the tail of the Ring Pin was broken off. A 1.2-mm designated cable wire was inserted through the eyelet, and the figure-of-eight TBW was tightened with 20 kg-force tensioner advancing the eyelet wires slightly. Finally, 1.2-mm cable wire was fixed by crimping the cable fastener. (Figure 2). In the ALP group, the fracture fragment was fixed temporarily using two 1.8-mm K-wires after the reduction of the fracture. An additional K-wire was inserted to reinforce the intermediate fragment, if required. The ALP was placed on the ulnar ridge, and the insertion of the triceps tendon was divided to prevent plate prominence. First, locking screws were inserted into the proximal fragment, and then we used the active compression technique with cortical screws in the distal slot. The distal locking screws were inserted into the distal fragment (Figure 3). Finally, a strong suture at the insertion of the triceps tendon was tied to the plate holes. The Ring Pin system is specially designed for tension band wiring. Postoperative radiographic image of tension band wiring with Ring Pin for the olecranon fracture. The intermediate fragment was reduced and the cavity was filled with β-TCP. Postoperative radiographic image of anatomical locking plate fixation for the olecranon fracture.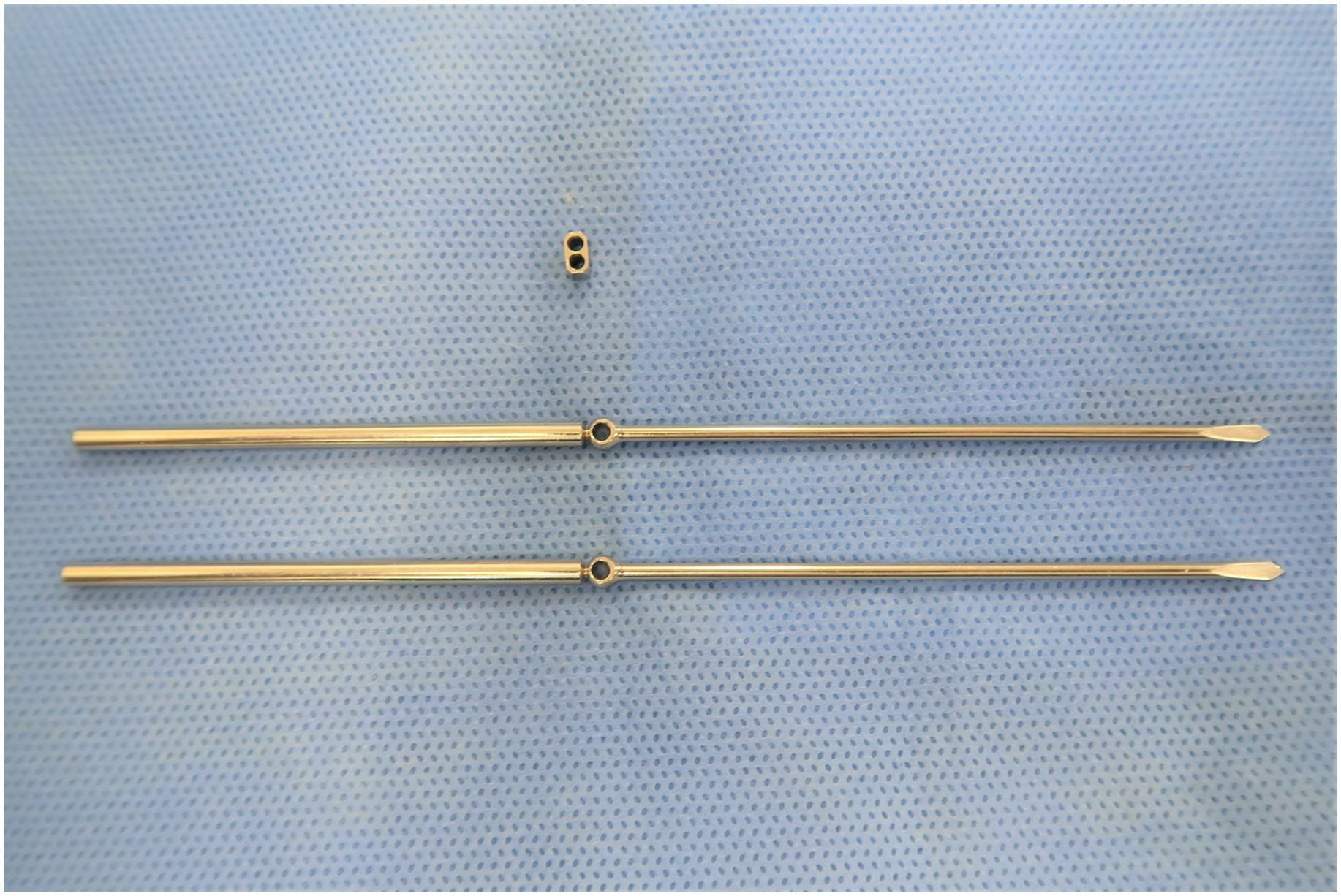


Results
General characteristics of the patients.

Functional outcomes
Clinical outcome.
Complications
Complications in two groups.

*Fisher’s exact test
In the ALP group, there were 19 major complications in 15 patients, including 12 implant removals with prominence and discomfort, two implant failures requiring revision surgery, two soft-tissue infection, one ulnar neuropathy, one heterotopic ossification in medial collateral ligament, and one articulation screw penetration. The implant was removed after bone union in two patients with two soft-tissue infections and one screw penetration. Two patients with implant failure underwent revision surgery with a different kind of ALP. There were four minor complications in four patients in the ALP group, including a superficial infection, a prominent implant without revision surgery, and two delayed unions. Asymptomatic implant removal was performed at the request of younger patients in one patient in the RP group and five patients in the ALP group.
Implant removal in each classification of BMI.

BMI: Body mass index.
Discussion
Tension band wiring for displaced olecranon fractures is a gold standard surgery, and good clinical outcomes have been reported. Recently, the plate fixation technique is widely used for simple and comminuted olecranon fractures due to advances in low profile and locking mechanisms. Some authors have reported similar clinical results between TBW and plate fixation, although TBW was associated with a higher complication rate than the plate fixation technique.1-4 Powell et al. 1 compared TBW with ALP fixation in only simple olecranon fractures and reported good outcomes with no differences in both groups. The total complication rate in the TBW group (39%: 19/48) was significantly higher than that in the ALP group (0%: 0/16), and 13 patients required implant removal for TBW irritation versus zero patient in the ALP group. Tarallo et al. 2 compared TBW with plate fixation in simple and comminuted olecranon fractures and found good outcomes with no difference between both groups; the implant removal rates were 10/33 (30%) in the TBW group and 4/45 (9%) in the ALP group. In a prospective randomized trial comparing nonlocking plate fixation with TBW for MayoⅡA fractures conducted by Duckworth et al., 4 no difference was found between the two groups in the patient-related outcome. The authors concluded that the overall complication rate was higher after TBW and was due to a higher rate of implant removal, while plate fixation led to a more serious complication of infection, requiring revision surgery. In our study, the complication rate in the ALP group was higher than that in the RP group in contrast to previous reports. No back out of the K-wire was found in the RP group, because the Ring Pin never moved proximal due to the eyelet, unless it was broken. Symptomatic implant removal rates in this study were 2/24 (8%) and 12/34 (35%) in the RP and ALP groups, respectively. Although the end of the K-wire passed through the anterior ulnar cortex to prevent the proximal migration in TBW, 7 other complications such as ulnar artery and anterior interosseous nerve injury8-10 and restriction of forearm rotation11,12 were described due to penetration of the K-wire. In the RP group, the end of the Ring Pin was inserted into the intramedullary canal, and we were able to avoid these complications. One of the advantages of Ring Pin is that the insertion of the wire at the fracture fragment is away from the fracture line. In the normal TBW technique, the insertion of the wire tends to come close to the fracture line to penetrate the anterior ulnar cortex.
Tension band wiring has been commonly used in treating simple olecranon fractures, in contrast to the indication of plate fixation that is believed to be used for comminuted olecranon fractures.13,14 Tarallo et al. 2 compared TBW with plate fixation in treating simple and comminuted olecranon fractures and reported no significant differences in the clinical outcome and complication rates in both fracture patterns. Moreover, in our study, there were no significant differences in the treatment of Mayo type ⅡB fractures between the RP group and the ALP group. Okamoto et al. 6 reported satisfactory clinical results using TBW with the eyelet wire and biodegradable pins for selected comminuted olecranon fractures.
Various factors are associated with implant removal after bone union. Yamamoto et al. 15 stated that the implant removal rate after plate fixation for distal radius fractures is dependent on the medical health insurance system of each country. For other reasons, we considered that implant irritation after bone union was associated with the site of the fracture and the thickness of the subcutaneous tissue. Bugarinovic et al. 16 reported that both lower BMI and age were associated with a higher rate of symptomatic implant removal after olecranon fracture fixation. The present study revealed significant differences in the prominent implant removal rate between patients with BMI ≥25 and those with BMI <25. BMI is not an accurate measure to evaluate subcutaneous tissue because fat and muscle mass are not taken into account; however, BMI is a simple index of weight for height and widely used to estimate overweight throughout the world. According to the report 17 of the Organization for Economic Co-operation and Development (OECD) in 2016, the proportion of obese people in Japan was only 3.7%, and the country ranked 34th among 34 countries. Furthermore, Japan has a universal health system, and hence the rate of prominent implant removal may tend to be higher.
Several limitations exist in this study, such as the retrospective design and the short follow-up. In the short follow-up, the patient who complains of the implant symptom later may come out. Moreover, we could not evaluate patient-related functional outcomes such as the disabilities of the arm, shoulder, and hand (DASH). However, to our knowledge, no clinical study has compared the outcomes between ALP fixation and TBW with Ring Pin. Although there were no significant differences in clinical outcomes between the two groups, the ALP group had a higher proportion of any type of complication than the RP group.
Conclusions
This study revealed no significant differences in the clinical outcomes between the two treatment approaches. However, the ALP group was associated with a higher rate of complications than the RP group.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.