
Abstract
Current literature occasionally considers septic arthritis in native joints and prosthetic joint infections as equal pathologies. However, significant differences can be identified. The aim of this review of literature is to describe these differences in definitions, pathology, diagnostic workups, treatment strategies, and prognosis.
Background
It can be challenging to establish the diagnosis of septic arthritis (SA) in native joints or periprosthetic joint infections (PJIs). 1,2 Delayed or inadequate treatment can result in life-threatening septicemia 1,3 –6 as well as loss of joint function and quality of life. 3 –7
Although there are similarities between SA and PJIs, there are also important differences that subsequently lead to different treatment modalities for both pathologies. 3,8 –13 Occasionally, there are still studies that appear to consider, evaluate, and treat SA and PJIs as equal pathologies, 14 –16 which is incorrect and could possibly have harmful repercussions. 17,18 Therefore, the aims of this review are to describe both the similarities and the differences between SA and PJI and to elaborate on the clinical implications of these differences.
Incidence and definitions
SA is a serious infection of the joint. 1,3 The incidence of SA varies from 6 to 10 cases per 100,000 individuals per year. 19,20 SA is generally monoarticular but can also occur polyarticular. 1 The knee is affected more often compared to other joints. 19,21 Peak incidences are in children under 3 years and adults over 55 years of age. 19,20 Polyarticular disease occurs in approximately 10–20% of the patients. 1
PJIs are one of the most serious complications in total joint arthroplasties and are an increasing problem. 5,22 –24 The incidence of PJIs is rising and currently varies from 1% to 3% for primary hip and knee arthroplasties 25 –28 and up to 5.6% in revision cases. 5,25,26 The majority of patients with PJIs are over 65 years old. 19,24 Although bilateral PJIs have been described in case reports, the incidence of polyarticular PJIs is unknown. 29,30
Underlying joint diseases, such as rheumatoid arthritis and other forms of inflammatory arthropathies, are predisposing factors for developing both SA and PJIs. 1,4,28,31,32 Patients receiving immunosuppressive therapy, such as classic disease modifying antirheumatic drugs, anti-Tumor-Necrosis-Factor (TNF) therapy, or intra-articular corticosteroid injections, are also at higher risk of both SA and PJI. 1,31,32 Other risk factors are alcoholic and intravenous drug abuse, cutaneous ulcers, and diseases such as diabetes, leukemia, cirrhosis, granulomatous diseases, cancer, and hypogammaglobulinemia. 1,4,31 –33 Additional risk factors for PJIs are obesity, malnutrition, and smoking. 6,26,28,31,33 These factors have not been assessed for patients with SA but are likely to be risk factors for SA as well.
The definition of having either SA or PJI is linked to diagnostic criteria. Considering the similarities in diagnostic workup possibilities for both joint conditions, large differences between described criteria can be found (Table 1).
Criteria for the diagnosis PJIs and native SA.

CRP: C-reactive protein; ESR: erythrocyte sedimentation rate; PMN: polymorphonuclear; WBC: white blood cell; SA: septic arthritis; PJI: periprosthetic joint infection.
aFor a positive diagnosis: 1 major criterion or scoring minor criteria.
bFor a positive diagnosis: 1 criterion.
In 1976, Newman 34 defined that in adults, SA is present if one of the four criteria in a patient with an inflammatory joint is found (Table 1). Four decades later, those criteria are still being used. 32,35,36 A major issue is that SA can be present without meeting the criteria, as described by Newman et al. 3,13,34,35,37 Even with additional available tests, diagnosis can still be delayed or missed. 13,36 Furthermore, SA is always an acute medical emergency, but if it remains untreated for a long time and the patient survives the infection, it becomes a chronic infection. 38 The definition of “chronic” remains unclear within current literature. Cases of chronic SA are rare and seem related to microorganisms causing subacute infections like Mycobacteria, Borrelia burgdorferi, and fungus. 38 –43
An updated definition, with clear criteria for SA, was not found within recent literature and might be a valuable addition to current daily practice.
The definition of PJIs dates from recent International Consensus Meeting documents. 2 A PJI is present with either one major criterion or by scoring the presence of minor criteria, as presented in Table 1. Similar to SA, PJIs can be missed despite the available tests and the updated definition, particularly in cases with less virulent organisms. 2 PJIs can be divided into acute and chronic PJIs. 11,44 Acute PJIs are early postoperative surgical site infections or acute hematogenous PJIs. 44 Acute hematogenous PJIs occur with a sudden onset of inflammatory joint pain in a previously symptom-free prosthetic joint as a result of bacteremia. 5,27,28,44,45 Acute PJIs can become chronic. Dividing SA into acute and chronic depends on the time frame in the existence of the infection. In PJIs, this is based on biofilm formation.
Pathology
The synovial membrane in joints is a well-vascularized structure with no limiting basement plate. 12,13 The lack of a natural barrier allows easy access for bacteria. 12,13 Once bacteria reach the joint space, the low fluid shear conditions allow bacteria to settle and to cause an infection. In addition, matrix proteins produced by the host may promote progression of the infection. 46 Colonization of the synovial fluid occurs and bacteria rapidly proliferate, generating an acute inflammatory response. 47 The host starts producing inflammatory cytokines, such as interleukin 1b (IL-1b) and IL-6, which promote opsonization and activation of the complement system. 47 When the host is immunocompetent, a protective inflammatory response is invoked and pathogens are eliminated by macrophages, synoviocytes, and polymorphonuclear (PMN) cells. If the immune system fails, SA has occurred. If SA is not ceased, progression of the infection generates joint effusion that increases intra-articular pressure, which prevents nutrients from reaching and supplying the joint. 1,13,46 This may result in the destruction of the synovium and cartilage. 1 In PJIs, the original joint surfaces have been replaced but soft tissue and bone damage occurs. 48 In both SA and PJIs, the most common microorganism is Staphylococcus aureus. 1,48 The second common microorganism is Staphylococcus epidermidis in PJIs and Streptococci in SA. 1,48
An important aspect of PJIs and a considerable difference with SA is biofilm formation. This process starts after bacteria and/or fungal penetrate the synovial membrane and attach to the prosthetic material. 49,50 A biofilm is a biologically active matrix of cells and extracellular substances. 48,51 These substances are released by bacterial or fungal cells and consist of extracellular polysaccharides that form an insoluble and slimy secretion on the prosthetic surface. 48,51 This slimy layer encapsulates the involved microorganisms and offers them three important advantages. First, due to the composition of charged polysaccharide groups, the layer can bind vital nutrients that are required for bacterial metabolism. Secondly, the layer can assist in dissemination of nutrients that are necessary for the growth of the invasive cells. Third, cells that are encapsulated are well protected from their external environments like host immune systems and antibiotics. 48,51 The process of biofilm formation starts within seconds after contamination. Time to maturation depends on several factors such as microorganism species and localhost and environmental factors. 49,50 During the early stages of formation, biofilms can be less stable and are therefore more susceptible to antibiotics and host defenses. 27,50 Until a mature biofilm has been formed, a PJI can be categorized as an acute PJI. 44 PJIs with mature biofilms, the chronic PJIs, are difficult to treat. 10,44,50,51
Diagnosis and workup
Patients representing with a short history of a hot, swollen, and tender joint, with restriction of movement and/or the inability to bear weight should be suspected of SA or an acute (hematogenous) PJI. 2,3,5,28,44
Laboratory tests may demonstrate elevated C-reactive protein (CRP), serum leukocyte cell count, and erythrocyte sedimentation rate (ESR). 2,3,11 Blood cultures were taken and synovial fluid was tested for bacteria, white blood cell (WBC) count, and percentage of PMN leukocytes. 2,3,11 Threshold values to support the diagnosis of infection are presented in Tables 1 and 2. 2,3,13,18,52,53 However, values for SA are still under debate. 3,13,18,45,52,53 Baran et al. 53 and Carpenter et al. 18 demonstrated that elevated WBC and PMN levels are highly associated with SA. Synovial fluid analyses are not included in the definition for SA, as opposed to PJI, but they could be a valuable addition. 18,45,53,54 Radiographs should be analyzed for periosteal reaction, osteolysis, and bony resorption without implant wear or the absence of it can have clinical consequences for the diagnostic pathways and treatment. 3,55
Important differences between native SA and PJIs.
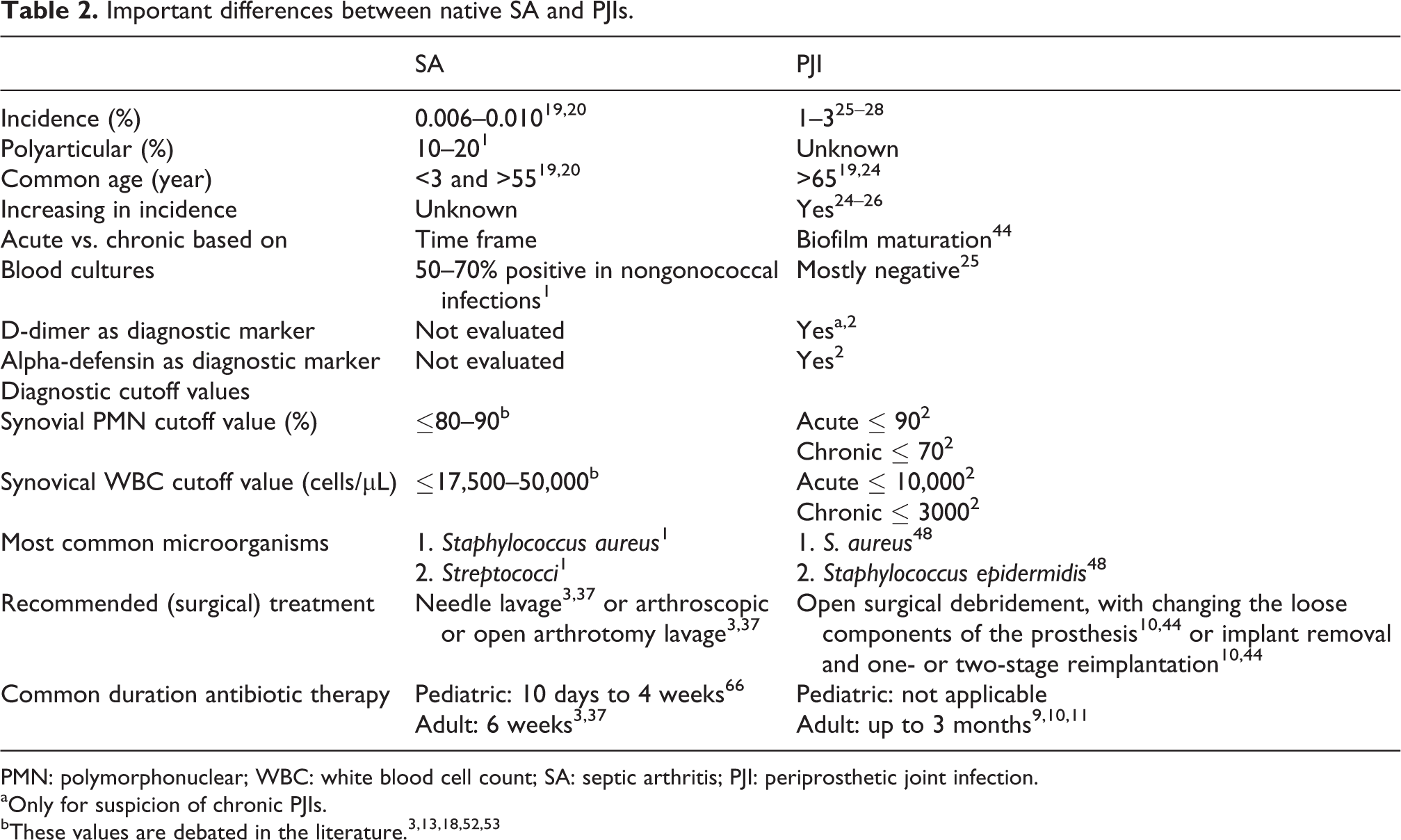
PMN: polymorphonuclear; WBC: white blood cell count; SA: septic arthritis; PJI: periprosthetic joint infection.
aOnly for suspicion of chronic PJIs.
For other ways of radiographic imaging, there might be a small role in both pathologies, however for PJIs, this is highly debated. 1,3,22,37,45 Ultrasound can be used to identify the presence of significant local joint effusion and ultrasound-guided aspiration. 3,22 CT scans and MRIs are not the optimal diagnostic tool for patients with joint prosthesis. The presence of metallic implants causes beam hardening and dephasing artifacts. However, CT and MRI could be useful in detecting soft tissue abnormalities, such as joint effusion, sinus tracts, soft tissue abscesses, and bone erosions. 22 For SA, these principles can be considered the same way, and CT scans and MRIs could be used to evaluate soft tissue involvement as well as bone erosions and osteomyelitis. 1,3,37
Early postoperative PJIs often, but not always, present with local signs of cellulitis, erythema, swelling, pain, wound discharge/drainage, and delayed wound healing. 3,11,44 Systemic symptoms such as fever and chills may also be present. 11
Chronic PJIs typically present with slowly increasing pain and deterioration of joint function without systemic symptoms. 11 Although any painful prosthesis may represent a PJI, the absence of an obvious mechanical reason for a painful prosthesis in the first few years following implantation, a history of wound healing problems, or superficial or deep infection should also raise the suspicion of PJI. 11
Repeated joint aspiration or intra-articular biopsies may be required when clinical suspicion for PJIs is high in the absence of major criteria. 2,45,56 For intra-articular biopsies, it is recommended to collect three to six periprosthetic tissue samples. 45 To optimize the identification of microorganism following the removal of prosthesis, sonication could be used. 57 Sonication is the use of low-intensity ultrasound for the disintegration of biofilm on removed implants, and it has been shown to possibly increase the chance of identifying causative microorganisms in the obtained cultures. 58 –60 However, currently, there is insufficient data to support the routine use of sonication and future studies for this method are recommended. 57
In the light of the aforementioned similarities of available clinical diagnostics, it is remarkable to establish that currently positive synovial cultures and purulence are the only common criteria for both types of infection. In former consensus documents about PJIs, purulence was deleted from the definition, but the new consensus has adopted it as a minor criterium again. 2,33,45 An objective definition for purulence is still absent and, therefore, the subjective nature of the assessment seems prone for interobserver unreliability. 2,33,45 Besides, purulence can also be found in noninfected native and prosthetic joints. 45 For firm conclusions about purulence as a diagnostic tool and criterion in SA and PJIs, clinical research is recommended.
An important difference to discuss is the use of CRP and ESR as definition criteria. For PJIs, elevated CRP and ESR are minor criteria. 2 Although they are not used as criteria for SA, CRP and ESR are easily obtained and are a valuable addition to the diagnostic workup for SA. 3,45
Furthermore, several synovial biomarkers other than WBC and PMN can be found within the minor criteria for PJIs. 2 Despite limited evidence, D-dimer has gained a place in the minor criteria for the definition of chronic PJIs. 2 For SA, no literature was found about using D-dimer as a possible marker. Based on the lack of evidence for this marker in PJIs and in perspective of other available tests, it does not seem advisable to evaluate this marker for diagnosing SA.
Leukocyte esterase and the alpha-defensin test are both biomarkers from synovial fluid that are determined to be a valuable addition in diagnosing and defining PJIs. 2 No studies were found evaluating alpha-defensin as a biomarker for SA, but it might be interesting to evaluate this. For the leukocyte esterase (graded as negative, trace, +, ++, or +++) as a biomarker for SA, two studies were found. 61,62 One found a sensitivity of 100%, a specificity of 88.24%, a positive predictive value 68.42%, and a negative predictive value of 100% with a threshold of ++. 61 The study of Gautam et al. found a sensitivity of 79.2%, specificity of 80.8%, a positive predictive value of 61.8%, and a negative predictive value of 90.1% also with a threshold of ++. 62 They concluded that this test could efficiently differentiate other etiologies of inflammatory arthritis from SA. 62 Leukocyte esterase seems a useful biomarker and could possibly be used for diagnosing and defining SA.
Another difference between both workups is the role of blood cultures; in SA, they are part of the definition and in PJIs not. 2,34 Blood cultures are reported to be positive in 50–70% of patients with nongonococcal cultures in native SA. 1 Blood cultures are a sensitive method for detecting bacteremia. 63 They are used in all kinds of infections, but they are not a specific marker for one type of infection. 63 Also half of these cultures are contaminants. 64,65 Taking this into account, it could be reassessed whether blood cultures should be a criterion in the definition for SA. Blood cultures in PJIs are mostly negative. 25 Therefore, blood cultures in PJIs can be considered for patients with systemic manifestations but are not included in a standard diagnostic workup. 11
Treatment
If clinical suspicion of SA is high, immediate joint irrigation is recommended, preferably after taking cultures. 3 Arthroscopic or open lavage has yet to be proved as superior to less invasive treatments such as needle lavage. 3,37 Therefore, one could argue to start with the least invasive procedure, a needle aspiration and irrigation. If unsuccessful, an arthroscopic lavage should be performed. 3 In adults with native SA, antibiotic treatment typically consists of 2 weeks intravenous therapy, followed by 4 weeks oral treatment. Treatment regimen can be adjusted on behalf of clinical symptoms. 3,37 Antibiotic treatment in pediatric joint infections has a duration of 10 days to 4 weeks. 66 In rare cases of septicemia that cannot be controlled with regular treatment options, amputation could be performed.
Acute and chronic types of PJIs are managed differently due to the aforementioned biofilm formation. In acute PJIs, the standard procedure is open surgical debridement, with changing the loose components of the prosthesis, followed by antibiotics and implant retention (DAIR). 10,44 Due to biofilm maturation, DAIR later than 4 weeks from the initial arthroplasty and/or duration of symptoms of infection is more likely to fail. 44 Arthroscopic debridement has been shown to be insufficient in treating PJIs. 67,68 Chronic PJIs are treated with the removal of the prosthesis, debridement, and reimplantation, which can be performed in either a one-stage or two-stage procedure. 10,11 Traditionally, antibiotics are administered for a minimum of 3 months in both acute and chronic PJIs. However, the optimal duration of antibiotic treatment is still under debate. 9,11,49,69 Preferably, antibiotics have bactericidal activity against growing organisms in biofilms and should achieve high concentrations in the bone. 9,11 This might lead to a different choice of antibiotics in PJIs compared to SA. For example, rifampicin is often used in combination with fluoroquinolone or amoxicillin in cases of sensitive Staphylococci. 9 Rifampicin allows better penetration of antibiotics through biofilms. 9 For intractable PJIs, arthrodesis, suppressive antibiotic therapy, supervised neglect, or amputation may be indicated. 70,71
Prognosis
Even with correct management of SA, a significant number of cases result in irreversible joint damage and in some patients, in overwhelming septicemia. 4 The risk of permanent loss of joint function is nearly 40%. 1 The recurrence rate of SA in native joints was not found within the literature. The mortality rate of septicemia in SA is approximately 11%, 32 and patients with polyarticular infections have an even higher mortality rate (up to 30%). 1
The prognosis of both SA and acute PJIs is optimized by fast diagnosis and appropriate treatment. 22,44 In chronic PJIs, the time until the start of treatment seems less important. 22,44 Overall, acute postoperative PJIs have a better prognosis than hematogenous PJIs. 23,72 Two-year infection recurrence rates after one-stage and two-stage revision surgery are 7.6% and 8.8%, respectively. 23 Mortality rates in PJIs range from 2.7% to 18%. 6 The large range is due to variation in the study populations from which the data were collected. 6 It is known, however, that prognosis for both SA and PJIs is influenced by the presence of comorbidities, accuracy of treatment, and causative microorganisms. 1,11,22
Discussion
Within their definitions and diagnostic possibilities, there are similarities between SA and PJIs. However, these similarities are not expressed in their current definition criteria. The SA criteria seem dated. It could be recommended to form an updated definition with clear criteria for native SA in the near future. Some diagnostic criteria used for defining PJIs, such as synovial biomarkers, serum CRP, and ESR, might be a valuable addition for the definition of SA. As purulence and blood cultures criteria for both pathologies, it can be recommended to clarify their reliability to determine whether they should earn a place within diagnostic pathways and definitions of both pathologies.
There are clinically relevant differences between SA and PJIs in incidence, common age, causative microorganisms, and treatment. A clear overview of differences is provided in Table 2. The most important and clinically relevant difference is biofilm formation, which is only present in PJIs. Biofilm formation is the main reason why PJIs require an aggressive surgical debridement and/or removal of the prosthesis in combination with a prolonged antibiotic management compared to SA to achieve optimal outcome. 10,22,44,48,50,51 Also, the choice of antibiotics differs between SA and PJIs, 3,9,11,37,66 and their prognosis in clinical outcome is different. 1,4,22,23,72
Conclusion
There are similarities between SA and PJIs, but there also are important clinical and prognostic differences. Because of the differences, considering SA and PJIs as similar infectious pathologies and, therefore, combining their data in clinical research, could lead to wrong clinical decisions, misleading studies and guidelines. Eventually, this might lead to incorrect medical practice with possibly devastating consequences for many patients. This should be considered in future clinical and epidemiological studies and subsequent reports.
Footnotes
Acknowledgements
We would like to thank Dr Dagan Cloutier for editing this article as a native speaker.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.