
Abstract
Purpose:
Sacropelvic fixation continues to present challenges when involved in the adult spinal deformity correction. The S2 alar iliac (S2AI) fixation is commonly used in sacropelvic fixation. Several techniques, including intraoperative navigation and freehand technique, were used for S2AI screws placement. The aim of this study is to analyze the anatomic parameters for S2AI screw trajectory in Asian population and introduce a novel technique described as a three-dimensional printed template guided technique (TGT). Meanwhile, the accuracy and safety of this technique were compared with the conventional freehand technique.
Methods:
The S2AI trajectory parameters were measured in 100 Asian adult volunteers. Parameters were compared between different genders. Forty-eight adult patients who underwent S2AI screw placement were reviewed: 28 patients received freehand technique and 20 patients received TGT technique. Postoperative computed tomography was used to assess the accuracy of screw trajectory and cortex violation-related complications were recorded.
Results:
The cephalocaudal angles (CAs), maximal length of screw pathway, narrowest width of pathway within the iliar teardrop, distance from the center of teardrop to sciatic notch, and distance of the start point distal to S1 dorsal foramen showed significant gender-related difference (p < 0.05). All 48 patients were placed S2AI screws bilaterally (40 screws in TGT vs. 56 screws in freehand). One screw penetrated iliac cortex in the TGT group but 10 screws penetrated iliac cortex in the freehand group (3% vs. 17.9%) (p < 0.05).
Conclusion:
Approximately 30–35° of CA and 39° mediolateral angle are appropriate for S2AI screw placement in Asian patients. Either freehand or TGT technique is safe for S2AI screw placement. TGT technique is more accurate compared with the conventional freehand technique.
Trial registration:
This is a retrospective study.
Keywords
Purpose
Spinopelvic fixation plays an integral role in achieving solid osseous fusion across the lumbosacral junction, especially in deformity procedures requiring substantial correction or long-segment constructs. 1,2 There are several techniques for spinopelvic fixation that include Galveston technique, 3 iliac screws (iliac bolts), iliosacral screws, and S2 alar iliac (S2AI) screw technique. 1,4 Compared with other pelvic fixation techniques, S2AI screws have been developed to be a prevailing alternative spinopelvic fixation technique due to the advantages of keeping screw tail away from the skin, no incision overexposure, more excellent pullout strength, and standing on the same longitudinal line of lumbar pedicle screws. 5,6 However, S2AI technique is still challenging for less experienced spine surgeons who have no navigation system available.
Inadequate accuracy of screw implantation is potential to result in surgery-related complications. 7 The incidental cortical breach of an S2AI screw may not only result in decreased fixation strength but also injury to the major vessels, particularly the internal iliac artery and the superior gluteal artery when breaching anteriorly and caudally. Injuries of these major vessels could lead to major intrapelvic hemorrhage, which is a life-threatening complication. 8 Therefore, surgeons should avoid anterior or caudal deviation during screw insertion to achieve safe insertion of S2AI screws. At present, the anatomic parameters in American population have been previously analyzed 9 but in Asian population remains unclear.
The aim of this study is to analyze the anatomic parameters for S2AI screw placement in Asian population and introduce a novel technique that depends on these parameters described as a three-dimensional printed template guided technique (TGT). The accuracy and safety of this technique compared with the conventional freehand technique were also evaluated.
Methods
From October 2014 to March 2015, 100 Chinese adult volunteers were recruited to measure the S2AI trajectory. They were 56 males and 44 females with a mean age of 51.6 ± 7.1 years old. We defined the optimal trajectory of the screw to be determined by the line connected the start point and the center of cross section of teardrop above sciatic notch. The start point was located lateral to the midpoint between S1 and S2 dorsal foramina and standing on the extending line from L5 and S1 pedicle screw anchor points. Then, we used UG software (Siemens PLM Software Corp., Plano, Texas, USA) (UG software is one of the most widely used CAD/CAM software in the field of computer aided design and manufacturing. UG software provides process design, parameter setting, simulation machining, entity processing, etc., and real objects of the mold are finally manufactured.) to mimic the optimal trajectory and measured the following parameters described as following (Figure 1). All the parameters were compared between different genders. Cephalocaudal angle (CA), defined as caudal trajectory angulation in the sagittal plane. Mediolateral angle (MA), defined as lateral trajectory angulation in the transverse plane. Maximal length of screw pathway (ML), defined as maximal length of the screw trajectory in pelvis. Narrowest width of screw pathway (NW), defined as the narrowest canal width along the pathway. Distance from the center of cross section of teardrop above sciatic notch to sciatic notch (sciatic notch distance (SD)). Distance of the start point to midline (midline distance (MD)), defined as the distance of the start point away from the midline. Distance of the start point inferior to S1 dorsal foramen (dorsal foramen distance (DD)).

Parameters for S2AI screws placement. Posterior view of 3D CT image. (a) The start point of S2AI was located lateral to the midpoint between S1 and S2 dorsal foramina and standing on the extending line from L5 and S1 pedicle screw anchor points. MD is defined as the distance of the start point away from the midline and DD is defined as the distance of the start point inferior to S1 dorsal foramen. (b) The CA is shown and (c) the MA, ML, and NW are shown. CT: computed tomography; S2AI: S2 alar iliac; MD: midline distance; MA: mediolateral angle; ML: maximal length of screw pathway; NW: narrowest width of screw pathway; DD: dorsal foramen distance.
Meanwhile, from April 2015 to October 2017, 48 patients with degenerative scoliosis, lumbosacral chronic infection, or tuberculosis, who underwent posterior lumbopelvic reconstruction with S2AI screw technique, were retrospectively reviewed. They were 26 males and 22 females with an average age of 58.3 ± 10.5 years old. Among these 48 patients, 28 patients received freehand technique and 20 patients received TGT technique for S2AI screw placement. All the operations were finished by a senior surgeon in our hospital. All the patients received pre- and postoperative pelvis computed tomography (CT).
Three-dimensional printed template preparation
All the patients underwent fine-cut (width of 1 mm) CT preoperatively. Digital imaging and communications in medicine data of CT were collected for each patient from the radiology department. These data were transferred to a 3D printing company and subsequently converted into a digital 3D model in the stereolithography format using Mimics software version 20 (Materialise, Leuven, Belgium). The 3D models and guides were designed with Meshmixer (Autodesk, San Rafael, California, USA) and 3-Matic software (Materialise). The models and guides were manufactured with the FDM 3D printer Fortus 450mc (Stratasys, Michigan, Eden Prairie, Minnesota, USA) using the thermoplastic material. A patient-specific template was obtained.
Surgical procedure
Screw placement began with meticulous subperiosteal dissection of the posterior elements and exposed anatomic landmarks including the S2AI start point. In the freehand group, the start point was located lateral to the midpoint between S1 and S2 dorsal foramina and standing on the extending line from L5 and S1 pedicle screw anchor points, and the following procedures were described by Kebaish and Sponseller previously. 9 –11 In the TGT group, the parameters of the optimal trajectory mentioned above were analyzed by the postprocessing software and the individualized 3D template was designed and printed (Figure 2). In the surgical procedure, the start point is as same as the abovementioned. All soft tissues were thoroughly dissected, dorsal foramen of S1 and S2 was clearly exposed, and the printed 3D guide template was closely matched to the sacral dorsal bone surface. It is crucial to closely match the guide template with the bone surface, which could guide the 2.5-mm K-wire to be drilled forward along the optimal trajectory. Otherwise, the TGT technique should be given up if the template could not closely match the bone surface. After checking the position of the K-wire, the track along K-wire was tapped, then K-wire was removed, and the screw along the track was placed (Figure 3).

A 3D view of the optimal trajectory and printed template. (a) The optimal S2AI trajectory from axial view is shown. (b) The S2AI trajectory from posteroanterior view and the designed template is shown. (c) A virtual printed template is shown. S2AI: S2 alar iliac.

Intraoperative procedures. (a) A template was closely matched with the bone surface after all soft tissues were thoroughly dissected and dorsal foramen of S1 and S2 was clearly exposed. (b) A K-wire (2.0 mm) was drilled along the guided template across the sacroiliar joint and into the ilium.
Postoperative accuracy evaluation of screw placement
Fine-cut (width of 1 mm) CT is used to assess the accuracy of screw placement after surgery. We define that the screw contained between the lateral and medial iliac cortex as being accurately placed. By contrast, screw that violated or broke medial or lateral cortex or the sciatic notch was defined as being inaccurately placed. The screw breach was divided into four grades according to the previous description by Oh et al. 12 No screw breach was defined as grade 0. The screw breach distance away from the cortex less than 3 mm was defined as grade 1 (mild), 3–6 mm as grade 2 (moderate), and more than 6 mm as grade 3 (severe). The screws breaches are considered as unqualified screw placement. All measurements were assessed bilaterally.
Statistical analysis
Data are presented as the mean ± standard deviation. For the optimal trajectory, the independent sample t-test was performed to detect possible divergence of the parameters between genders. And the χ 2 test was used to determine the different results in comparison between freehand with the TGT technique. Statistical significance was defined as p value <0.05. Analysis was conducted using SPSS 17.0 (SPSS Inc., Chicago, Illinois, USA).
Results
Ideal S2AI trajectory parameters were obtained based on all volunteers. There is no statistical difference between the left and right sides of the same gender. The CA, MA, ML, NW, SD, MD, DD, and KD were 29.21 ± 6.52°, 39.75 ± 2.40°, 110.3 ± 7.22 mm, 16.60 ± 2.51 mm, 11.58 ± 1.18 mm, 26.5 ± 1.88 mm, 5.18 ± 1.08 mm, 39.25 ± 11.98 mm in males, and 35.21 ± 6.86°, 40.38 ± 3.58°, 102.64 ± 14.28 mm, 13.86 ± 2.65 mm, 10.83 ± 1.48 mm, 25.95 ± 1.28 mm, 4.60 ± 0.83 mm, 44.31 ± 9.20 mm in females, respectively. Among these parameters, CA, ML, NW, SD, and DD showed significant sex-related difference (p < 0.05; Table 1). Additionally, there is no significant age-related difference in all parameters. Bilateral S2AI screws were placed in all 48 patients and 96 screws were placed in total. (Table 2). There is no cortex violation-related complications occurred in all patients. One screw was placed with penetrated iliac cortex in the TGT group (3%, 1/39) but 10 screws were placed with penetrated iliac cortex in the freehand group (17.9%, 10/56). There is a significant difference between two groups (p < 0.05; Table 3) (Figure 4).
Parameters of optimal trajectory and comparison between different genders.

CA: cephalocaudal angle, MA: mediolateral angle; ML: maximal length of pathway, NW: narrowest width of the ilium along this pathway, SD: distance of the center of teardrop to sciatic notch, MD: distance of the start point to midline; DD: distance of the start point to inferior S1 dorsal foramen.
Demographics of the patients.
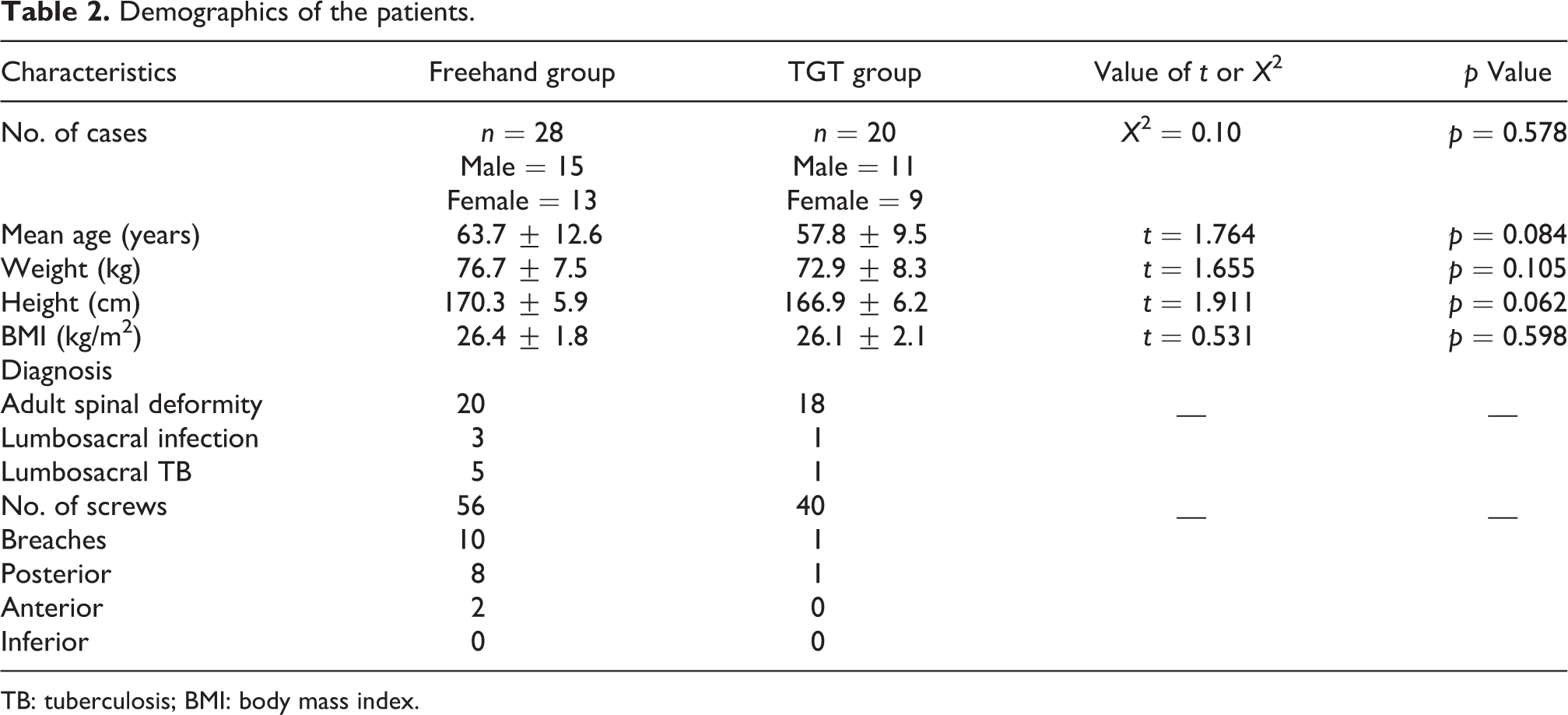
TB: tuberculosis; BMI: body mass index.
The comparison of the accuracy between freehand technique and TGT technique.

TGT: template guided technique.

The positions of S2AI screws are placed by two techniques. (a) A screw penetrated the medial iliar cortex by freehand technique is shown. (b) An excellent screw position by TGT technique is shown. S2AI: S2 alar iliac; TGT: template guided technique.
Discussion
Achieving pelvic fusion across the lumbosacral junction with the S2AI screw can be challenging for less-experienced surgeons in the management of spinal deformity. 4 Compared to other sacropelvic fixation techniques, S2AI technique has several theoretical merits including lower rate of implant failure and less surgical revisions. Additionally, the S2AI screw technique precludes the need for cross connectors, 4,9 which can significantly reduce the incidence of screw loosening. With lower screw prominence and deeper subcutaneous locations, S2AI screws are covered by full-thickness skin and subcutaneous tissue, which can significantly reduce the incidence of local skin ulceration and deep infection. 5,6 Furthermore, the direction and the length of the S2AI screw sacropelvic fixation provide more reliable stability compared to traditional iliac screw fixation. 13,14 However, in spite of emerging clinical evidence demonstrating the advantages of S2AI screws, the accuracy of S2AI screw placement remains concerns. The accuracy of S2AI screw placement depends on pelvic anatomic landmarks and trajectory.
Two start points were recommended for S2AI screw placement. One is the midpoint between the S1 dorsal foramen and the S2 dorsal foramen, where they meet the lateral sacral crest. The other is 1 mm inferior and 1 mm lateral from the S1 dorsal foramen. Two start points have different safety margins. However, in most cases, the difference between the two start points was considered negligibly in terms of safe screw insertion. 8 In this study, the point which was located lateral to the midpoint between S1 and S2 dorsal foramina and standing on the extending line from L5 and S1 pedicle screw anchor points was adopted as a start point and the optimal trajectory of the screw to be determined by the line connected the start point and the canal center of teardrop. The result showed that the CA of optimal trajectory is on average of 29.21 ± 6.52° in males and 35.21 ± 6.86° in females. CA presented significant differences between males and females. This result is consistent with a previous study from Zhu et al., and a radiographic study assessing optimal S2AI screw placement presented that CA in females has 4–5° more caudal trajectory compared with males. 15 But a study from Shillingford et al. showed that there are no significant differences in the CA or MA between females and males. 2 This study showed that there is no difference in MA between males and females with an average 40° (39.75 ± 2.40° vs. 40.38 ± 3.58°). This result is also consistent with the previous studies. 16 Based on this, the author recommended that S2AI screws of females should be placed 5° more caudally than males.
Whether the S2AI screws can penetrate the ideal iliac plane smoothly mainly depends on the iliac width, which is described as the NW within the iliar teardrop. Previous studies defined that the standard S2AI screws range from 70 mm to 100 mm in length and 5.0 mm to 7.5 mm in diameter. 10,17 A study from Wang et al. showed that the iliac canal width ranged from 17.4 mm to 32.4 mm in males and 13.5 mm to 20.3 mm in females in Chinese population. They suggested that the screws ranging from 5.0 mm to 7.5 mm in diameter can be appropriate. 18 This study showed that the NW was 16.60 ± 2.51 mm in males and 13.86 ± 2.65 mm in females. Although in females, the canal showed narrower with an average difference of about 3 mm frequently used screws in the clinical could go through the iliac canal without difficulty.
In the present study, the ML, SD, and DD showed a significant sex-related difference. These parameters depend on the morphology of the pelvis, which varied from 50 mm to 75 mm in practice. 19 In our study, the ML was 110.3 ± 7.22 mm in males and 102.64 ± 14.28 mm in females. The average max length of trajectory in females was approximately 8 mm shorter than that in males. Compared with the previous study from Zhu et al, 15 ML is different from their investigation in which the average max length of trajectory in females was approximately 5 mm shorter than that in males. In clinical practice, the optional S2AI trajectory exceeds more the length of usually used screw. Although O’Brien et al. consider that 65-mm length S2AI screw was equivalent to 80-mm length S2AI screw in respect of providing biomechanical purchase, 20 using longer screw was much more in surgery, which may consider the long-term stability of sacropelvic fixation particularly in long-range fusion. And if the stress of longer screw fixation can be distributed as far anteriorly and laterally to the spine as possible, more stability could be achieved. 13,14
Three-dimensional printing (3DP) has been developed as a promising innovation for many disciplines including medicine. For spine surgeon, they deal with complex pathologies of spine column, including deformity, trauma, and degeneration. A review from Alpaslan Senkoylu discussed the pros and cons of 3DP. The 3D models help surgeons to identified landmarks of anatomy and simplified surgical procedure, and it also can be a perfect instrument for improving patient–doctor communication. 21 The utilization of 3D models has been related to better doctor–patient relations and educated assent in adult and pediatric patients. Additionally, three-dimensional rapid prototyping (3DRP) technology became an excellent facility to avert the risks of complications by helping surgeons in determining the pedicle entry points and accurate trajectories for pedicle screw insertion by manufacturing 3D-printed guides according to the preoperative CT images. A study compared pedicle screw placement with 3DP jigs and freehand technique in complex deformities and higher accuracy was found in the 3DP jig group. 22 In this study, we used a 3D printed template to guide S2AI screw placement individually to avoid the screw penetration, which might arise screw-related complications. Compared with the freehand group, in which 10 screws penetrated iliac cortex, only one screw penetrated iliac cortex in the TGT group. The accuracy rate of the freehand and TGT group is 82.1% and 97.5%, respectively. The TGT technique is quite accurate. Additionally, other merits can also be obtained via the TGT technique. There is no need to probe to identify the integration of the track canal repeatedly, which could save surgery time. Second, CA and MA more rely on the surgeon’s subjective estimation during surgery because without objective measurement tool when placing S2AI screw in the freehand technique, there still has malpositioned screws even under repeated fluoroscopy. So, the TGT technique could surely decrease radiation exposure. Finally, the TGT technique is easier to study for less-experienced surgeons, who are not familiar with the complexomorphic pelvis, and easier to place the screw even for experienced surgeons when facing anatomically abnormal pelvis, which is not rare in congenital deformity. In this study, all the operations were finished by the same senior surgeon who was very experienced in spine surgeries. Even so, the TGT technique provides more accuracy compared with the freehand technique (only one screw penetrated iliac cortex). For less experienced surgeons, the TGT technique will be more useful and reliable, which helps them to insert the S2AI screws safely avoiding severe complications.
There are some limitations in this study. The parameters of optimal trajectory analyzed in our study were based on Chinese population. TGT technique is time-consuming and not suitable for urgent cases. It is crucial to closely match the guide template with the bone surface, otherwise, the technique has to be abandoned because of the potential wrong direction guided by the template and increasing risk of screw misplacement. The material for printing template and the precision of printing machine would influence the quality of template. Another limitation is that the practitioner need extra time to design the individual template if plans to perform the TGT technique. Pre- and postoperative CT scan means high radiation exposure for patients, which is an issue that can be overcome using imaging technique alternative for CT in the future.
Conclusion
Optimal position for S2AI screw placement in Chinese adult patients is starting at approximately 1 mm inferior and 1 mm lateral to the S1 dorsal foramen and go through the sacroiliac joints with approximately 30° of CA (5° more in females) and 39° MA. Additionally, either freehand or TGT technique is safe for S2AI screw placement. TGT technique is more accurate compared with the freehand technique.
Footnotes
Author contribution
KC and ZZ contributed to the conception. ZZ contributed to the designs and draft of the work and revised it critically for important intellectual content. ZZ, HY, and JX did the acquisition of data of the work. ZL, RZ, WW, ZP, and LC did the analysis and interpretation of data of the work. KC approved the version to be published. He agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. All authors read and approved the final manuscript.
Ethics approval
This study was approved by Ethic Committee of The Second Affiliated Hospital of Nanchang University.
Informed consent
Written informed consent was acquired from each of volunteers and patients to authorize treatment, imageology findings, and photographic documentation. The patients consented to the publication of their pictures as well as their anonymous and clustered data.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China [Grant No.81860473], 5511 Innovation-driven Program of Department of Science and Technology, Jiangxi Province [Grant No. 2165BCB18017], Health Commission of Jiangxi Province [Grant No. 20191029], and Department of Science and Technology of Mianyang City, Sichuan Province [Grant No. S16041].