
Abstract
Background:
The coracoclavicular fixation with suture anchors adds stability to type IIb distal clavicle fractures fixed with a plate and screws when loaded to failure. The purpose of this study was to compare the clinical and radiological outcomes between the use of a locking compression plate (LCP) with all-suture anchor fixation and hook LCP fixation of Neer IIb distal clavicle fractures.
Methods:
A total of 82 consecutive patients who underwent plate fixation for Neer IIb distal clavicle fractures were included. The subjects were divided into two groups: an LCP with all-suture anchor fixation group and hook LCP fixation group. For clinical assessments, the American Shoulder and Elbow Surgeons score, Korean shoulder score (KSS), and Constant score were recorded. A percentage of the coracoclavicular distance (CCD%) was used to evaluate fracture reduction. Typical reported complications, such as secondary dislocation, implant failure or loosening, peri-implant fracture, acromion osteolysis, stiffness, peri-anchor osteolysis, postoperative acromioclavicular joint arthrosis, nonunion, or delayed union, were also analyzed.
Results:
There were no differences in the clinical and radiological outcomes at the final follow-up between the two groups. The period for bone union and CCD% showed no significant differences between groups. Stiffness at 3 months after surgery of LCP with all-suture anchor fixation (n = 3, 10.7%) was less than that of hook LCP fixation (n = 17, 31.5%). The complication rate also showed no significant differences between groups. However, LCP with all-suture anchor fixation had anchor-related complications, although it can reduce hook-related complications.
Conclusion:
LCP with all-suture anchor fixation showed satisfactory outcomes in comparison with hook LCP fixation. In Neer IIb distal clavicle fractures, LCP with all-suture anchor fixation is a useful method for the maintenance of reduction, avoiding implant removal, and hook-related complications. However, anchor fixation should be carefully used, especially in osteoporotic patients or patients with underlying diseases.
Level of Evidence:
Level III, retrospective study.
Introduction
Distal clavicle fractures are rare, accounting for approximately 15–25% of all clavicle fractures. 1 Neer classified these fractures based on the location of the fracture line relative to the coracoclavicular (CC) ligaments and acromioclavicular joint (ACJ). 2 Neer type II and V fractures are unstable, and their treatments remain controversial. 3,4 Various treatment options have been described, including open reduction and internal fixation (ORIF) with hook plate fixation, tension band wiring, screw fixation, and distal locking plates. 5 –8
Hook plate osteosynthesis is an ACJ-spanning procedure that can be used to recreate CC stability more effectively than isolated locking plate osteosynthesis. 9 However, a second surgery to remove the hardware to prevent subacromial impingement and rotator cuff tears is essential, and various complications associated with the subacromial space positioning of the hook have been reported. 10,11
Despite satisfactory clinical outcomes following isolated locking plate osteosynthesis without additional CC stabilization, the delayed union or nonunion rate was up to 10%. 7,12,13 Furthermore, Shin et al. showed that locking plate osteosynthesis alone may not fully restore the preinjury coracoclavicular distance (CCD) for the treatment of Neer IIb distal clavicle fractures. 5 Recently, additional suture anchor fixation with LCP osteosynthesis was developed to overcome this limitation. 14 –16 In 2013, Madsen et al. 16 described that CC fixation with suture anchors adds stability to type IIb distal clavicle fractures fixed with a plate and screws when loaded to failure. However, comparative in vivo analysis of a locking compression plate (LCP) with all-suture anchor fixation and hook plate fixation was limited. To our knowledge, we believe this is the first study of the clinical and radiological outcomes of all-suture anchor fixation for additional CC fixation.
The purpose of this study was to evaluate the clinical and radiological outcomes of LCP with all-suture anchor fixation for Neer IIb distal clavicle fractures in comparison with hook LCP fixation. We hypothesized that the union period, union rates, and CCD between the two groups would not differ, but LCP with all-suture anchor fixation would exhibit lower complication rates and better clinical outcomes than hybrid LCP fixation.
Method
This study was approved by our institutional research ethics committee, and informed consent was obtained from all patients. We enrolled 82 consecutive patients who underwent ORIF with LCP with all-suture anchor fixation or hook plate fixation for Neer IIb distal clavicle fractures at our institution from January 2011 to March 2019.
Unstable distal clavicle fractures were clinically and radiologically diagnosed. The clinical diagnosis was based on an assessment of pain and tenderness occurring after frank injury. Preoperative radiological examinations included anteroposterior and cephalic tilt views taken with the shoulder fixed in the same position to minimize the impact of inconsistent posture in the interpretation of the radiographs. To confirm the definite fracture site, location of fracture fragments, and degree of comminution, three-dimensional computed tomography (CT) was performed on all patients preoperatively. Fracture patterns were classified after a review of the radiographs and CT images of the patients.
We employed a retrospective comparative cohort study design with the following inclusion criteria: (1) acute and isolated Neer IIb distal clavicle fracture; (2) operative treatment using LCP with all-suture anchor fixation or hook LCP fixation; (3) minimal follow-up period of 12 months after surgery; and (4) history of painless and unrestricted shoulder function prior to trauma. The exclusion criteria were as follows: (1) previous surgical history of the affected shoulder and (2) concomitant fracture around the affected shoulder. The subjects were divided into two groups: an LCP with all-suture anchor fixation group and hybrid hook plate group. LCP with all-suture anchor fixation was used in the final 28 cases, and hybrid hook plate fixation was used in the first 52 consecutive cases. Two patients who underwent LCP with all-suture anchor fixations were converted to hook LCP fixation because the anchors pulled out during surgery. As a result, the number of anchor LCP cases was 28, and the number of hook LCP cases was 54 (Figure 1). Data were collected to define patient characteristics, injury mechanisms, time to surgery, follow-up period, operative time, and estimated blood loss.

Study flow diagram. LCP: locking compression plate.
Surgical procedure of LCP with all-suture anchor fixation
All surgeries were performed under general anesthesia with the patient in the supine position and their chest elevated at 30°. A sabre cut incision (5–6 cm) was performed medial to the ACJ. The deltoid-trapezoidal fascia was incised in line with the lateral clavicle. A triple-loaded Y-Knot® RC All-Suture Anchor (ConMed, New York, NY, USA) was inserted after a 2.8-mm Y-Knot® RC disposable drill bit without additional deltoid detachment from the anterior clavicle under fluoroscopy (Figure 2). After the reduction was held with Kirschner wires, the LCP (TDM, Seoul, Korea) was placed on the fracture site. After plate fixation with several cortical screws, locking screw fixation of both the medial and lateral fragments was performed. The sutures were pulled through the holes of the plate, and five knots were tied (Figure 2). Although additional CC ligament repair was not performed, a delto-trapezius fascial repair for reinforcement was performed securely over the plate.

(a) Preoperative anteroposterior radiographs showing a Neer type IIb distal clavicle fracture. (b) The anchor was inserted without additional deltoid detachment from the anterior clavicle under fluoroscopy. (c) The sutures were pulled through the holes of the plate, and five knots were tied. (d) Postoperative radiograph after LCP with all-suture anchor fixation. LCP: locking compression plate.
Surgical procedure for hook plate fixation
The same position, approach, and reduction were used for LCP fixation.
After exposure and reduction of the fragments, the reduction was performed with Kirschner wires. A hook LCP (TDM, Seoul, Korea or Synthes, Solothurn, Switzerland) was placed under the acromion and on the fracture site, extending medially. After plate fixation with one or two cortical screws, we checked the reduction status, depth of the hook, and contour of the plate on the distal clavicle under fluoroscopic guidance. Subsequently, locking screw fixation of both the medial and lateral fragments was performed. Although additional CC ligament repair was not performed, a delto-trapezius fascial repair for reinforcement was performed securely over the plate (Figure 3).

(a) Preoperative anteroposterior radiographs showing a Neer type IIb distal clavicle fracture of the left shoulder. (b) Plain radiograph obtained 12 weeks after surgery showing complete union. (c) Plain radiograph obtained after implant removal showing restoration of the CCD percentage. CCD: coracoclavicular distance.
Postoperative rehabilitation and implant removal
The affected arm was kept sled for 6 weeks after surgery. Pendulum, self-assisted circumduction, and gradual passive range of motion (ROM) exercises were started 3 days after surgery, as tolerable. Active ROM exercises were started 6 weeks after surgery. In the hook LCP group, after 3 months, the implant was removed if bone union was achieved; if not, implant removal was delayed until union was observed. If the patient experienced shoulder stiffness at the time of implant removal, brisement or arthroscopic capsular release under general anesthesia was performed concomitantly. In the anchor LCP group, the implant was removed in nine patients to decrease the impingement of implants.
Clinical and radiologic evaluations
For clinical assessments, the visual analogue scale, American Shoulder and Elbow Surgeons (ASES) score, Korean shoulder score (KSS), and Constant score were recorded by the physician assistant at the final follow-up.
For radiological evaluations, anteroposterior views of both clavicles were taken regularly after surgery (at 3, 6, and 12 weeks; 6 months; and 1 year). In the hook plate group, the patients who did not achieve union at 12 weeks after surgery were followed up each month until bone union was achieved for early removal of the hook plate. Bone union was defined as a bridging callus across the fracture site or invisible fracture line. A percentage of the CCD was used for the evaluation of fracture reduction (Figure 4), which was calculated using the following formula:

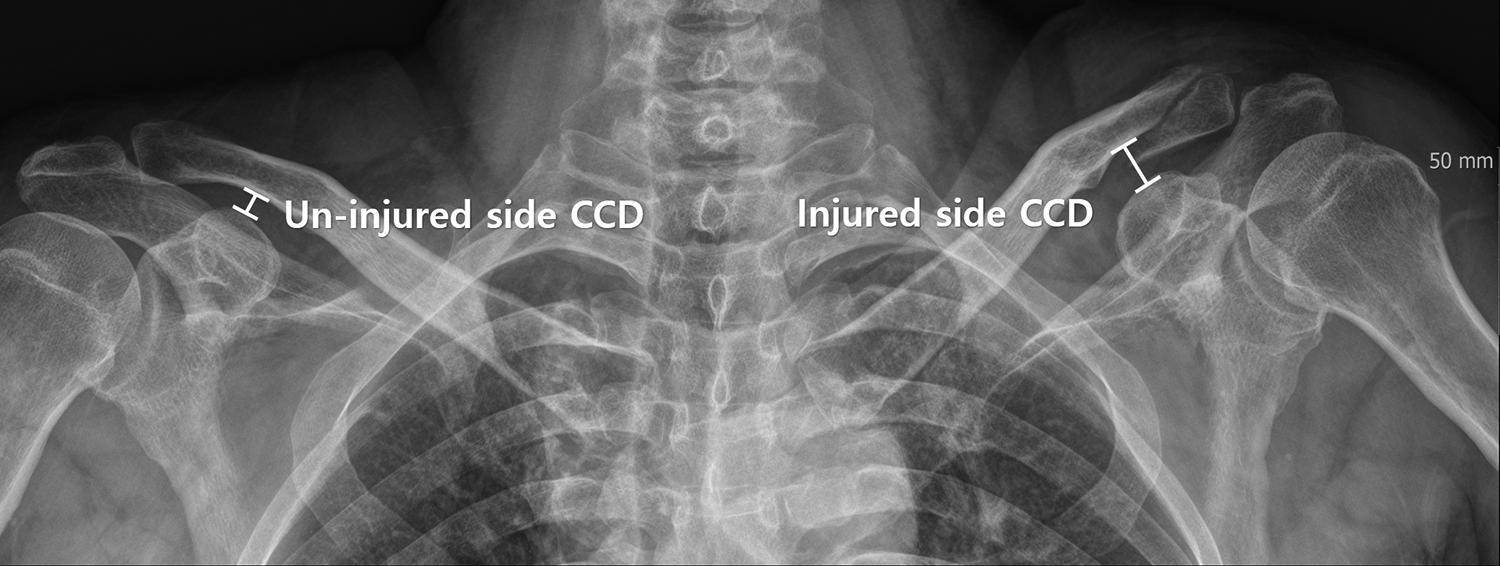
The CCD was measured between the uppermost border of the coracoid process and the lateral aspect of the conoid tubercle. The CCD ratio was measured using the CCD and compared with that of the contralateral shoulder on a standard radiograph. CCD: coracoclavicular distance.
For deltoid muscle volume evaluation, preoperative and l-year postoperative shoulder CT images were used. The cross-sectional area of the deltoid muscle was measured on axial CT at three positions: the upper and lower edges, and the middle of the glenoid (Figure 5). 17 The mean value of the three positions was calculated for deltoid muscle volume evaluation, and the ratio of the deltoid muscle volume was calculated using the following formula:


Six months after LCP with all-suture anchor fixation in a 63-year-old man with a peri-anchor cyst, loosening implant, loss of reduction, and nonunion. LCP: locking compression plate.
All radiologic measurements were analyzed by two independent examiners (KYK and JSY). The individual value was measured, after which the individual mean value was calculated. All radiographs were evaluated for the time period required for fracture consolidation and adverse events, including the typical reported complications of both procedures, such as secondary dislocation, infection, implant failure or loss of reduction, subacromion osteolysis, peri-anchor osteolysis, peri-implant fracture, postoperative ACJ arthrosis, and nonunion or delayed union (Figure 5). Delayed union was defined as incomplete radiographical consolidation >6 months after surgery.
Statistical analyses
To determine the normal distribution of continuous data, a Kolmogorov–Smirnov test was performed. Continuous variables were analyzed using an independent t-test, and noncontinuous variables were analyzed using a Pearson χ 2 test. All statistical analyses were performed using the Statistical Package for Social Sciences version 25.0 (SPSS, Inc., an IBM Co., IL, USA). Statistical significance was considered at a p value <0.05 for all analyses.
Results
Demographic data
The study included 29 women and 53 men, with ages ranging from 20 to 76 years. The initial injuries were caused by traffic accidents in 34 cases, falls in 35 cases, and sport-related injuries in 13 cases. No significant differences were found in the demographic data, time to surgery, operative time, and mean follow-up period between the two surgical groups (Table 1).
Demographic data.

ASA: American Society of Anesthesiologists; LCP: locking compression plate.
Clinical outcomes
There were no differences in the ASES score, KSS, and Constant score at the final follow-up between the two groups. The mean ASES scores were 89.6 ± 12.2 and 90.8 ± 11.3 in the hook and anchor LCP groups (p = 0.615), the mean KSSs were 87.3 ± 11.9 and 89.2 ± 12.4 in the hook and anchor LCP groups (p = 0.781), and the mean Constant scores were 86.1 ± 8.9 and 86.8 ± 9.6 in the hook and anchor LCP groups (p = 0.403), respectively. Furthermore, 61, 9, 7, and 5 patients obtained excellent, good, satisfactory, and fair results, respectively. Of the five patients who showed fair results, two patients had peri-hardware fractures, one patient had severe subacromial erosion, one patient had post-traumatic ACJ arthrosis, and one patient had nonunion. The incidence of stiffness at 3 months after surgery was significantly higher in the hook LCP group than in the anchor LCP group (p = 0.038); the incidence was reported in 17/54 (31.5%) and 3/28 (10.7%) patients in the hook LCP and anchor LCP groups, respectively, although pendulum and self-assisted circumduction exercises were started on the first postoperative day. Brisement was performed in 17 patients in the hook LCP group who experienced postoperative stiffness during the implant removal operation. All patients recovered full ROM at the final follow-up.
Radiologic outcomes
There were no differences in the time for bone union between the two groups (p = 0.829); the mean times for bone union were 14.5 ± 5.2 and 14.2 ± 3.2 weeks in the hook and anchor LCP groups, respectively. There were no significant differences in the CCD values between the treatment groups (p = 0.997, 0.820). The mean CCD% decreased from a preoperative value of 210.3 ± 79.1% to a follow-up value of 105.3 ± 31.2% in the hook LCP group, whereas the mean CCD% decreased from a preoperative value of 209.7 ± 89.4% to a follow-up value of 107.1 ± 36.3% in the anchor LCP group. There were no significant differences in the deltoid volume ratio between the two groups (p = 0.543). The mean deltoid ratios were 95.3 ± 18.7% and 94.4 ± 17.2% in the hook and anchor LCP groups, respectively (Table 2).
Clinical and radiological outcomes between the two groups.
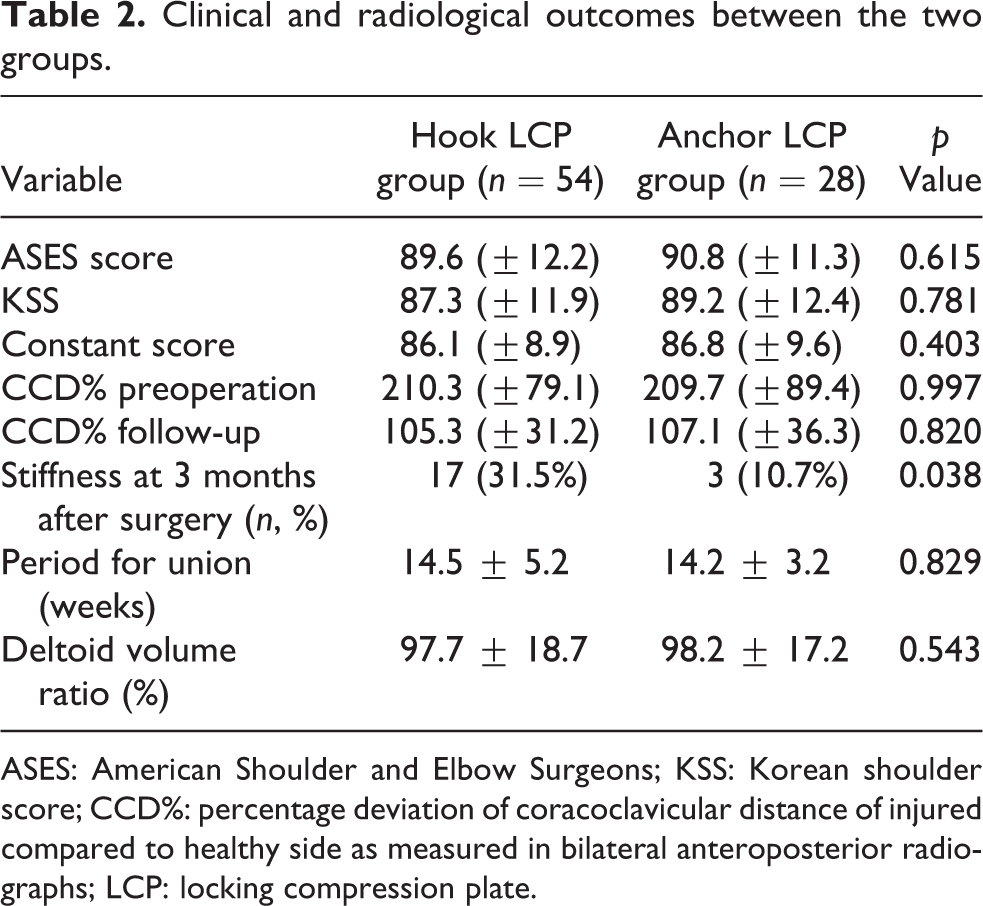
ASES: American Shoulder and Elbow Surgeons; KSS: Korean shoulder score; CCD%: percentage deviation of coracoclavicular distance of injured compared to healthy side as measured in bilateral anteroposterior radiographs; LCP: locking compression plate.
Complications
There was no difference in the complication rates between the treatment groups. The number of overall complications was 24 (44.4%) and 12 (42.8%) in the hook and anchor LCP groups, respectively (p = 0.487). There were two cases in the hook LCP group that could not achieve bone union at 6 months after surgery, one case of nonunion in the anchor LCP group, and no cases of infections. There were no significant differences in the prevalence of postoperative ACJ arthrosis, heterotopic ossification, and synostosis between the two groups.
Subacromial osteolysis was observed in 16 (29.6%) patients in the hook LCP group, whereas peri-anchor osteolysis was observed in 4 (14.3%) patients in the anchor LCP group. Two (3.7%) cases of peri-hardware fractures were observed in the hook LCP group. Revision surgery with long locking plate osteosynthesis was performed in two patients with peri-hardware fractures, whereas one case (3.6%) showed a loss of reduction with nonunion in the anchor LCP group. Moreover, two cases (7.2%) of knot-induced irritation were observed in the anchor LCP group (Table 3).
Complications between the two groups.
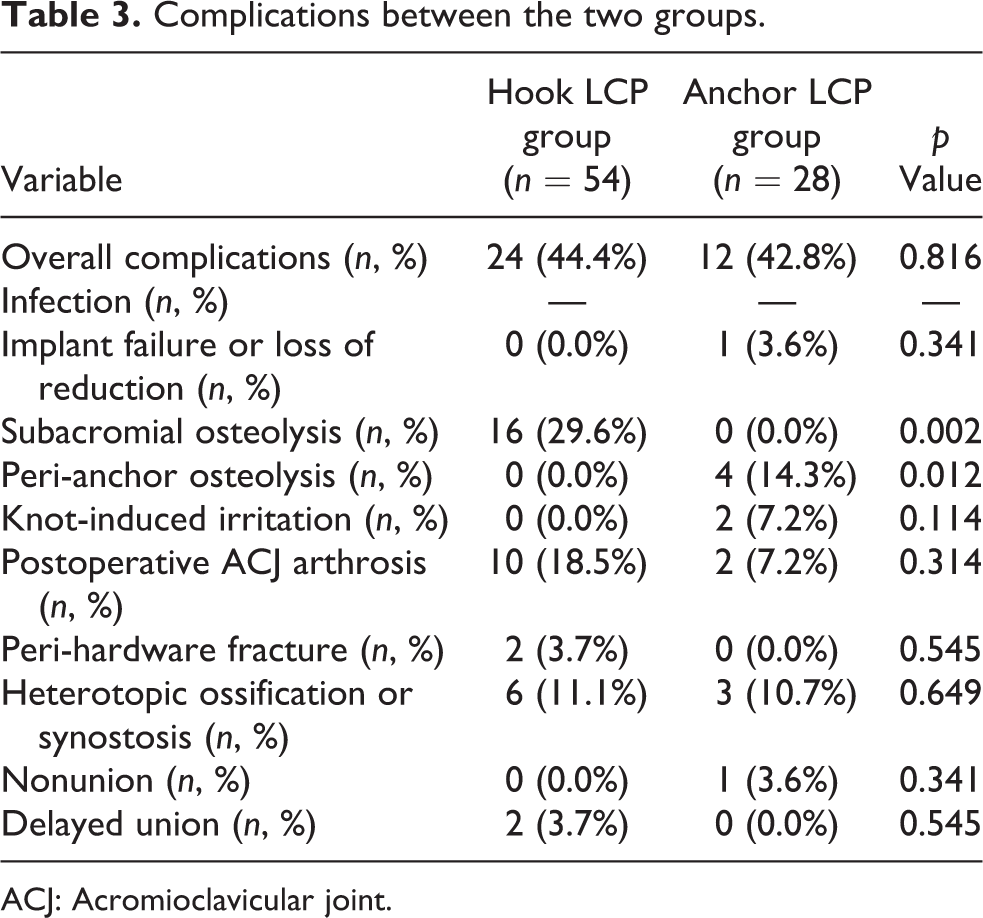
ACJ: Acromioclavicular joint.
Discussion
The primary aim of this study was to assess the clinical and radiological outcomes of LCP with all-suture anchor fixation for Neer IIb distal clavicle fractures in comparison with hook LCP fixation. Supporting our initial hypothesis, there was no difference in the union period, union rates, and CCD between the two groups. However, contrary to our hypothesis, there were no significant differences in final clinical outcomes and complication rates between groups.
There are various surgical techniques that have been previously introduced, such as K-wire fixation, tension band wiring, locking plates, and hook plates. 5,18 –21 However, there has been no consensus for the “gold standard” of fixation for unstable distal clavicle fractures. The hook plate fixation technique, originally used for acromioclavicular ligament injuries, has especially demonstrated good clinical and radiological outcomes in acute injuries by restoring the normal CCD, even without repair or augmentation of the CC ligament. 22,23 Several studies have reported that this hook plate also showed favorable outcomes when used for the fixation of unstable distal clavicle fractures. 20,24,25 However, 66 of 162 patients (40.7%) treated with hook plate fixation experienced complications in a systematic review of type II fractures. 26
In 2017, Erdle et al. 9 reported that both hook plate and LCP fixations were equally effective in relation to the restoration of vertical stability, overall functional outcomes, and fracture consolidation in the treatment of Neer IIb distal clavicle fractures. However, Shin et al. showed that locking plate osteosynthesis alone may not fully restore the CCD in Neer IIb distal clavicle fractures. 5 Shin et al. 5 recommended the insertion of more than four distal screws for the lateral fragments to achieve stability. However, it is difficult to achieve firm fixation of the lateral fragment when it is comminuted or small. Erdle et al. reported a mean number of fragments of 2.59, 9 while Lee et al. also reported a 47.7% proportion of comminuted fractures. 24
Therefore, various additional CC fixation techniques have been introduced to increase vertical stability. 14 –16 In 2013, Madsen et al. reported that CC fixation with suture anchors adds stability to type IIb distal clavicle fractures fixed with a plate and screws when loaded to failure. 16 In 2019, Xu et al. also demonstrated that both locking plates and CC suture anchors can provide more stability in the early stages after operation than can the use of locking plates alone. 14 They also recommend a locking plate combined with a suture anchor for elderly patients with comminuted Neer IIb distal clavicle fractures to provide more stability in the early stages after the operation. 14 However, iatrogenic anterior deltoid detachment from the clavicle is necessary to accurately insert the conventional suture anchor because inaccurate insertion of the suture anchor without visualization of the coracoid can induce coracoid fracture or anchor pullout. Recently, all-suture anchors have been frequently developed for shoulder surgery, and comparable pullout strength has been reported in several previous studies. 27,28 Therefore, an all-suture anchor was used to avoid iatrogenic deltoid detachment in the present study. As a result, LCP with all-suture anchor fixation showed satisfactory clinical and radiological outcomes without a loss of reduction and deltoid atrophy at 1 year after surgery.
However, contrary to our hypothesis, there were no significant differences in the complication rates between the two groups. Only the ROM at 3 months after surgery of LCP with all-suture anchor fixation was better than that of hook LCP fixation. Various hook plate-related complications are well known because the clavicular hook plate has been extensively used. 11,26,29,30 However, the incidence of hook-related complications was quite different because the definition of complications also differed in each study. 11,26,29,30 Otherwise, the complication of additional anchor fixation is not well known because previous studies on LCP with additional anchor fixation are still limited. In the present study, we evaluated and defined the complications of additional anchor fixation such as peri-anchor osteolysis and knot-induced skin irritation. Additionally, shoulder stiffness before implant removal in the hook plate fixation group was excluded from the definition of complications because all patients who had shoulder pain before implant removal recovered full ROM at the final follow-up.
The most common complication was pre-implant osteolysis (peri-anchor and subacromial osteolysis) in both groups. In biomechanical analysis, Lee et al. reported that the stress of the clavicle hook plates indicates that high stress was found in the corner of the clavicle hook plate. 31 As a result, subacromion osteolysis was an inevitable common complication of contact stress concentration of the hook. 11,20,21,29 Although there has been no study on biomechanical analysis of stress concentration at the coracoid with anchor fixation, we believe that peri-anchor osteolysis is similar to subacromial osteolysis of the hook plate according to the stress concentration at the coracoid anchor to maintain vertical stability.
Few reports have been published on peri-hardware fractures at the medial end of the plate as a rare complication of clavicular hook plates. 10,32 Lee et al. also reported that based on the stress applied to the screws in the clavicle, the most medial screw positioned at the proximal end of the clavicle results in more stress on the clavicle, regardless of differences in hook depths or plate materials. 31 In this study, two cases (3.7%) of peri-hardware fractures were detected only in the hook LCP fixation group. Although there were no cases of peri-hardware fracture in the anchor LCP group, one case of a loss of reduction with nonunion was observed in the anchor LCP group. We believe that the reason for the loss of reduction was anchor pullout from the coracoid. Moreover, two patients who underwent LCP with all-suture anchor fixations were converted to hook LCP fixation because the anchors pulled out during surgery. Therefore, LCP with all-suture anchor fixation should be carefully performed after preoperative evaluation because all patients who showed anchor failure had osteoporosis or chronic renal failure.
This study has several limitations. First, this was a nonrandomized, retrospective study. Second, only 28 patients were included in the anchor LCP group. A small sample size often leads to a type II error, although the adequacy of the present study was proven on the basis of the post hoc analysis results with a power of 80.7%. Third, CT is the gold standard for evaluating bone union. However, union was defined using only simple radiography without CT evaluation. To increase the accuracy of union assessment, cases in which the two shoulder surgeons did not agree were not defined as union. Fourth, only the ASES score, KSS, and Constant score were analyzed without ACJ-specific functional evaluations (Taft score or ACJ instability score) in this study. Fourth, all cases of the anchor LCP group were treated by one shoulder surgeon (JSY). Cases under the hook LCP group were treated by two shoulder surgeons (JBS and JSY). Therefore, the difference in surgical skills between surgeons may be a factor in this study. Fifth, two different plates were used in the hook LCP fixation group, although there was no resultant difference due to plate type. Finally, although previous studies have demonstrated that osteoporosis is a contributing factor, its effect could not be evaluated since bone matrix density analysis was not performed in all patients.
Although anchor LCP fixation showed new anchor-related complications and limitations, we believe that LCP with all-suture anchor fixation is a useful method for Neer IIb distal clavicular fractures to achieve additional vertical stability, avoiding hardware removal, hook-related complications without surgical time consumption, and iatrogenic postoperative deltoid atrophy. However, it is necessary to verify anchor security intraoperatively and patient selection after preoperative evaluation to prevent anchor pullout or loss of reduction.
Conclusion
LCP with all-suture anchor fixation showed satisfactory clinical and radiologic outcomes in comparison with hook LCP fixation. In Neer IIb distal clavicle fractures, LCP with all-suture anchor fixation is a useful method for the maintenance of reduction, avoiding implant removal, and hook-related complications. However, anchor fixation should be carefully used, especially in osteoporotic patients or patients with underlying diseases.
Footnotes
Authors’ note
JBS and JSY designed the study, KYK and JSY performed the radiological measurements, and KYK collected the retrospective data.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.