
Abstract
Introduction:
The purpose of this study was to compare the results of arthroscopically assisted reduction of acute acromioclavicular (AC) joint separations with the Tight-Rope technique with results of clavicular hook plate fixation.
Materials and Methods:
The 28 patients with acute high-grade AC joint dislocation were treated with arthroscopic assisted fixation using the Tight-Rope system, the arthroscopic evaluation and treatment of glenohumeral lesions were performed before AC ligament reconstruction. Each Tight-Rope technique group patient was matched with three controls that underwent clavicular hook plate fixation, and preoperation and postoperative visual analogue scale (VAS) and functional recovery (Constant Score) of the shoulder joint was assessed,. Furthermore, the demographics and clinical characteristics were compared between the two groups.
Results:
All patients had clinical and radiological results available at 2 years or greater (mean: 34; range: 24–72 months), they were statistically significant improvement in the constant score and VAS score at the end of follow-up respectively (P < 0.001). Compared with the clavicular hook plate group, Tight-Rope system group patients were incurred significant statistically lower skin incision, hospitalization time and estimated blood loss (P < 0.001), and the constant score and VAS score at the end of follow-up was significantly higher in the Tight-Rope group (P < 0.001). Patients who underwent clavicular hook plate had a higher incidence of fixation failure [10 cases (11.9%) versus 2 cases (7.1%)] than those of the Tight-Rope system group.
Conclusions:
The Tight-Rope technique is advantageous for treating these patients because it is a minimally invasive procedure with low complications and superior clinical outcomes.
Introduction
Traumatic injury of the acromioclavicular (AC) joint runs up to 9% of all shoulder injuries in human beings. 1 Recent epidemiological studies showed that around 60,000 new cases were diagnosed with complete dislocations (Rockwood type’s ≥ III) every year. 2 Treatment of AC joint separations remains controversial. According to the severity of AC injury, Rockwood classified the AC joint disruption into six grades, and Rockwood I and II AC joint injuries was be recommended for conservative treatment. 3 As for high-grade AC joint separations, surgical treatment was recommended. However, studiesrevealed that a large number of those patients were associated with significant residual symptoms, and the biomechanical consequences of the injury are permanent. 4 Therefore, most of the studies indicated that surgery should be recommended for patients with high demands and failure of non-surgical treatment. 5
During the past decade, growing interest has focused on the reconstruction techniques for high-grade AC joint dislocations. Long-term AC joint stability by initial fixation is strong enough to maintain the entire biological healing process. There are several methods used for fixation, like K-wires, hook plate and Tight-Rope system, without a gold standard procedure. Compared with the open surgical techniques, more evidence indicates that the all-arthroscopic approach is advantageous for patients with AC joint disruption, because the minimally invasive procedure is superior to the open surgical techniques, in terms of low complications, avoids the need for a second procedure for implant extraction, fixation failure and a loss of reduction after plate removal. 6,7
Arthroscopic assisted fixation using Tight-Rope system techniques for treating acute high-grade AC joint dislocations had been examined in a few studies but some results remained controversial. 8,9 Furthermore, the current literature lacks studies comparing different stabilizing techniques with short injury-to-surgery intervals and clinical outcome assessments. This study aims to compare the short-term efficacy of the Tight-Rope technique and clavicular hook plate technique in the treatment of acute high-grade AC joint dislocation. Also, we hypothesized the new Tight-Rope-fixation techniques lead to comparable or even better results than the previously described open AC joint repair.
Materials and methods
Patient selection
This study was approved by the medical research ethics committee of our hospital. A total of 518 patients with acute high-grade AC joint dislocation (<3 weeks 10 and Rockwood type’s III–V) received ligament reconstruction surgery between February 2015 and June 2017 were included in this study. Of these patients, 28 patients were treated with arthroscopic assisted fixation using the Tight-Rope system. To compare the treatment results between the Tight-Rope technique and clavicular hook plate fixation, each Tight-Rope technique patient was matched with 3 controls that underwent clavicular hook plate fixation at the same period based on gender, age and diagnosis.
The inclusion criteria were (1) the presence of symptomatic (<3 weeks), diagnosed based on clinical evidence, plain film and magnetic resonance imaging (MRI), and operative therapy was indicated depending on the type of AC joint dislocation according to Rockwood classification (type III, IV, V); (2) All-arthroscopic reconstruction of the AC ligaments with Tight-Rope system, and the arthroscopic evaluation and treatment of glenohumeral lesions were performed before AC ligament reconstruction; (3) clinical examination of operatively treated patients by an independent observer with radiographs performed at least 2 years after surgery (Figure 1).

A 48 years female with a painful and weak shoulder after the traffic accident trauma. (A) Preoperative radiograph showing a high-grade (Rockwood type V) AC joint dislocation. (B and C) Postoperative radiograph after treated with arthroscopic assisted fixation using Tight-Rope technique (at 2-year follow-up).
The exclusion criteria were (1) previous AC joint injuries, chronic AC joint injuries (>3 weeks after trauma), Rockwood I and II AC joint injury; (2) AC joint arthritis, and those with fractures of the distal clavicle; (3) patients presenting with concomitant pathologies that could potentially preclude accurate evaluation were excluded from this study, such as neuromuscular, rheumatic, significant psychiatric or metabolic disorders.
Data collection
The following parameters were recorded: patients’ age at diagnosis of AC joint injuries, gender, comorbidities, Rockwood type, treatment for AC joint injuries, duration from injury to the surgery, the incision length, operation time, intraoperative blood loss, hospitalization time, preoperation and postoperative visual analogue scale (VAS 10 ) of the affected shoulder, functional recovery of the shoulder joint and complications at 2-year follow-up.
Surgical techniques
Clavicular hook plate techniques
The patient was positioned in beach-chair position under general anesthesia. An approximately 8 cm long skin incision was made between the lateral clavicle and the AC joint. After clavicular reduction, the clavicular hook plate was positioned on the lateral clavicle and fixed in the clavicle with screws, and the wound closed in layers. Implant removal was performed 3 months after surgery.
Tight-Rope techniques
Arthroscopic evaluation and treatment of glenohumeral lesions were performed with the patient in the beach-chair position under general anesthesia. The antero-superior and antero-inferior portals were used to expose the base of the coracoid bone from intraarticular. An approximately 2 cm long skin incision was made on superior surface of the lateral clavicle, and then a guide pin was drilled from the clavicle to the base of coracoid under the special guide system assisted followed by insertion of a Tight-Ropes system, the AC joint was reduced under image intensifier control (Figure 2). The Tight-Rope was tightened, and the wounds were closed in layers.
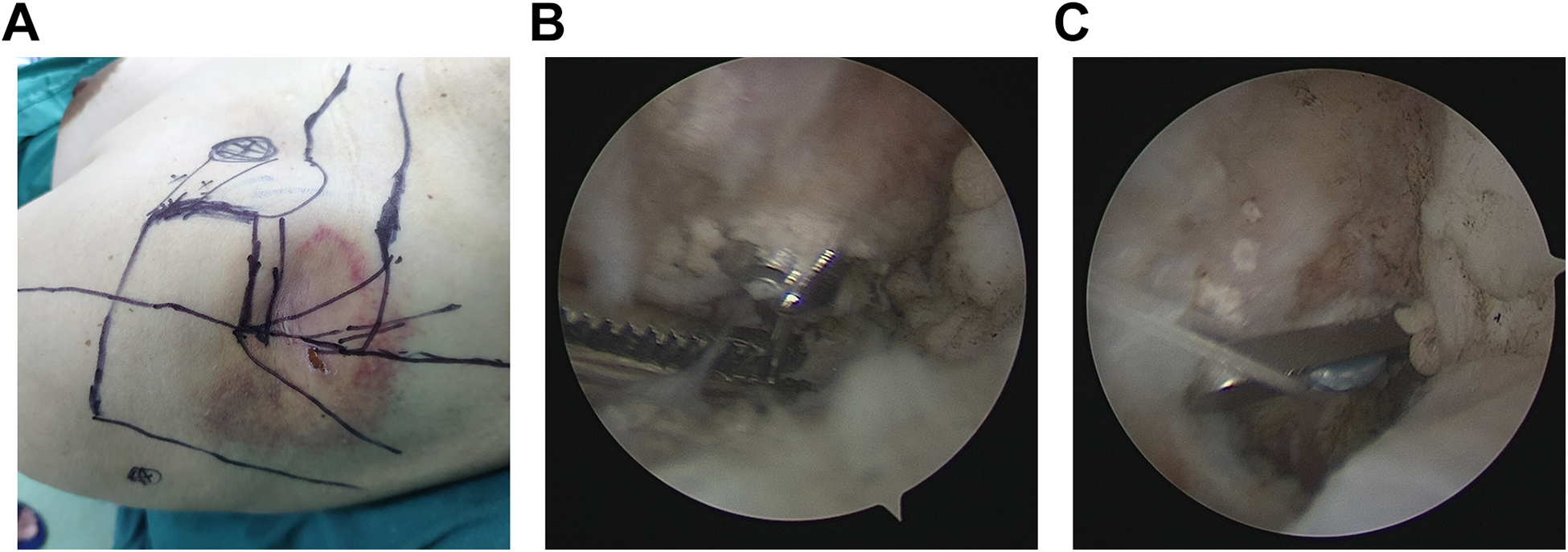
(A) Preoperative picture of the shoulder showing skin landmarks and portals. (B) Intraoperative image showing the cannulated drill came out of the under surface of the coracoid. (C) The button of the Tight-Rope flipped on the inferior surface of the coracoid process.
Postoperative management
The correct reduction and position of the clavicle were confirmed relies on plain film, all patients arm used a sling for 6 weeks, normal use of the arm for most activities of daily living was encouraged, full active motions of the shoulder were allowed after 6 weeks, no heavy strenuous activities were allowed for the first 12 weeks.
Outcome assessment
The outcome was evaluated by two orthopedics surgeons, and imaging and clinical examinations were performed at directly postoperative, 1 month, 3 months, 6 months, 12 months, and 24 months, and shoulder functional assessment was performed according to the constant score 4 and VAS score.
Statistical analysis
Quantitative variables were presented as mean value ± standard deviation (SD), and the two groups were compared using the Student’s t-test. Count variables were expressed as numbers and percentages, and were assessed by the Chi-square test. Statistical significance was set as P-value less than 0.05. All analysis was performed by IBM SPSS Version 22 (SPSS Inc. Chicago, IL, USA).
Results
Patient demographics
The patients’ demographics were demonstrated in Table 1. The 28 acute AC joint dislocation patients were treated with arthroscopic assisted fixation using the Tight-Rope system. Also, concomitant glenohumeral lesions were treated during the surgical procedure (4 cases, 14.3%). In detail, there were no significant differences in age, gender, duration from injury to the surgery, injured side, Rockwood classification, comorbidities, follow-up time and mechanism of injury among the two groups.
Patient demographics in different groups.

CH: clavicular hook plate; TR: Tight-Rope.
There were no significant differences in postoperative complications among the two groups (P > 0.05). Intraoperative and postsurgical complications, such as fracture, were not found in the Tight-Rope system group, comparing 2.4% complication in the clavicular hook plate group (superficial infection one patient and deep infection one patient). And one patient in the clavicular hook plate group with deep wound infection underwent reoperation. Patients who underwent clavicular hook plate had a higher incidence of partial loss of reduction or fixation failure [10 cases (11.9%) versus 2 cases (7.1%)] than those of the Tight-Rope system group. Revision surgery with semitendinosus autograft and Tight-Rope system have good anatomic and functional outcomes at the last follow-up.
Comparison of surgery-related factors between groups
Functional and subjective results of patients in the different groups are revealed in Table 2. All 112 patients had outcome scores available at 2 years or longer, and there was a statistically significant improvement in the constant score and VAS score at the end of follow-up, respectively (P < 0.001 for both). All the patients were regained their normal range of motion, and very satisfied with the function of their shoulder at the last follow-up.
Functional results of the study groups.

Data are reported as mean ± SD.
CH: Clavicular hook plate; TR: Tight-Rope.
a Significant improvement in the constant score and VAS score (P < 0.001 for both).
Compared with the clavicular hook plate group, patients treated with arthroscopic assisted fixation using the Tight-Rope system were subject to a smaller length of skin incision, less estimated blood loss and shorter hospital stay (P < 0.001). Compared with patients of the clavicular hook plate group, those of the Tight-Rope technique group demonstrated statistically significant improvement in the constant score and VAS score at the end of follow-up, respectively. However, There were no statistically significant differences in surgical time, preoperative constant score and VAS score between the two groups (P > 0.05, respectively).
Discussion
The most important finding of this study is that the outcome of the arthroscopically assisted fixation using the Tight-Rope system for acute AC joint dislocation patients was superior to the results, which could be achieved using the clavicular hook plate. Compared with the clavicular hook plate, the Tight-Rope technique is advantageous for treating these patients because it is a relatively simple and durable surgical technique with fewer complications. Generally, AC joint separations are caused by traffic accidents and downfall, and the traumatic injury of the AC joint runs up to 9% of all shoulder injuries in human beings. 10 Treatment of AC joint separations remains controversial, many conservative treatment patients associated with significant residual symptoms, these patients may end up seeking a surgical treatment after many weeks or months of persistent shoulder symptoms. 11 More than 150 techniques for treatment of acromioclavicular joint dislocations have been described in the literature, but no single technique has gained widespread acceptance for surgical management, due to the reported diversity of operative technique has a unique complication profile. 12,13
Many studies were recommended for the treatment of high-grade AC dislocations injuries, such as tendon grafts or suture-button configurations, because it had superior results compared with nonsurgical treatment. 14 However, recent studies confirmed the incidence of complication after reconstruction of the AC ligaments was reported to be ranged from 27% to 52%, and 20% of the patients were identified with clavicle fracture complication. 15 Tendon grafts may fail due to stretch during remodeling, and the failure of suture-button configurations associated with knot slippage or button migration. Cook et al. 16 demonstrated an early failure rate as great as 29% with AC ligament reconstruction. The two buttons are now connected with a tape for a Tight-Rope system that can be self-propelled adjust reconstruction length, which has been shown to resist higher loads. 11 All the patients had outcome scores available at 2 years or greater, the present study showed successful short-term clinical outcomes for the patients who treated with arthroscopic assisted fixation using a Tight-Rope system, with a statistically significant difference between the preoperative and postoperative constant score and VAS scores, the most patients were regained their normal range of motion, and very satisfied with the function of their shoulder at last review.
During the past decade, growing interest has focused on the reconstruction techniques for high-grade AC joint dislocations, compared with open surgical techniques, evidence indicates that the all-arthroscopic approach is advantageous for treating these patients because it is a minimally invasive procedure that allows successful reduced the risk of infection and big scar. 17,18 An arthroscopic technique using the Tight-Rope system is a minimally invasive procedure that avoids the need for a second procedure for implant extraction, and fixation failure or a loss of reduction after plate removal, this results in faster recovery and better shoulder function results. 19 In line with previous studies, compared with the clavicular hook plate group, patients treated with arthroscopic assisted fixation using the Tight-Rope system were subject to smaller length of skin incision, estimated blood loss and decreased length of hospital stay. Patients who underwent clavicular hook plate had a higher incidence of partial loss of reduction or fixation failure and infection than those of Tight-Rope system group. Furthermore, our study showed an important advantage of the arthroscopic approach for treating these patients is simultaneously achieving diagnosis and treatment of the frequently (14.3%) associated glenohumeral joint lesions.
Many studies recommend using the double Tight-Rope technique for the treatment of high-grade AC dislocations. 20,21 However, Patzer et al. 22 analyzed the clinical and radiological results of arthroscopically assisted Tight-Rope technique for high-grade AC dislocations injuries, it was found that there was no significant difference between the single and double Tight-Rope technique group. Furthermore, the previous study confirmed the constant score of shoulder after Tight-Rope technique was reported to be ranged from 86.4 to 96.3. 23,24 Referring to our study, the mean postoperative constant score was 89.3 ± 4.2 in the Tight-Rope group, and 83.3 ± 8.8 in the clavicular hook plate group, the mean post-operative VAS scale was 1.2 ± 0.6 in the Tight-Rope group, and 1.8 ± 1.1 in the clavicular hook plate group. In a retrospective data that investigated 69 patients, Gunnar et al. 10 confirmed that the arthroscopically assisted reduction of acute AC joint separations with the Tight-Rope technique advantages over the clavicular hook plate fixation. In line with previous studies, compared with patients of clavicular hook plate group, those patients of the Tight-Rope group demonstrated statistically significant improvement in the constant score and VAS score at the end of follow-up, respectively.
Several limitations were also detected in this study. First of all, our current study is a single-center study, and a relatively small number of patients were treated with arthroscopic assisted fixation using a Tight-Rope system may introduce bias into the results, further prospective study with increased sample size is required to definitely the answer the question whether the arthroscopically assisted Tight-Rope technique is superior to the open procedure or not. Second, our study is not fully showed what the outcome results would be while performing AC reconstruction alone without performing any other glenohumeral joint lesions surgery, the difference in outcomes could be related to the management of other pathology in 14.3% of patients. Third, we just observed the constant score and VAS score of the shoulder within 2 years after injury in patients with AC reconstruction, therefore, a prospective study with long-term follow-up is necessary.
The present study showed successful short-term clinical outcomes for the patients who treated with arthroscopic assisted fixation using the Tight-Rope technique, the most patients were regained their normal range of motion, and very satisfied with the function of their shoulder at the last review. Compared with the clavicular hook plate technique, the Tight-Rope technique is advantageous for treating these patients because it is a minimally invasive procedure with low complications and superior clinical outcome.
Footnotes
Author contributions
The authors made the following contributions: Min Lan made the conception for this research. Min Lan and Si Nie analyzed the data and drafted the article. Min Lan and Si Nie reviewed/ edited the manuscript. All the authors critically revised the article for important intellectual content. The author(s) read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.