
Abstract
Study Design
Broad narrative review.
Objectives
To review and summarize the evolution of spinopelvic fixation (SPF) and its implications on clinical care.
Methods
A thorough review of peer-reviewed literature was performed on the historical evolution of sacropelvic fixation techniques and their respective advantages and disadvantages.
Results
The sacropelvic junction has been a long-standing challenge due to a combination of anatomic idiosyncrasies and very high biomechanical forces. While first approaches of fusion were determinated by many material and surgical technique-related limitations, the modern idea of stabilization of the lumbosacral junction was largely initiated by the inclusion of the ilium into lumbosacral fusion. While there is a wide spectrum of indications for SPF the chosen technique remains is defined by the individual pathology and surgeons’ preference.
Conclusion
By a constant evolution of both instrumentation hardware and surgical technique better fusion rates paired with improved clinical results could be achieved.
Introduction
The reconstruction of a physiologically aligned lumbosacral junction with solid fusion where clinically indicated has been a long-standing challenge due to a combination of anatomic idiosyncrasies and very high biomechanical forces. Biomechanically, the lordotically angled lumbosacral alignment with its sagittal plane mobility and decreased mobility in the coronal axis creates an anteriorly directed translational shear force in addition to a directly vertical load. 1 The concentrated cumulative vector forces acting on this area result in the highest transitional strain found anywhere in the spinal column. 2 Clinical challenges in the realm of spinal trauma, oncology, infections and deformities have prompted surgeons to seek to develop newer techniques to reduce complications and achieve better fusion rates paired with improved clinical results. 3 Our Narrative Review aims to outline the evolution of lumbopelvic fixation and its impact on clinical care.
History of Non-Instrumented Spondylodesis
From 1914 to 1919, a ‘pioneer of spine surgery’, Russell A. Hibbs, treated fifty-nine patients with scoliosis with spinal arthrodesis and reported the outcomes of forty-five of these patients in 1924. 4 Facing the need for a lumbosacral arthrodesis in 3 out of fifty-nine patients, early on, he recognized the lumbosacral junction as “the point of greatest strain” in all trunk movement in the normal spine” and advocated arthrodesis of the lumbosacral junction “in cases of dorsal scoliosis with a marked lateral tilt of the fifth lumbar”. 5 Over the next decade, Hibb`s arthrodesis technique gained popularity for use in treating a diversity of spinal pathologies and was subject to modifications by a number of other surgeons, including Frederick Albee in New York City and Alexander MacKenzie Forbes in Montreal, Canada, who described their own spinal arthrodesis variations. In order to help achieve a fusion, Forbes detached chunks of bone from the lamina and the lateral surface of the spinous processes to denude the cortical surfaces and thus facilitate fusion. In contrast, Albee spliced a bridging cortical tibial autograft between the splinted spinous processes in the sagittal plane. 6 In 1933, Ralph Ghormley of the Mayo Clinic reconsidered Hibbs`s hypothesis of increased strain across the lumbosacral junction due to the biomechanical forces resulting from the interaction of the mobile spine with the relatively immobile pelvis. 7 He associated the strain experienced by the facet joints at the lumbosacral junction with therapy refractory low back pain and proposed lumbosacral fusion as last resort for treatment of patients with symptomatic lumbosacral spondylosis after failed conservative management. 7 Given the problems at this location, he suggested the use of autogenous iliac bone graft to augment arthrodesis. 7
Beginnings of Instrumented Lumbo-Sacral Spondylodesis
It is safe to say that the origins of instrumented spine surgery were quite improvisational given the many material and surgical technique-related limitations facing surgeons at the time and were mainly aimed at preventing disease progression rather than enabling restoration of compromised neural elements and restoring physiologic alignment. The birthing date of spinal instrumentation can probably be specified to the year 1891, when Berthold Hadra from Dallas, Texas, reported on his experience using silver wires wrapped around adjacent cervical spinous processes for treatment of a fracture-dislocation in a patient with Pott’s disease.
8
It took almost 20 years until 1910, when Fritz Lange of Munich, Germany treated a spondylotic spine by attaching a celluloid bar to either side of a spinous process with silk sutures and wire and reported improved fusion results.
9
The concept of a formal instrumented fusion with accompanying autologous bone graft was not used in the spine until the 1940s: King and Toumey were the first to perform instrumentation via facet joint fixation with screws across the joint and fusion with autologous bone-grafting to achieve immediate stability.10,11 Their “simplification of spine fusion technique by use of the bone bank”,
11
in situ fusion and prolonged immobilization via whole body casting remained as the main modality of achieving a lumbosacral fusion until the 1960s.
12
While these procedure variants remain of historical interest, they are of little value in current practices due to the need for prolonged external immobilization and bedrest to allow for adequate osseous healing while not endangering the hardware construct. In addition to the substantial care effort and many complications associated with prolonged recumbency, the associated pseudarthrosis rate was reported to be as high as 50%.13,14 The breakthrough for instrumentation systems of the thoracolumbar spine was the hook and rod based scoliosis fixation system primarily developed for patients suffering from polio by Paul Harrington from Houston, Texas in the 1960s.
12
It consisted of distraction and later compression Harrington rods (Figure 1), which could be attached to transverse processes or via lamina hooks and provided a chance to distract or compress across coronal plane deformities. One of its main advantages was its easy application in the thoracic spine and across the thoracolumbar junction. However, this instrumentation system struggled to accomplish adequate mechanical stability across the lumbosacral junction as shown in sacral hook dislodgements with rates as high as 26%. In response to this evident shortcoming, sacral bars were introduced in an effort to better control attachment points to the lumbosacral junction.
12
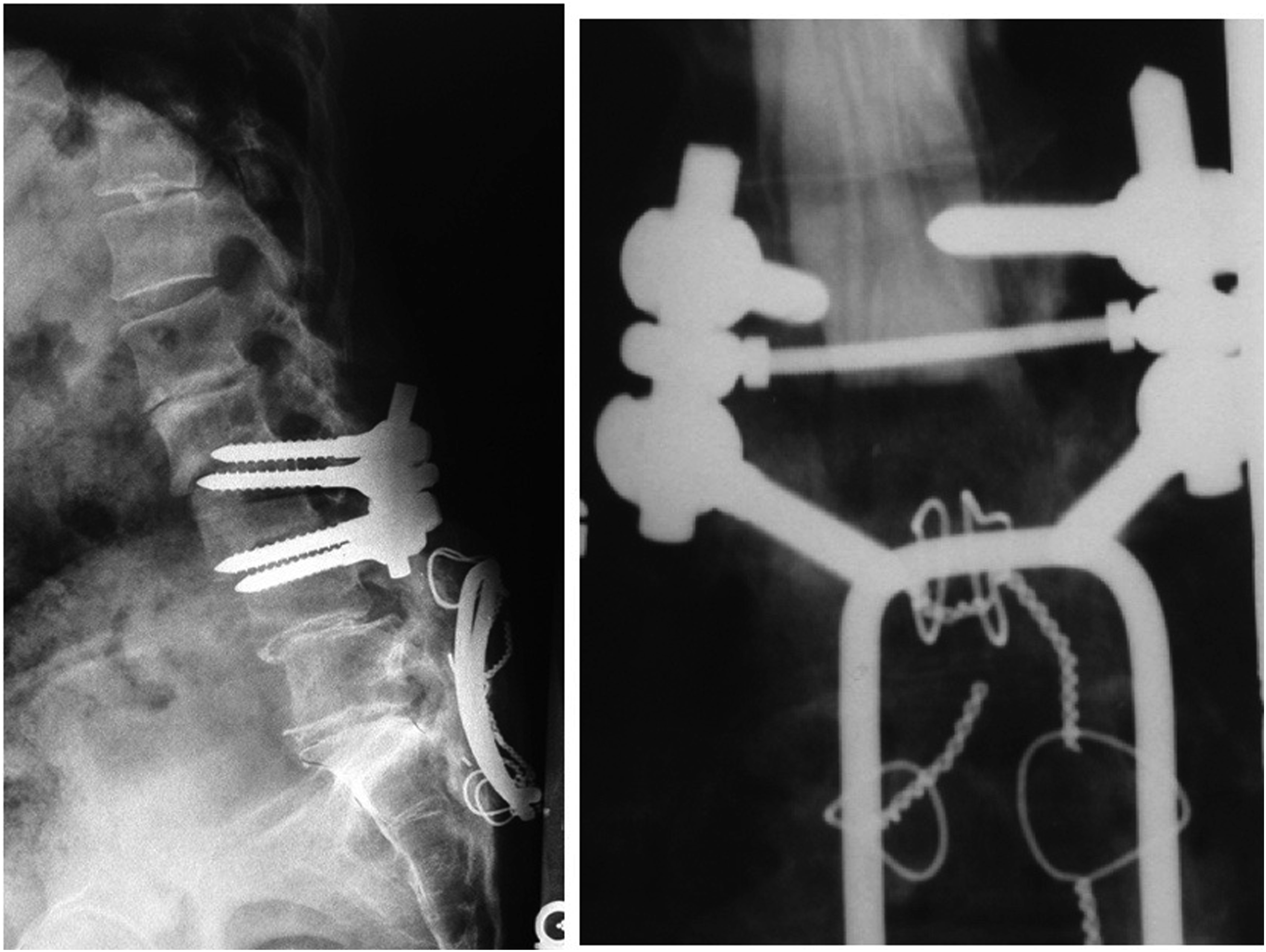
Nevertheless, pseudarthrosis rates as high as 40% were reported.14,15 Without question residual instability in flexion, rotation and side-bending concentrated at the lumbosacral junction, remained a significant weakness of the Harrington rod and it´s modifications.14,15 In order to reduce these shortcomings, Eduardo Luque in the 1970’s introduced the concept of “segmental instrumentation” which was based on multiple fixation points provided by sublaminar cable fixation and hoped to improve pelvic fixation through insertion of an L-shaped caudal end into the iliac crest using a quarter-inch (0.64-cm) Luque “L” rod.16,17 The L-shaped rod offered cephalad and caudad contouring to avoid rod migration. A compelling further advancement was its low-profile construct with which it could be used to bridge the lumbosacral junction in deformity or in case of complex sacral fractures (Figure 2). In contrast to the Harrington technique, which offered very limited spinal segmental fixation points, Luque´s segmental instrumentation concept allowed a differentiated correction in coronal and sagittal planes by multilevel sublaminar wire fixation, thereby reducing the ‘flatback-syndrome’ famously associated with Harrington rods.18,19 Through its use of multiple fixation points and accompanied increased construct rigidity, favorable fusion results seemed to become attainable, despite pseudoarthrosis rates between 6% and 41%.20,21 A well-known persistent shortcoming of this system was its inability to resist sagittal plane trunk flexion at the lumbosacral junction.
22
Another concern was the risk of dural injury and even nerve root compromise brought on by the attempt to pass sublaminar cables at L5 and the sacrum.
20
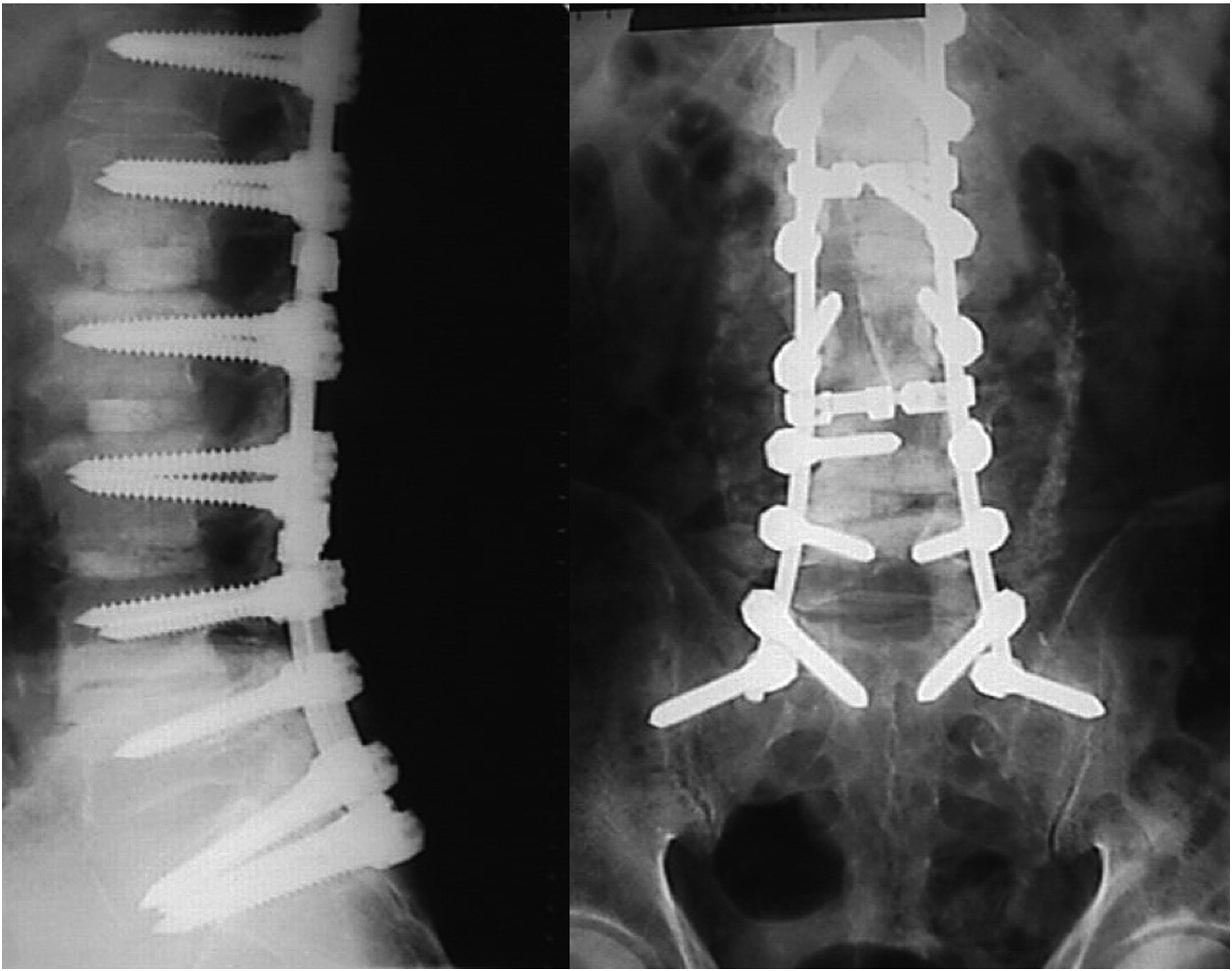
With the advent of the Cotrel-Dubousset concept of segmental multipoint fixation and derotation of scoliotic spinal deformity and 3-dimensional correction using a combination of hooks and monoaxial pedicle screws, much improved realignment results were combined with increased biomechanical construct strength (22). Such novel and truly segmental fixation options provided by individualized rod attachment points for the first time allowed not only pedicle screws in addition to hooks, but also sacral alar and iliosacral screws (Figure 3).
23
Despite this undeniable technologic advancement, there was still a relatively high pseudoarthrosis rate of 33% and pedicle screw pull out as high as 44% at the lumbosacral junction. This was again largely due to insufficient control of the long leverage arms brought on by the trunk mass especially in forward flexion and rotation at the caudal fixation points at the lumbosacral junction of adult patients.
24
This evident shortcoming of implant options opened the door to a plethora of improvised lumbo-sacral constructs using the tools available at the time in some largely improvisational applications. Harrington rods (left) are straight stainless-steel distraction rods which can be fitted with hooks at both ends and elongated via a ratchet. One common complication was the development of a flat back syndrome (right). Luque sacral loop, after distal junction failure. Sacral alar screws with sacral screw loosening.
The Dawn of Spino-Pelvic Fixation
The modern idea of stabilization of the lumbosacral junction was largely initiated in 1983, when Allen and Ferguson introduced the Galveston technique with the inclusion of the ilium into lumbosacral fusion (Figure 4).
25
The insertion of precontoured rods in “L” shape from the posterior superior iliac spine between inner and outer cortex of the ilium represented a major improvement in stability.
25
By augmenting instrumentation across the lumbosacral junction, the prevalent flexion moment and cantilever forces, that may contribute toward pseudarthrosis at the lumbosacral junction, could be reduced, thereby improving odds of fusion.16,25,26 Fusion rates up to 94% in their largely adolescent deformity patient population were achieved but there were still associated complications which were mostly mechanical in nature.16,25,27 Despite its low profile entry point at the posterior superior iliac spinous process (PSIS), implant prominence and wound healing issues were the most commonly described complications caused by the Galveston technique.
25
A typical failure seen with this lumbopelvic fixation was caudal end hardware loosening, radiographically described as a “wind-shield wiper” effect; nevertheless, this fixation technique constituted a significant step forward in achieving adequate lumbosacral fixation.28,29 In 1993, the concept of intrasacral rods were introduced to try to address the shortcomings of prominent hardware.
30
After analyzing CT scans of fifty patients, Jackson and McManus proposed to insert 7 mm rods in the lateral sacral masses as an early form of spinopelvic fixation. While this Jackson technique avoids potential damage to the sacroiliac joint and reduces the problem of prominent hardware, achieving inline fixation with S1 screws was difficult and there was an increased risk of fracturing the sacrum depending upon individual sacral morphology. Moreover, there were biomechanical limitations of this technique reported compared to iliac-screw based techniques.
31
Another variation was introduced by Kostuik who tried to improve fixation by trans iliac bars that he passed 1-2 cm anterior to the PSIS bilaterally and then connecting them to S1 screws. Using this technique Kostuik could achieve lumbosacral fusion in ninety of ninety-three adult patients who underwent a long spinal arthrodesis for scoliosis. Galveston Technique.
Traditional Iliac Screws
In the 1990s, driven by the need to more effectively treat complex sacral fracture patterns, several orthopedic trauma surgeons took the next steps towards a modern lumbopelvic fixation. In 1994, Käch and Trenz described a 2-point fixation technique for transforaminal sacral fractures.
32
The major shortcoming however was the missing vertical stability under full weight bearing conditions due to only a 2-point-fixation. Simultaneously, in 1994 Josten and Schildhauer published the concept of performing a ‘triangular osteosynthesis’ in a first case series.
33
In comparison to Käch et al, their triangular osteosynthesis concept between the lower lumbar spine and the ilium allowed for combined vertical and horizontal reduction maneuvers and 3-D multiple point fixation for increased mechanical stability.
34
Based on this technique, Schildhauer et al introduced the modern iliac screw fixation, which remains the most common modality used for sacropelvic fixation.34–38 A detailed anatomical understanding of the osteology of the ilium is important as misdirected screws might cause neurovascular damage, especially when perforating the ischial foramen.
39
To minimize screw misplacement, intraoperative fluoroscopic control was recommended using predictable angled views such as the obturator oblique–outlet (‘tear drop’and standard lateral pelvic (‘sciatic notch’) views to guide trajectory (Figure 5).
36
The suggested entry point of traditional iliac screws was originally suggested to be located at the PSIS.
35
This approach required subperiosteal dissection to expose the insertion point. After completed exposure of the PSIS was accomplished, an osteotome was used to create a focal osseous depression in the area of the intended starting spot to allow the screw heads to be recessed below the iliac crest to avoid excessive soft tissue infringement. While the authors differentiated 3 different screw placement trajectories, either (1) through the iliac tubercle and AIIS, (2) through a point directly above the PIIS and AIIS or (3) a plane through the PSIS and AIIS, the preferred path was the 1 from PSIS to AIIS.
36
This trajectory allowed for the longest screw lengths in both gender, with an average length of 141 mm in male and 129 mm in female patients,
36
as subsequently confirmed Berry et al.
40
Furthermore, this PSIS-AIIS trajectory enables cortical purchase at 2 narrow intercortical iliac junctions located approximately at the anterior joint surface of the sacroiliac joint and the iliac wing just anterior and superior to the greater sciatic notch, while simultaneously avoiding violation of the so called ‘photoluminescence area’ (PLA), which is a known very thin monocortical weak spot of the iliac wing.35,41 These narrow intercortical areas limit transiliac screw diameter and suggest screw sizes of up to a 8 mm diameter in male and 6 to 7 mm in female patients under inclusion of the cortical bone in the overall transcorticomedullary thickness of the ilium.
35
Considering iliac screw design with regards to optimizing screw pullout strength, Schildhauer et al recommended against using conically shaped screws in order to optimize cortical anchorage and to maximize actual bone–implant interface.
42
By implementing the above-mentioned technique using threaded and thicker diameter iliac screws, the cortical anchorage proved to be of clear fixation benefit, compared to the smooth surfaced Galveston rod or historically undersized posterior pelvic crest screws, which can lead to the undesirable radiographic windshield wiper sign representative of loosening of the pelvic anchorage.24,25,43–45 While these dedicated iliac screws represented a significant refinement of the Galveston technique by providing more definitive iliac anchors that allowed for modular connectivity with modern posterior spinal fixation systems, their limitations were associated with the more extensile posterior subfascial exposure of the PSIS, also a real risk of hardware prominence related to the iliac screw starting point and further coupling problems related to the off-center rod placement necessary to mate the typical S1 screw line with this more lateral starting point, that might prompt the surgeon to use biomechanically inferior side opening screw-to-rod connectors.46–50 Intraoperative C-arm positioning for Iliac Screw placement: A: Lateral view confirming safe distance to the ischial foramen and hip joint. B: Obturator outlet view showing the “tear drop” view confirming intraosseus trajectory C: Obturator inlet view confirming intraosseus trajectory and avoidance of medial and intraarticular perforation.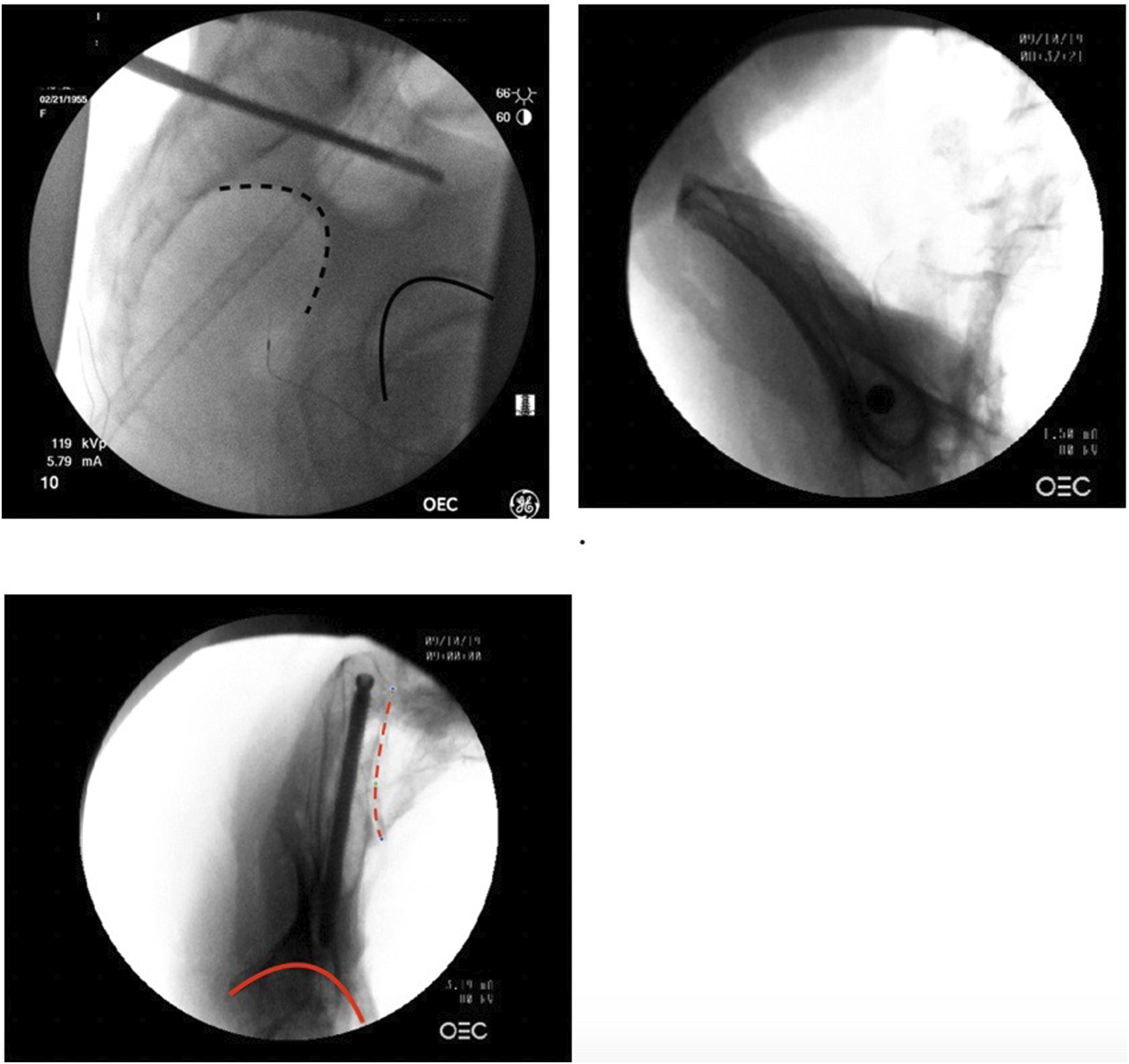
S2-Alar-Iliac Screws (S2AI)
To counter such perceived or real shortcomings and limitations of conventional iliac screw fixation technique, the S2-alar-iliac screw (S2AI) was first described in 2007 by Sponseller and Kebaish. 51 The insertion point is described as usually being 10 mm lateral to the sacral midline, located between the S1 and S2 foramina and usually starts on the medial prominence of the rudimentary S1-2 facet joint adjacent to the sacroiliac joint. The preferred trajectory was described to be within 30-40° lateral angulation in the transverse plane and 20 to 30 degrees of caudal angulation in the sagittal plane with an inclination towards the anterior inferior iliac spinous process (AIIS). The measured screw lengths usually were reported to be between 60 and 90 mm length with an 8 to 9 mm diameter.52,53 Typical fluoroscopy based images consisting of anteroposterior, obturator-outlet and teardrop-views were used to ensure correct screw placement with fluoroscopy. 54 Similarly, navigation and robotics can be used to aid with placement as the pelvic crest offers a stable platform for reference anchors for such a navigational system. One of the distinct advantages of S2AI screws was their improved vertical alignment with S1 screws, therefore obviating the need for a more extensive lateral dissection or a separate incision. Such S2AI screw heads usually come to lay in line with the more cephalad screw heads, thus making rod insertion and screw connection easier and obviating the need for mechanically inferior offset connectors. 55 Further, these screw heads were positioned deep enough between the posterior iliac crests to reduce hardware prominence and reduce patient discomfort. In a clinical comparion study Guler et al found a 35% failure-rate in adult degenerative scoliosis surgery using S2AI screw anchors compared to 12% with traditional iliac screws leading the authors to suggest that the type of spino-pelvic fixation (SPF) was the primary factor for failure in these patients despite the use of offset connectors with traditional iliac screws, which may present a possible weak link in this application.56,57 Guler et al hypothesized that increased stresses at the junction of the screw head and shaft interface created an acute angle, and this was thought to be the cause for the increased rate of mechanical failure using S2AI. 57
Indications for Spino-Pelvic Fixation
Spino-pelvic fixation (SPF) can be of benefit in the management of a number of spine pathologies as a biomechanically advantageous construct by providing a secure anchoring foundation. A commonly agreed upon indication for SPF is a long thoraco-lumbo-sacral arthrodesis surgery of 5 or more levels terminating at the sacrum. 23 Biomechanical evidence provided by Cunningham et al suggests that for instrumented arthrodesis extending above L3, sacral screws are preferably protected with supplemental iliac screws or additional spinopelvic fixation. 58 Spino-pelvic fixation may also benefit patients with high-grade spondylolisthesis (grade 3 or higher according to the Meyerding classification system), in which large shear forces challenge reduction and fixation attempts across the lumbosacral junction. 59 By virtue of their unparalleled fixation strength - if done properly - spino-pelvic fixation can provide critical supplemental foundation anchorage to aid in spondylolisthesis reduction efforts by decreasing the shear loads sacral screws are subjected to during maturation of the fusion. 60
Similarly, major three-column osteotomies deformity correction procedures in the lower thoracic spine or lumbar spine, such as intradiscal osteotomies, pedicle subtraction or vertebral column resections usually benefit from additional caudal stabilization provided via SPF.61–63 In these cases, spinopelvic fixation can be a desirable adjunct to enhance stability across the lumbosacral junction as foundation for a newly restored thoracolumbar spinal column and to facilitate arthrodesis. Lumbar deformity and pelvic obliquity correction, especially in children with neuromuscular deformity, are other indications for spinopelvic fixation. Placing anchors in the sacrum alone is frequently insufficient to achieve and maintain the necessary correction due to shorter screws and anchorage in sparse trabecular sacral bone rather than between cortical constrictions within in ilium.16,64 As advocated by Jacobs et al. another indication is in the treatment of Charcot arthropathy of the lumbar spine with a lumbopelvic quadruple-rod construct.65,66 This mitigates flexion, extension and axial rotation at L5-S1 and especially in paraplegic patients, who bear excessive multidirectional lumbosacral loads during bed transfers and mobilization, and has been shown to decrease the instrumentation failure rate in short-term follow up.67–69 For trauma patients, complex sacral fractures, sacropelvic dislocations, pelvic ring disruptions and fracture dislocations involving the lumbosacral region often require reduction and stabilization with lumbo-pelvic fixation.46,70–74 Similarly, patients with destructive lesions from oncologic and infectious diseases involving the lumbosacral region benefit from stable SPF.
Traditional Iliac Screw Fixation Vs. S2AI: Current Controversies
Regarding clinical advantages of either technique, current literature can be quoted in support of either technique, though none of these studies assesses cost of surgery, quality of life, satisfaction levels and cost efficacy analysis.75–77 Contrary to Guler et al, Gao et al found that sacropelvic fusion (SPF) using S2AI screw was associated with a lower risk of implant failure (S2AI, 12%; IS, 26%), as well as a lower risk of screw loosening (S2AI, 8%; IS, 20%) and screw breakage (S2AI, 2%; IS, 12%), which were the 2 main complications of implant failure.51,57,78,79 A Level 1 study by Keorochana et al compared S2AI screws with iliac screws in the pediatric and adult population and concluded that iliac screw fixation was associated with higher complications and increased rates of revisions, mostly due to hardware prominence. 77 While these findings were similar in both adult and pediatric population, there was no difference in the VAS scores between the 2 groups. 77 These findings were also confirmed by De la Garza Ramos et al, who included 5, level III evidence studies in their meta-analysis. 75 They also reported a comparatively decreased incidence of complications as well as biomechanical failure with S2AI in adult spine surgery. 75 Gao et al carried out a meta-analysis comparing the outcomes of S2AI with traditional iliac screws within different patho-entities including deformity and trauma. Taken together, S2AI screw shows an effective maintenance of the correction and arrest of progression of deformity, which was equal or better than iliac screw fixation. 76 While S2AI screws have been evaluated mainly in the setting of ADS,76,80 certain pathologies require, of course, traditional or modified iliac screws due to the nature of the underlying disease process. For instance, complex sacral fracture patterns may require decompression and complex reduction maneuvers between the sacrum and pelvis, which cannot be achieved with the S2AI trajectory.47,70,72,81 Moreover, sacral metastases or primary neoplasms can create difficult or impossible situations for S2AI placement due to required resection margins.82,83 The range of indications caused by the inherent technical limitations of the S2AI technique may, however, introduce a considerable selection bias in comparison studies.32–34 While the S2AI technique was most commonly used in stable conditions like ADS,75,80 patients treated with traditional iliac screws frequently included patient cohorts featuring patients with highly unstable lumbosacral disruption secondary to trauma or tumors, which inherently sets up a risk of increased complication rates.46,72 Moreover, while the use of traditional iliac screws does not demand offset connectors in the absence of S1 screw fixation points, which are not necessary in cases of the above-mentioned trauma and tumor cases.34,46,84
Additionally, a higher disease burden, for instance involving prolonged intensive care, may predispose these patients to medical complications as well as wound healing complications caused by immobility and prolonged ventilation.48,53,85,86 Many earlier studies also relied on traditional first-generation iliac screws. Tsuchiya et al described a loosening rate up to 43.2 % after long fusions as well as an iliac screw failure rate of 6 % with first generation screws. Further review of this specific study, however, revealed that these screws were clearly undersized with reported lengths of 60-70 mm and 7.5 mm diameter. 60 While those earlier iliac screws offered a partial thread and a conical shape, 80 modern iliac screws offer additional options such as dual outer diameter screws which provide a deeper iliac insertion by a nominal distal diameter. This provides a better cortical and cancellous purchase especially in osteoporotic bone. 13 Furthermore, closed head dual outer diameter screws provide a maintained core diameter and allow better guidance between the cortical walls combined with a better cancellous purchase. These dedicated polyaxial screws provide not only an arch of 15° head tilt, but 30° angulation in all planes. 13 These newer dedicated screw designs also have been reported to have significantly reduced screw related complications in iliac fixation: Nguyen et al. described a 3.5% iliac screw loosening rate and in 260 patients with 2 year follow up. 87 In a metanalysis Hasan et al compared post-operative complications between iliac and S2AI screw techniques. They concluded that S2AI screws had a lower profile and thus had a significant impact in reducing complications associated with conventional iliac screws, but they also highlighted the concern of sacroiliac joint violation with S2AI screws. 80 The authors did emphasize that modifications of iliac screw insertion technique could reduce complications associated with screw prominence. 80
In 2009, Harrop et al used an anatomical model to describe a low-profile anatomic/modified iliac screw technique (MiS) which spares the erector spinae muscles and obviates the need for an offset connector while providing inline fixation (Figure 6).
88
Cadaveric studies have shown a similar hardware prominence using the modified iliac screw while equally obviating the need for an offset connector and, therefore, a possible weak link.
50
Clinical studies confirm the feasibility and applicability of the modified iliac screw as an acceptable alternative for lumbopelvic fixation, offering the benefits of iliac screw fixation in terms of screw length and size while avoiding its frequently discussed disadvantages, namely offset connectors and screw prominence.
89
Comparison of all three techiques (left: traditional iliac screw, middle: S2AI, right: modified iliac screw. Below left sided traditional iliac screw in cadaver, right sided modified iliac screw in cadaver.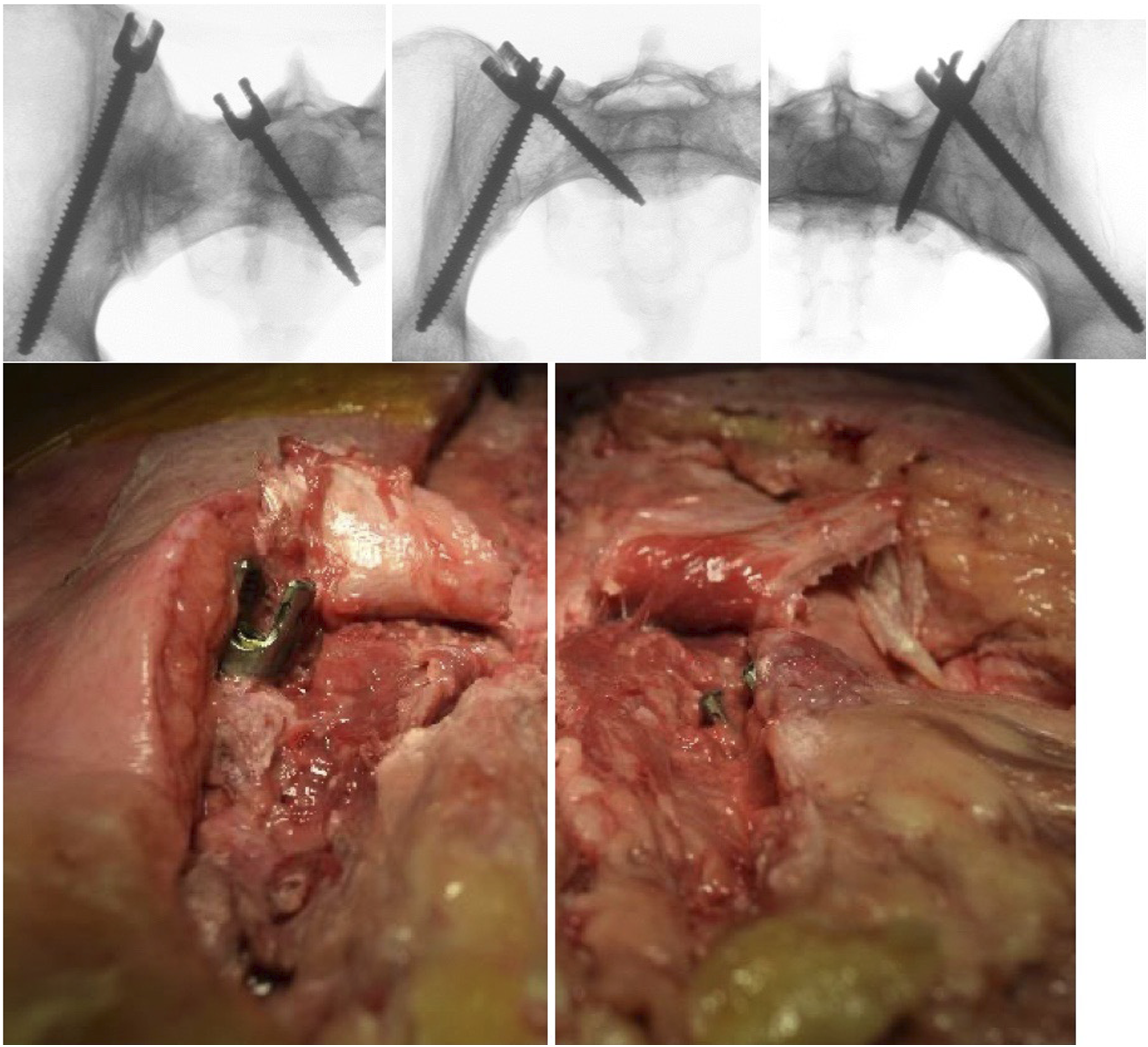
Due to the medialized entry point at the level of the PSIS, the modified iliac screw does not only provide a similar hardware prominence compared to the S2AI, but more importantly avoids the mechanically inferior use of offset connectors, 89 which have been clinically associated with higher instrumentation failure rates, increased wound healing complications and increased need for revision surgery.46,51–53,57,87 Since it is largely coaxial with the iliac tables it also allows for longer screws to be placed.
The Role of Image Guidance Systems
The evolution of image guidance systems has further enhanced the comfort level of general Spine surgeons toward placement of pelvic ring fixation. From the beginnings of blind more proprioceptively and direct exposure guided placement of instruments like lower Galveston rod ends into the pelvis, towards more directed use of image intensifiers and direct radiographs the emergence of navigational systems and augmented reality guidance technologies puts placement of iliac screws in the reach of surgeons without dedicated training. In theory, referencing attachments anchored in the posterior ilium can allow for reliable indirect planning of execution of complex pelvic screw trajectories. Despite absence of larger long term outcomes studies, these surgeon enabling technologies also make percutaneous iliac screw placement possible. The use of augmented reality technologies presents an interesting next step in aiding placement of complex iliac screw hardware in a complex but relatively stable posterior pelvic ring.84,90–92
Conclusion
Lumbopelvic fixation has evolved substantially since the 1960s, in concert between greater general appreciation of the role the pelvic ring in managing spinal deformities and growing sophistication of spinal fixation technologies. The continuous evolution of management strategies for pathologies involving fixation in and around this challenging junctional area has resulted in unprecedented mechanically sound pelvic fixation as a safe and feasible option. The 2 most widely accepted techniques today, S2AI and iliac screw fixation techniques, offer comparable biomechanical stability and rates of fusion, though often described for different surgical indications. While recent studies of the S2AI technique report lower rates of instrumentation-related complications and reoperation rates compared with first generation conventional iliac screw fixation, such iliac screws offered a decreased direct load compromise of the sacrum and SI joints. Using the recently described modified ilium screw entry point, iliac screw fixation has evolved into a preferable form of fixation due to its advantageous more sizeable screw dimensions and option to place several ‘stacked’ ipsilateral ilium screws if needed. Especially complex sacral fractures requiring reduction maneuvers or extensive sacral tumor resection, continue to make iliac screw fixation an indispensable option in which the often-criticized offset connectors can be avoided without the use of S1 screws. Moreover, with the previously mentioned modifications, the often-mentioned shortcomings of the traditional iliac screw can easily be avoided.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was organized and funded by AO Spine through the AO Spine Knowledge Forum Trauma, a focused group of international Trauma experts. AO Spine is a clinical division of the AO Foundation, which is an independent medically-guided not-for-profit organization. Study support was provided directly through AO Network Clinical Research.