
Abstract
Purpose
Hook plate fixation is one of the most frequently used methods for unstable distal clavicular fractures, but it is still unknown if there is a need for coracoclavicular (CC) reconstruction. This study aimed to compare the efficacy of hook plate fixation with versus without CC reconstruction for distal clavicular fractures.
Methods
Eighty-one patients who underwent hook plate fixation (HP group, n = 45) or hook plate fixation plus suture anchor reconstruction (HPA group, n = 36) for Neer type II or V clavicular fractures were enrolled. Demographics, fracture characteristics, and surgical data were recorded. Union time, coracoclavicular distance (CCD), post-operative complications, Constant score, and Disabilities of the Arm, Shoulder, and Hand (DASH) score were compared between HPA and HP groups.
Results
Constant score in the HPA group was higher than that in the HP group (91.8 ± 3.6 vs 88.8 ± 6.0, P = 0.007). However, there were no significant differences in union time, DASH score, CCD, and post-operative complications between the two groups (P > 0.05). Hook plate fixation combined with CC reconstruction costed more (3023.7 ± 202.6 vs 2416.2 ± 167.6 EUR, P < 0.001) and prolonged operative duration (78.2 ± 9.2 vs 73.7 ± 8.3 min, P = 0.023) compared with hook plate fixation alone.
Conclusion
Hook plate fixation with or without suture anchor reconstruction achieved satisfactory outcomes for Neer type II or V clavicular fractures. However, hook plate fixation plus CC reconstruction showed better functional outcomes compared with hook plate fixation alone.
Introduction
Clavicular fractures are common injuries of the shoulder girdle with an incidence of 30 per 100,000. 1 The rate of occurrence of distal clavicular fractures is 10%–30% in all clavicular fractures. 2 Neer types II and V clavicular fractures are displaced and unstable because of the detachment of coracoclavicular (CC) ligaments. It is difficult to achieve rigid internal fixation because distal fragments are usually small and comminuted. 3 The nonunion rate of conservative treatment is as high as 22%–50%, so surgical treatment is currently recommended. 4 Although there are many operational methods including internal fixation using hook plates, locking plates, Kirschner wires, tension band wires, and CC reconstruction, there is no gold standard of treatment. 5
Hook plate fixation is considered one of the popular internal fixation methods for distal clavicular fractures. Previous studies demonstrated that hook plate fixation could achieve good outcomes.6,7 However, hook plate fixation often causes many complications including subacromial impingement syndrome, acromial fractures, ligament injury, and implant-related irritation. 8 In addition, implant removal is needed to prevent above-mentioned complications.
CC reconstruction can maintain CC distance, facilitate the healing of CC ligaments, and enhance the vertical stability of distal clavicular fractures. CC fixation can be accomplished with CC screws, endo-button devices, tight ropes, suture anchors, suspensory sutures, ligament transfer, and so on.9,10 However, for comminuted distal clavicular fractures, it is difficult to achieve stable fixation with CC reconstruction alone.5,11
Biomechanical studies showed that the combination of plate-and-screw fixation and CC reconstruction achieved greater stability of unstable distal clavicular fractures than plate-and-screw fixation alone, suggesting the combined treatment could theoretically improve CC stability and allow early mobilization.12,13 Several studies demonstrated hook plate fixation with or without CC reconstruction achieved satisfactory clinical outcomes, and hook plate fixation plus CC reconstruction reduced complication rates for patients with acute acromioclavicular joint (ACJ) dislocations.9,14,15 In addition, a case series showed hook plate fixation plus suture anchor reconstruction yielded good functional outcomes with low complication rates for patients with Neer types Ⅱ and Ⅴ distal clavicular fractures. 16 It seemed that the above-mentioned studies supported the combined treatment. However, to our knowledge, there are no published studies comparing hook plate fixation with CC reconstruction and hook plate fixation alone in the treatment of distal clavicle fractures.
This study aimed to investigate the role of CC reconstruction in patients who underwent hook plate fixation for Neer types II and V clavicular fractures. We hypothesized that hook plate fixation plus CC reconstruction would provide better outcomes and have a lower complication rate than hook plate fixation alone.
Materials and methods
This study was approved by the Ethics Committee of our hospital and retrospectively registered in Chinese Clinical Trial Registry (registration number: ChiCTR1900027163). Informed consent was obtained from all patients. We reviewed 97 patients who received hook plate fixation for Neer types II and V distal clavicular fractures between January 2011 and May 2021. Inclusion criteria were: (1) Neer type II or V clavicular fractures, (2) fresh fractures within 3 weeks, (3) hook plate fixation with or without suture anchor reconstruction, (4) normal shoulder function before fractures, and (5) at least 1 year of follow-up. Sixteen patients were excluded for the following reasons: a history of shoulder injury (3 patients), less than 1 year of follow-up (4 patients), loss of follow-up (6 patients), and refusal to participate in the study (3 patients). Finally, this study included 36 patients who underwent hook plate fixation plus suture anchor reconstruction (HPA group) and 45 patients who underwent hook plate fixation alone (HP group). Figure 1 shows the flow chart of this study. Flow chart of this research.
Demographic parameters included age, sex, body mass index, injury severity score, fracture side, injury type, fracture pattern, time to surgery, and follow-up time. Operation-related indices included intraoperative blood loss, surgical time, operation-related cost, and hospitalization time. For clinical outcomes, we analyzed fracture healing rate, fracture union time, the Disabilities of the Arm, Shoulder, and Hand (DASH) score, Constant score, post-operative complications, and time to implant removal at the last follow-up. For radiographical outcomes, we measured the coracoclavicular distance (CCD) of the injured side at the last follow-up.
Surgical technique
All the operations were performed by six senior orthopedic surgeons with more than 10 years’ experience. Patients underwent open reduction and internal fixation (ORIF) under general anesthesia in the supine position. A 10-cm skin incision was made parallel to the clavicle, and then the deltoid-trapezius fascia was incised. The fracture was temporarily reduced using reposition forceps. The hook of the hook plate (DePuy Synthes, Raron, Switzerland) was inserted under the acromion, and fixed with locking screws after confirming the reduction of fractures via C-arm fluoroscopy. Whether we performed CC reconstruction or not was dependent on the surgeons’ preferences and personal experience. In HPA group, patients received hook plate fixation and CC reconstruction. CC ligaments were explored and identified. Then, a suture anchor (3.5-mm titanium anchor with two sutures, Smith & Nehpew, Andover, MA, USA) was fixed in the base of the coracoid process. The sutures were tied around the clavicle and the hook plate. In HP group, patients received hook plate fixation alone.
Post-operative rehabilitation
Patients were encouraged to wear sling protection for 4 weeks post-operatively. Slight pendulum movement, circumduction exercise, and passive range of motion exercise were encouraged from the first day after surgery. The shoulder abduction angle should be <90°. One month later, the intensity of physical exercise was gradually increased. About 3 months later, the patients began to engage in normal activities. The hook plates were removed when bone union and joint functional recovery were achieved.
Statistical analysis
Statistical analyses were conducted using SPSS 21.0 (IBM Corp, NY, USA). Between-group differences were compared using independent t-test, independent Mann–Whitney U test, and Pearson chi-square test. Statistical significance was defined as P < 0.05.
Results
Baseline characteristics of 81 patients.

SD standard deviation; BMI body mass index; ISS injury severity score.
aMotor vehicle accident, high-altitude injury, heavy object injury, and assault.
bFalls from standing height, and on stairs or steps.
Clinical outcomes and operation related indexes.
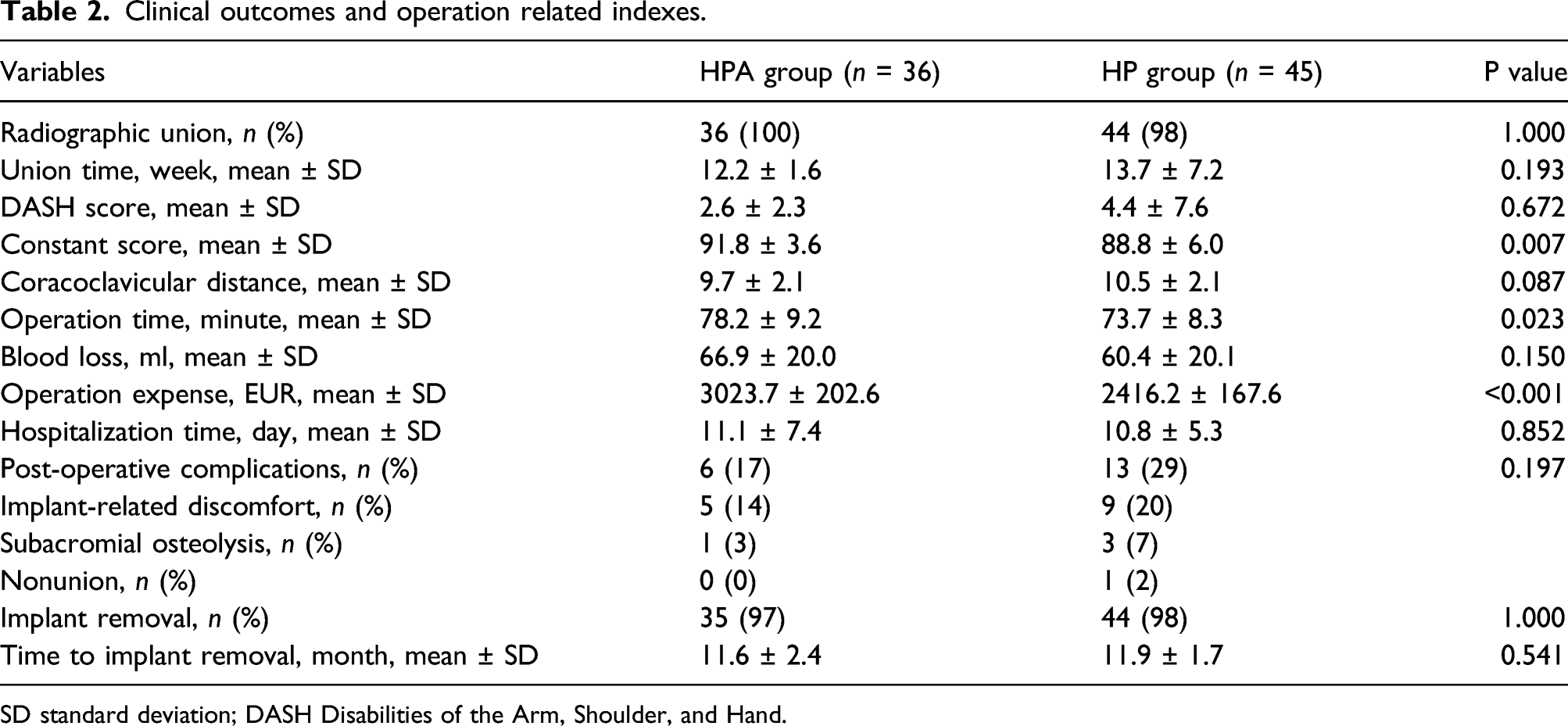
SD standard deviation; DASH Disabilities of the Arm, Shoulder, and Hand.
Constant score in HPA group was significantly higher than that in HP group (91.8 ± 3.6 vs 88.8 ± 6.0, P = 0.007), while the two groups showed no difference in DASH score (2.6 ± 2.3 vs 4.4 ± 7.6, P = 0.672). Fracture union time did not significantly differ between the two groups (P > 0.05). HPA group had a shorter CCD than HP group while no significant difference was found (9.7 ± 2.1 vs 10.5 ± 2.1 mm, P = 0.087). Figure 2 shows radiological results of typical cases. X-rays of pre-operation, post-operation, fracture union, and implant removal in HP and HPA groups. In HP group, a 35-year-old male patient had a right distal clavicle fracture treated with a hook plate. (A) Pre-operative X-ray showed a right Neer type Ⅱb distal clavicle fracture. (B) Post-operative X-ray showed good reduction. (C) X-ray at 13 weeks post-operatively showed fracture union. (D) X-ray showed implant removal. In HPA group, a 42-year-old male patient had a right distal clavicle fracture treated with a hook plate and suture anchor reconstruction. (E) Pre-operative X-ray showed a right Neer type Ⅱb distal clavicle fracture. (F) Post-operative X-ray showed good reduction, and suture anchor was fixed in the coracoid process. (G) X-ray at 10 weeks post-operatively showed fracture union. (H) X-ray showed implant removal, and the suture anchor remained in the body.
The HPA group had fewer complications than the HP group while the difference was not significant (17% vs 29%, P = 0.197). All patients in HPA group achieved radiographic union. One patient in HP group suffered nonunion, and then achieved fracture healing after a reoperation. Five cases in HPA group and nine cases in HP group suffered implant-related discomfort, and the symptom improved after implant removal. One patient had subacromial osteolysis in HPA group, while three had subacromial osteolysis in HP group.
Discussion
This is the first study to compare the clinical and radiographical outcomes between hook plate fixation plus CC reconstruction and hook plate fixation alone for unstable distal clavicle fractures. Both methods achieved satisfactory outcomes at the last follow-up, whereas the combined treatment provided significantly higher Constant score than hook plate alone despite similar DASH score. HPA group showed less union time, shorter CCD, and a lower complication rate compared with HP group, while the between-group differences were not significantly different. However, the combined method costed more and prolonged operative duration compared with hook plate fixation only.
The CC ligament connects the acromial extremity of the clavicle and the coracoid process of the scapula, and maintains the vertical stability of the acromioclavicular joint. In Neer type II or V distal clavicular fractures, distal fragments can be displaced caudally by the deadweight of the upper extremity, the pectoralis muscles, and the latissimus dorsi. 17 Contrarily, the proximal fragments can be pulled superiorly by the trapezius and sternocleidomastoid muscles.17,18 As a result, Neer type II or V distal clavicular fractures are unstable and displaced, and are associated with high nonunion rates. Previous studies showed surgical treatment reduced the complication rates of distal clavicle fractures.19,20 A multi-center, prospective, randomized controlled trial demonstrated surgical treatment provided more satisfactory outcomes for displaced distal clavicular fractures than non-operative treatment within 6 months after operation. 21 Therefore, ORIF such as hook plate fixation, locking plate fixation, K-wires, and CC reconstruction has been commonly used to treat distal clavicular fractures. 22
Hook plate fixation is an easy and reliable technique for unstable distal clavicular fractures. With the leverage spread across the ACJ, the hook of the hook plate can reduce the stress on the fracture site and help maintain fracture reduction. 23 The hook plate can recreate the biomechanics of the ACJ and firmly fix the small fragments of distal clavicular fractures. 11 However, the subacromial hook frequently involves the subacromial joint and often causes some complications including acromion osteolysis, shoulder impingement, and rotator cuff injuries. 24 An autopsy study found the hook tail significantly reduced the subacromial space, and impingement between the humeral head and the lateral hook easily occurred during the movement of the shoulder joint. 25
Erdle et al. suggested CC instability might increase the risk of hook plate-specific complications. 26 The suture anchor is a kind of miniature internal fixation that is used to connect tendons, ligaments, and bones. It is simple to operate and can effectively reconstruct CC ligaments; thus, it has been considered to treat distal clavicular fractures.27–29 Suture anchor fixation can resist the upward pull at the proximal end of fractures, and enhance the vertical stability of clavicular fracture fragments and hook plates. Therefore, we speculate that suture anchors can lower the risk of implant-related complications by limiting the movement of the subacromial hook and increasing CC stability.
Comparative studies examining hook plate fixation with or without coracoclavicular reconstruction for acute acromioclavicular dislocations.

VAS, visual analog scale; ASES, the American Shoulder and Elbow Surgeons; UCLA, the University of California at Los Angeles; CCD, coracoclavicular distance; ACJ, acromioclavicular joint; HP, hook plate; N/A, not applicable
aThe height in percentage compared to the contralateral shoulder between the upper border of the coracoid process and the inferior cortex of the clavicle.
bSevere subacromial osteolysis (depression >2 mm or cut-out of acromion).
cRelative coracoclavicular distance was defined as the ratio of the absolute coracoclavicular distance to the absolute acromiocoracoid distance.
*P < 0.05; ***P < 0.001 (compared with hook plate alone).
In this study, HPA group showed lower incidence of subacromial erosion and implant-related discomfort while there was no statistical difference in the complication rate between the two groups. The incidence of subacromial osteolysis was 6.8%–25%,6,11,18 and the incidence of implant-related irritation was 6.5%–84% after hook plate fixation among patients with distal clavicular fractures.4,23,31 Some studies demonstrated that the combined treatment of hook plates and CC reconstruction offered good outcomes and reduced the complication rate of hook plate fixation in the treatment of acute ACJ dislocations.9,14,15,30 The incidence of subacromial osteolysis was 40.4%–58.0% after hook plate fixation alone, and was 15.8%–43.8% after combined fixation (Table 3).9,14,15,30 Seo et al. found that the direct repair of CC ligaments could help maintain reduction of the CC joint, 30 suggesting that CC reconstruction might reduce the stress on the acromion.
Comparative studies examining internal fixation with or without coracoclavicular reconstruction for unstable distal clavicle fractures.

DASH, Disabilities of the Arm, Shoulder, and Hand; CCD, coracoclavicular distance; N/A, not applicable; LP, locking plate; CC, coracoclavicular; HP, hook plate.
aPercentage deviation of coracoclavicular distance of injured side compared to healthy side.
*P < 0.05, **P < 0.01 (significant between-group differences).
This study had a few limitations. First, CC reconstruction increased trauma, cost more, prolonged operative time, and caused some complications including loss of reduction, coracoid fractures, and brachial plexus injuries. 33 Second, this was a single-center retrospective control study with a small sample size. Third, short-term results were not available as we did not evaluate functional and radiographical outcomes within one year after operation.
Conclusions
Hook plate fixation with or without CC reconstruction provided satisfactory outcomes for Neer type II or V distal clavicular fractures. However, hook plate fixation with suture anchor reconstruction had better functional outcomes than hook plate fixation alone.
Footnotes
Acknowledgements
Not applicable.
Authors’ contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by Shuang Wu, Jialei Chen, Jie Zhang, and Sujan Shakya. The first draft of the manuscript was written by Shuang Wu and Jialei Chen. Zhou Xiang, Fei Xing, and Jiachen Sun critically revised the manuscript. All authors commented on previous versions of the manuscript. All authors read and approved the final manuscript. The study was supervised by Zhou Xiang.
Authorship declaration
All authors listed meet the authorship criteria according to the latest guidelines of the International Committee of Medical Journal Editors. All authors are in agreement with the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Our study was funded by National Natural Science Foundation of China (Grant number 31870961), Science & Technology Department of Sichuan Province (Grant number 2020YFS0140), and Clinical Research Incubation project of West China Hospital of Sichuan University (Grant number 2019HXFH041).
Ethics approval
This retrospective study involving human participants was in accordance with the ethical standards of the institutional and national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. The Human Investigation Committee (IRB) of West China Hospital of Sichuan University approved this study.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Data,materials and/or code availability
The original data of this study are available from the corresponding author for reasonable request.