
Abstract
Background:
Periprosthetic joint infection (PJI) is the most common complication after artificial joint replacement as previously reported. However, the main problem at present is its difficulty in diagnosis. This systematic review and meta-analysis aimed to compare the diagnostic accuracy of α-defensin, D-dimer, and interleukin-6 (IL-6) in clinical practice.
Method:
Online databases were systematically searched until June 18th, 2020 with keywords and medical sub-headings terms. Studies mentioned the sensitivity and specificity of biological markers in detecting PJI were included in our study. The sensitivity, specificity, and diagnostic odds ratios (DORs) were obtained after integration.
Results:
A total of 34 studies with 1036 patients diagnosing as PJI were included for comparing α-defensin, D-dimer, and IL-6. The sensitivity and specificity of α-defensin for PJI were 0.88 and 0.96, and the DOR was 189 (95% CI 72–496), respectively. The sensitivity and specificity of D-dimer (0.82 and 0.72) and IL-6 (0.80 and 0.89) were lower than α-defensin.
Conclusion:
The detection of α-defensin is a promising biomarker for diagnosing PJI. The optional cut-off needs to be curtained when using other biomarkers.
Introduction
With the aging of the world population and the improvement of artificial joint replacement technology, more patients with bone and joint diseases have chosen to receive artificial joint replacements in recent years. This surgical method effectively eradicates the patient’s joint pain, restores and improves their joint function, and thereafter improves the quality of life, especially for elderly patients. It has now become one of the most successful surgical procedures recognized in the world. 1,2 However, because the artificial joint prosthesis itself does not have the potential for repair, the prosthesis will inevitably wear out and the joint instability will eventually lead to the erosion of the bone around the prosthesis and cause the prosthesis to loosen with the continuous extension of the use time. However, as researchers continue to study prosthesis loosening after joint replacement, it has been found that periprosthetic joint infection (PJI) is one of the major causes of prosthesis loosening after artificial joint replacement. 3,4 Due to its complexity, PJI is clinically unavoidable and often leads to a poor clinical prognosis. 5 According to previous related literature, it is found that the probability of PJI in patients undergoing artificial shoulder and hip replacement surgery can reach 1%, while in patients received knee artificial joint replacements is close to 2%, while the infection rate of the elbow replacement group is higher, reaching 3%–8%. 6 –8 Patients with joint diseases who suffer PJI after artificial joint replacement not only take a heavy medical burden on their family and society but also are seriously affected in their quality of life. After PJI, reoperation is usually required, and anti-infective treatments such as lavage and debridement therapy may be required during the process, and severe cases may even face amputation. 9
The complications of PJI after joint replacement cause great harm to patients, however, there is still no effective way to avoid such incidents in clinical practice. The main problem at present is the difficulty of diagnosis of PJI. So far, there are no clear diagnostic criteria that can diagnose all chronic PJIs. 10 In particular, chronic PJI caused by some less virulent bacteria is often more difficult to be diagnosed, which affects the choice of treatments. 11
Besides, there is no accurate detection method that can be used as the gold standard in relevant fields. 12 There are still many problems to be solved to effectively diagnose the symptoms of infection around the prosthesis, which is difficult before the revision surgery. 13 In recent related studies, it is speculated that the above results are caused by low-virulence pathogens, and patients who are missed diagnoses usually show more serious clinical results. 14 Since the diagnosis of PJI has been the focus and difficulty of clinical medicine for a long time, it is necessary to find a scientific solution to minimize the incidence of this catastrophic concurrent disease. 13 The hematology tests have the characteristics of convenience, efficiency, and low cost. therefore, they have always been the first choice in the practice to screen patients with chronic PJI. 15 In this systematic review and meta-analysis, we are trying to compare the most useful biomarkers in diagnosing PJI, analyzing the diagnostic accuracy of different biomarkers, and providing a diagnostic suggestion for clinical practice.
Methods
This study was carried out by the preferred reporting items for systematic review and meta-analysis (PRISMA) guidelines. 16
Search strategy
This diagnostic meta-analysis was designed to compare the diagnostic accuracy of different biomarkers in detecting PJI patients. The online databases, including Pubmed, Ovid Medline, Embase, and the Cochrane Library were systematically searched until June 18th, 2020. Also, Google Scholar and other search engines were screened for the gray literature. The keywords and medical sub-headings (MeSH) terms were designed by an experienced librarian. Briefly, the keywords included “biomarker,” “interleukin-6,” “alpha-defensin,” “C reactive protein,” “D-dimer” and “periprosthetic joint infection”. All the studies were downloaded as cite containing titles and abstracts and were imported into Endnote X7 for deleting duplication and literature screening.
Selection criteria
All the studies mentioned the sensitivity and specificity of the biological markers in detecting PJI were included in this systematic review. Specifically, we focused on the diagnostic accuracy of α-defensin, D-dimer, and interleukin-6 (IL-6) in diagnosing PJI in the meta-analysis. The inclusion criteria were as follow: 1) the samples were from blood or synovial fluid, 2) the number of true positives (TP), true negative (TN), false positives (FP), and false negatives (FN) or the sensitivity and specificity could be extracted from the original articles; 3) the studies diagnosed the PJI with common diagnostic criteria. The other meta-analysis, reviews, letter, editorial, and conference abstracts were reading for the further inclusion of the studies.
The exclusion criteria were: 1) the total sample of studies were less than 10; 2) case reports; 3) no data on patients diagnosing as PJI; 4) no assessing of the diagnostic accuracy of α-defensin, D-dimer, and IL-6, and 5) the study was not reported in English.
Literature screening and data extraction
Two researchers (Cui LW and Jiang WH) independently screened the titles and abstracts based on the including and excluding criteria. The full texts were further evaluated if it could not be determined by the titles and abstracts. The superior researcher (Tian BZ) was adapted for discussion if any disagreement existed. After the literature was determined, the data were extracted in a standard excel form including the information as follows: the first author, publish year, publish country, recruitment year, the total included sample, the number of PJI cases, the diagnostic criteria of PJI, the location of study, and cases of infected joint (knee or hip), the diagnostic methods, the cut-off of the detection method, the source of the sample, and the cases of TP, FP, FN, TN or the sensitivity and specificity of the diagnostic methods.
The most common PJI diagnostic criteria were the Musculoskeletal Infection Society (MSIS) criteria. Generally, patients satisfied with one of the following criteria were considered as PJI patients: 1) there is a sinus tract communication with the prosthesis; 2) two positive periprosthetic cultures with phenotypically identical organisms; and (3) three of the following five criteria were positive: (a) increased erythrocyte sedimentation rate (ESR) and C reactive protein (CRP); (b) increased synovial fluid white blood cells; (c) an increased synovial fluid percentage of polymorphonuclear neutrophils; (d) positive histological analysis of periprosthetic tissue; and (e) a single positive culture. 17
Quality evaluation
Two researchers (Cui LW and Tian BZ) independently evaluated the quality of the included studies. The quality evaluation was based on the Quality Assessment for Studies of Diagnostic Accuracy Score (QUADAS) tool, with a maximum score of 14. 18
Statistical analysis
For each study, the sensitivity and specificity were recorded from the original study and calculated based on the TP, FP, FN, and TN. Besides, the positive likelihood ratio (PLR), negative likelihood ratio (NLR), and diagnostic odds ratio (DOR) were obtained after integration. The 95% confidence interval (95% CI) was calculated for each item. The higher the value of DOR, the higher the diagnostic value the biomarker had. The analysis was based on a summary of receiver-operator characteristics (SROC) curves. 19,20 The heterogeneity was assessed using the χ2 test and I2 statistics (I2 ≥ 50% indicating the presence of heterogeneity). The random-effect model and the subgroup analysis were furtherly used for detecting the source of the heterogeneity. To judge the publication bias, the funnel chart (Deek’s funnel plot) was drawn accordingly. All calculations were performed by Stata 15.0 software with the MIDAS module.
Results
Literature screening
A total of 1,518 studies were found based on the search strategy above. 7 other records were identified through other sources. The flowchart of the literature selection was shown in Figure 1. After screening the titles and abstracts, 242 studies were scanned in full text. Unrelated studies were excluded. A total of 52 studies described the biomarkers in diagnosing PJI patients, and among them, 34 studies were included for comparing α-defensin, D-dimer, and IL-6 in PJI. 3 –5,15,17,21 –49

The flowchart of literature screening.
Characteristics of including study
The characteristics of the included studies were shown in Table 1. A total of 3,246 patients were included in our meta-analysis, among them, 1036 patients were diagnosed with PJI, and 2,250 patients were not. Nineteen studies were published after 2017, and the recruitment year was between 2013 and 2019. Ten studies were from Germany, seven studies from the United States, six studies from China, three studies from Austria, two studies from Egypt, and the rest were from Japan, Italy, Belgium, separately. Fifty-one percent of patients had undertaken knee surgery while the rest had undertaken hip surgery. The MSIS criteria were adopted in 23 studies to diagnose the PJI. Thirteen studies used α-defensin, eight studies used D-dimer, and 10 studies used IL-6 to detect PJI. The quality of included studies was assessed in QUADAS guidelines, with high quality, and all the studies were scored ≥13 based on the QUADAS guideline.
The characteristics of included studies.

The diagnostic accuracy of α-defensin, D-dimer, and IL-6 for PJI
The pooled sensitivity and specificity of α-defensin, D-dimer, and IL-6 in PJI were plotted in Figures 2 to 4. In Figure 2, the sensitivity of α-defensin for PJI was 0.88 (95% CI = 0.82–0.93) with I2 = 62.97% which had a median heterogeneity. Similarly, the specificity was 0.96 (95% CI = 0.93–0.98). The DOR of α-defensin was 189 (95% CI 72–496). In Figure 3, the sensitivity of D-dimer for PJI was 0.82 (95% CI = 0.73–0.88) with I2 = 81.68% which had high heterogeneity. Similarly, the specificity was 0.72 (95% CI = 0.59–0.82), also with high heterogeneity (I2 = 83.28%). The DOR of D-dimer was 11 (95% CI 5–26). In terms of IL-6 for PJI, the sensitivity was 0.80 (0.69–0.88), and the specificity was 0.89 (0.79–0.95), also with high heterogeneity. The DOR was 33 (95% CI 13–89). Thus, we used the random-effect model to weight those studies.

The pooled plots of sensitivity and specificity of α-defensin.
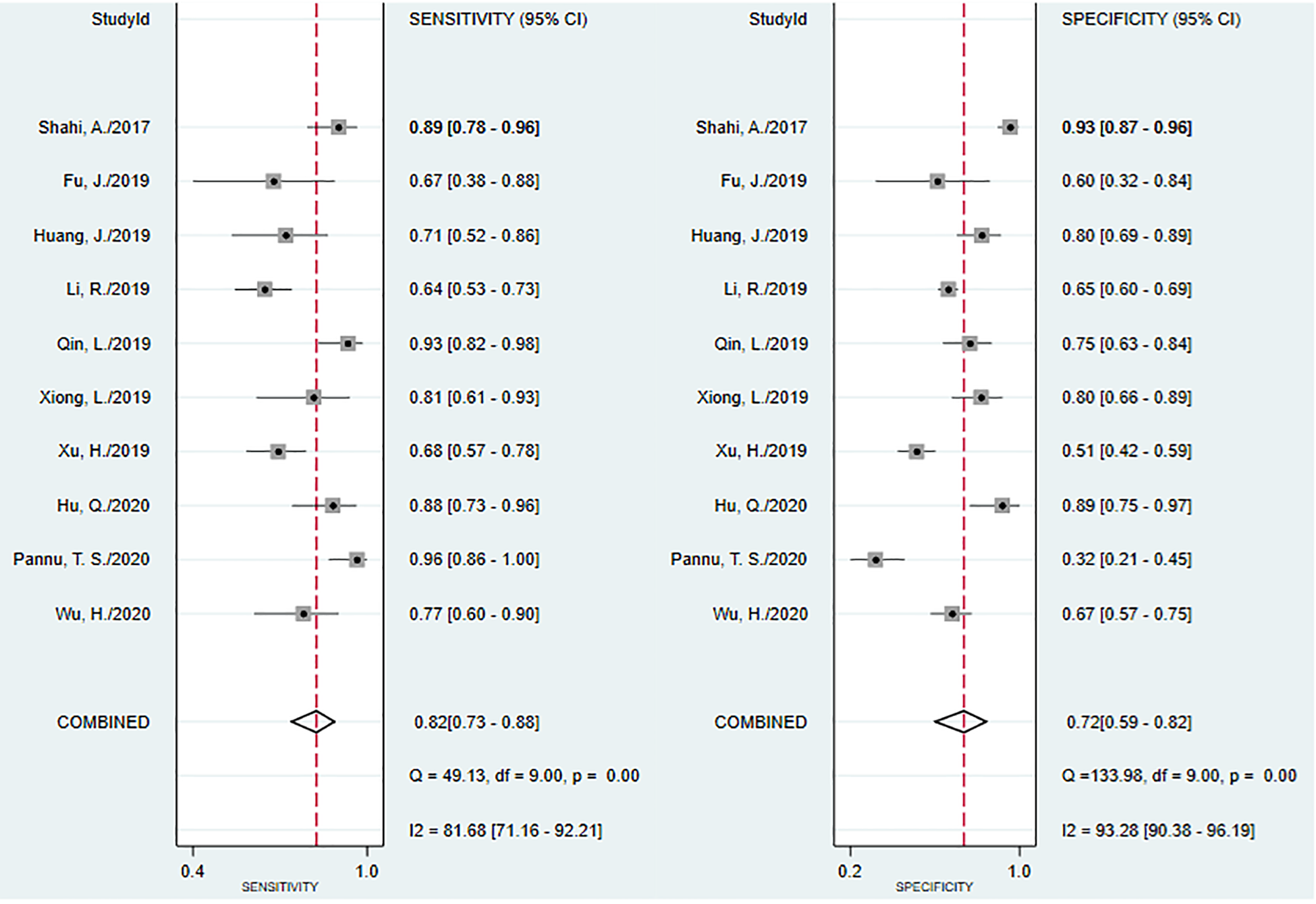
The pooled plots of sensitivity and specificity of D-dimer.
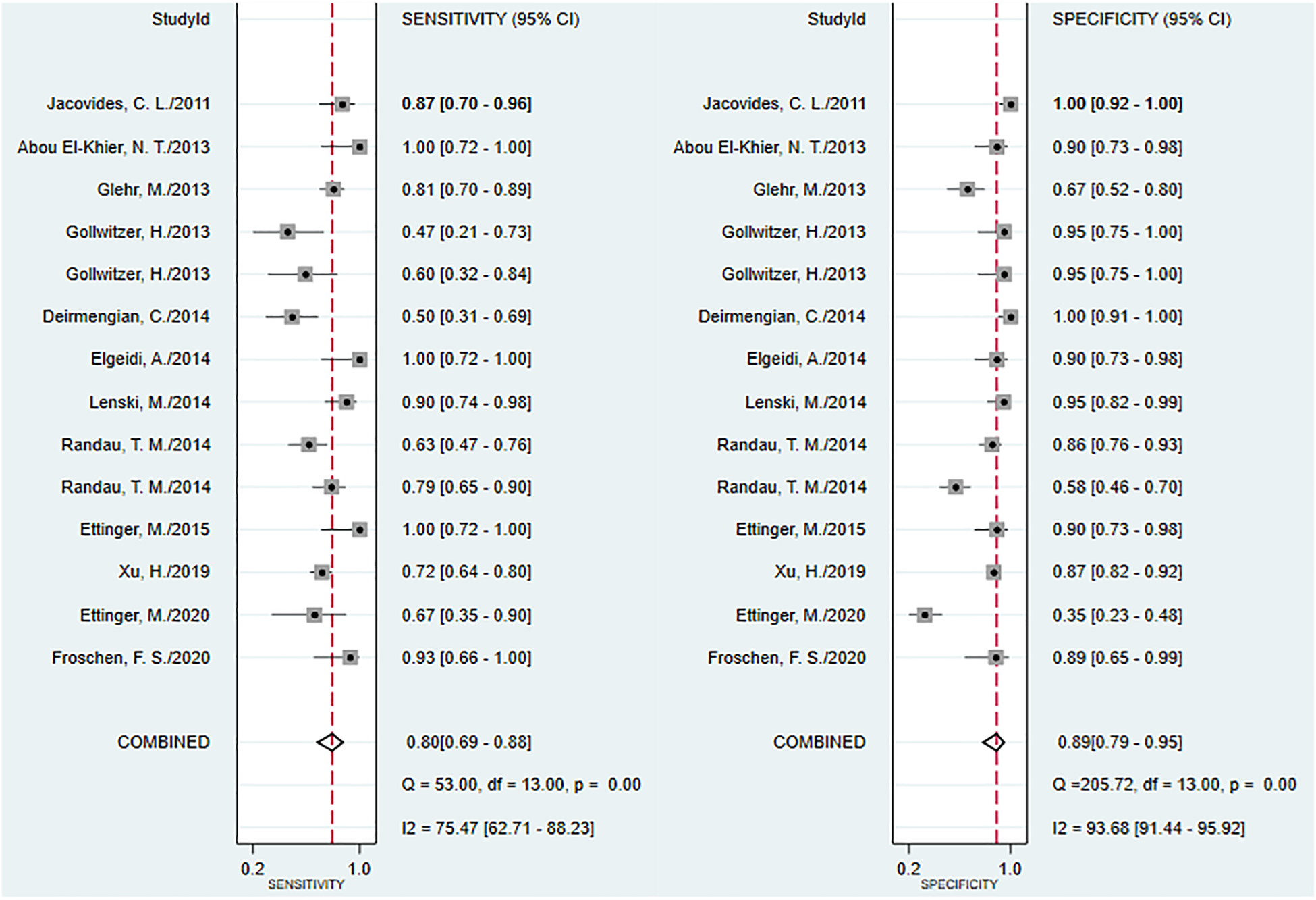
The pooled plots of sensitivity and specificity of IL-6.
The SROC of α-defensin, D-dimer, and IL-6 in detecting PJI were shown in Figure 5. Among the three diagnostic approaches, the α-defensin occupied the largest area of the curve (AUC) with 0.98 (95% CI 0.95–1.00), the area under SROC of IL-6 was 0.91 (95% CI = 0.88–0.93), which was larger than D-dimer (AUC = 0.85, 95% CI = 0.87–0.87). Besides, we assessed the Deek’s funnel plot test to assess the publication bias of the included study, and all the P-value was larger than 0.05, suggesting no evidence of publication bias (Figure 6).

SROC curves of included studies using three different biomarkers.

Publication bias assessment of included studies.
Subgroup analysis in α-defensin, D-dimer, and IL-6 for PJI
To further evaluate the heterogeneity in each approach, we undertook the subgroup analysis to explore the sources of heterogeneity, such as publish year, publish country, the cut-off of different approaches, and the sources of the sample (Table 2). In terms of α-defensin, the sensitivity and specificity were 0.84 and 0.95 for studies from Germany, 0.86 and 0.95 for studies published after 2017, and 0.86 and 0.96 for an approach using Synovasure (Zimmer Inc). All the DOR were larger than 100 for each subgroup.
Subgroup analysis of α-defensin, D-dimer, and IL-6 for PJI diagnosis.
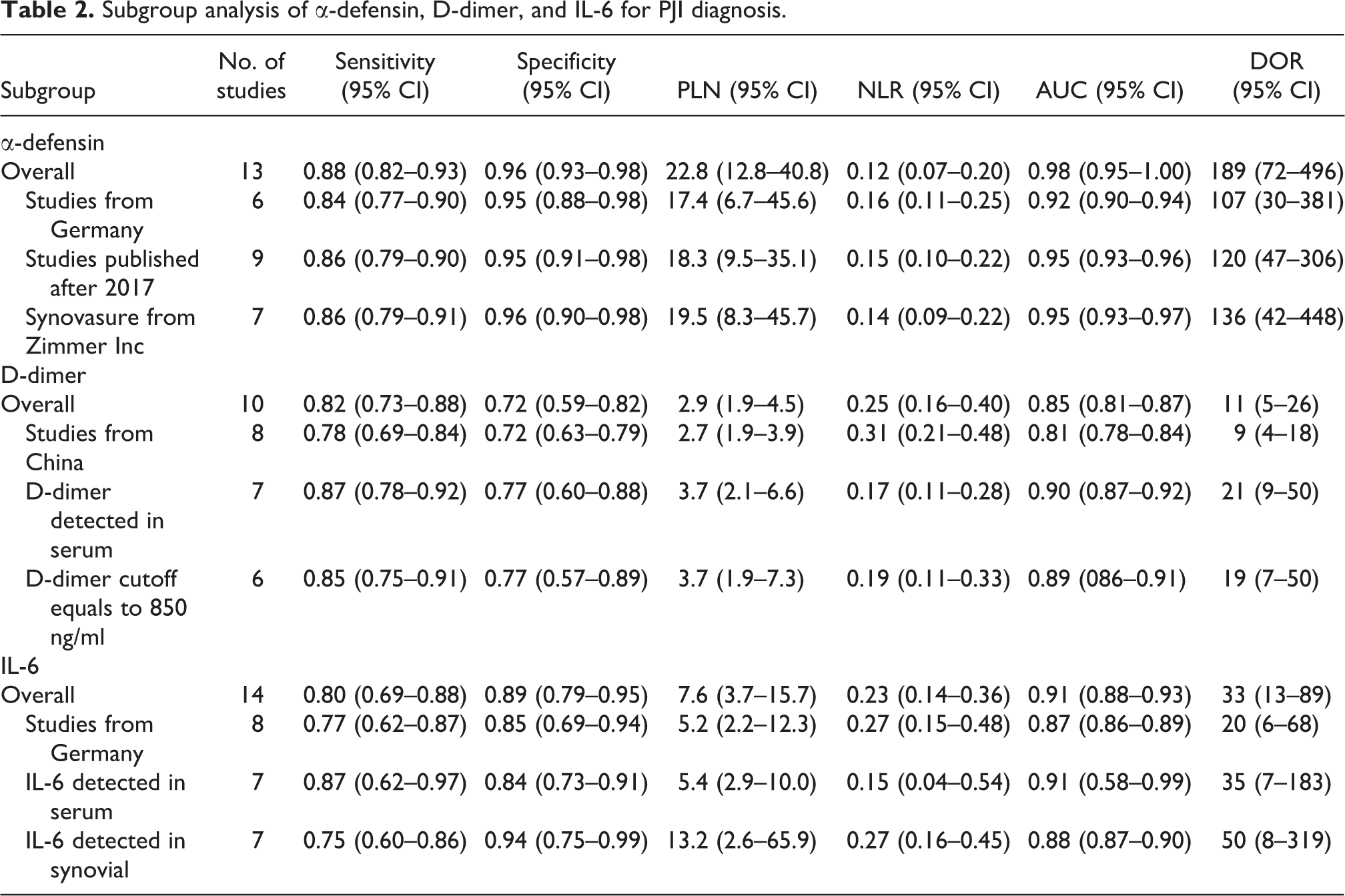
In terms of D-dimer, the sensitivity and specificity were higher in the sample tested in serum than the overall detection, which was 0.87 (95% CI 0.78–0.92) and 0.77 (95% CI 0.60–0.88). In terms of IL-6, although the sensitivity was higher in the sample detected in serum (0.87, 95% CI 0.62–0.97) than the sample detected in the synovial fluid (0.78 95% CI 0.60–0.86), the specificity and DOR of sample detected in the synovial fluid was higher (0.94, 95% CI 0.75–0.99 and DOR = 50, 95% CI = 8–319) comparing to the sample detected in the serum (0.84, 95% CI 0.73–0.91 and DOR = 35, 95% CI = 7–183)
Discussion
Our systematic review and meta-analysis reviewed 52 studies and included 34 studies for comparing α-defensin, D-dimer, and IL-6 in the diagnosis of PJI. Our study suggested that α-defensin could provide higher diagnostic accuracy than D-dimer and IL-6. In terms of D-dimer and IL-6, the diagnostic accuracy was higher if the sample was achieved in synovial fluid rather than serum but the cut-off of each index needed to be investigated.
The diagnosis of PJI is complicated and difficult because of its lack of specific clinical manifestations and symptoms, and lack of laboratory tests with high sensitivity and specificity that can be clinically accepted. 50 MSIS has proposed the diagnostic criteria for prosthetic infections but also has major problems in clinical practice: 1) there are subjective criteria in the diagnostic criteria, such as observing pulse formation or pathological examination of frozen sections; 2) multiple indicators need a culture of organisms in the diagnostic criteria, which will cause the delay in diagnosis; 3) The diagnostic criteria involve primary and secondary criteria, which are complicated to apply. 51 Due to the various deficiencies of the diagnostic criteria, the diagnosis of PJI urgently needs a laboratory test with good specificity and sensitivity to guide the clinical diagnosis. Serological examination occupies an important position in the diagnosis of various diseases due to its ease of operation. However, serological indicators are often related to a variety of diseases, and therefore often have the disadvantage of poor specificity. However, according to the American Association of Orthopaedic Surgeons (AAOS) clinical practice guidelines, serological indicators are important indicators for diagnosing infections around the prosthesis. 52 The guidelines believe that all patients with suspected prosthetic infections should be tested for CRP and ESR. And it is recommended that ESR exceeding 30mm/h or CRP exceeding 10mg/L can be considered as possible periprosthetic infection. However, CRP and ESR are not very specific indicators. According to reports, the specificity of CRP is 87%, and the specificity of ESR is only 67%. 53 Serum IL-6 was adopted for diagnosing PJI since 2005. 53,54 IL-6 is a member of the cytokine family and it is a protein composed of 184 amino acids formed by phosphorylation and glycosylation of alpha-helix structure protein. It plays an important role in inflammation, bone metabolism, and tumorigenesis. 55 In our study, we evaluated that the specificity and DOR of synovial IL-6 were higher compared to serum, which indicated that the synovial fluid had a higher diagnostic accuracy than serum because it is only focused on the location of the infection.
D-dimer is a biomarker associated with sepsis, systemic, and abdominal inflammation. As a specific product representing secondary hyperfibrinolysis in vivo, D-dimer has been widely used in the exclusion diagnosis of venous thrombosis of the lower extremities. 56 In the past, Ribera et al. 52 reported that septic arthritis caused the increase of D-dimer in the synovial fluid due to the inflammation caused by bacteria in the joint. In recent years, many studies have confirmed that D-dimer in the blood can be used as a diagnostic tool for PJI. 4,22,28,35 Eight studies analyzed the effect of D-dimer in evaluating the diagnostic accuracy in PJI. However, the DOR of D-dimer was not so high comparing to IL-6, this may be because there was not a standard cut-off to diagnose the PJI patients.
Alpha-defensin is a bacteriostatic peptide that is secreted by white blood cells into the synovial fluid after pathogen infection and then integrated into the pathogen cell membrane to quickly kill the pathogen, thereby providing antibacterial support to the immune system and completing spontaneous and adaptive immune responses. 57 Bingham et al. found that the α-defensin immune response has a higher diagnostic accuracy for periprosthetic infections, and provides the same accurate diagnostic information as the MSIS diagnostic guidelines in all researched patients. 45 The synovasure test is an immunoassay test that measures the concentration of α-defensin peptides in human synovial fluid. In our meta-analysis, the α-defensin test would provide the highest sensitivity and specificity in diagnosing PJI with satisfied DOR.
α-Defensin, D-dimer, and IL-6
There were still some limitations to our study. Firstly, there were still heterogeneities existing among studies although we had undertaken the subgroup analysis, further meta-regression analysis was needed to undertake for seeking for the source of the heterogeneity. Secondly, most studies used the MSIS to define PJI, but still, several patients missed the diagnosis because the gold standard cannot be detected. Thirdly, although we mentioned that the best cut-off was needed to evaluate in IL-6 and D-dimer, it is still impossible to calculate the optimal cut-off value in our meta-analysis due to the lack of individual patient data.
Conclusion
Detection of α-defensin could provide higher sensitivity and specificity in diagnosing hip and knee PJI, with a satisfied diagnostic accuracy comparing to IL-6 and D-dimer. The synovial fluid sample would be a better choice compared to serum to detect the biomarker while the best cut-off still needed to be investigated.
Footnotes
Author contributions
Design of the meta-analysis: Baozhong Tian. Literature screening: Liwen Cui and Weihai Jiang. Quality assessment: Baozhong Tian and Liwen Cui. Statistics analysis: Baozhong Tian. Write and revise: Baozhong Tian, Liwen Cui, and Weihai Jiang.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.