
Abstract
Purpose:
Fillet flap is a “spare part” concept. This technique allows the defect to be covered without donor site morbidity. Over the past 5 years, there were 107 diabetic foot cases of one-toe fillet flap in our hospital. After the operation, in some patients, there was necrosis of the adjacent toe that required additional amputation. The aim of our study was to determine the cause of necrosis of the adjacent toe after fillet flap.
Methods:
The patients were divided into two groups. One group had no necrosis of the adjacent toe (group A) after the operation, and the other group had necrosis of the adjacent toe that required additional amputation after the operation (group B). Then, to confirm the cause of the additional necrosis of the adjacent toe, χ 2 tests, Fisher’s tests, and logistic regression tests were performed.
Results:
A total of 107 patients were included, and 48 patients needed additional amputation. The logistic regression test revealed that a fillet flap at the metatarsophalangeal joint (MTPJ), horizontal sutures, and a fillet flap at the second toe were significant risk factors for developing necrosis.
Conclusions:
If a fillet flap with a second toe, fillet flap on MTPJ level and horizontal closure after fillet flap is needed, the chance of developing necrosis of the adjacent toe and additional revisional surgery must be communicated preoperatively.
Introduction
Diabetic foot ulcers were defined as any breakdown of the patient’s foot. These foot ulcers are common in patients with diabetes and easily lead to amputation of the patient’s leg. Currently, the incidence of diabetes is expected to rise, and the incidence of diabetic foot ulcer is elevated. 1 The incidence of diabetic foot ulcers in diabetes is 4–10%, and 5% of patients with diabetes are anticipated to have a history of foot ulceration. 2 As the risk of diabetic foot ulcers is high, the incidence of diabetic foot ulcers may increase in the future. 3
Diabetic foot ulcers are a common complication of diabetes and are caused by various factors, such as poor glucose control, diabetic neuropathy, peripheral vascular disease, structural deformity, 4 and reduced pedal soft tissue thickness. 5 In addition, patient lifestyle also affects the development of foot ulcers. These various factors cause foot ulcers in patients with diabetes, and the development of foot ulcers is a complicated process. Therefore, hospitalized patients with diabetic foot ulcers need a multidisciplinary approach determined by a team composed of doctors from endocrinology, vascular surgery, orthopedics, physiatry, and so on.
The treatment of diabetic foot ulcers includes tight glucose control, physical therapy, dressing with specific materials, and surgical therapy. If the patient’s wound is not severe and the circulation is intact, then conservative treatment, such as foam dressing, can be performed. However, if necrosis, infection, or gangrene is found in the patient’s foot, then surgical debridement is needed. After wound preparation, surgery is needed to cover the wound. The surgical options include skin graft, local flap, and free flap.
Recently, most surgeons have chosen a free flap to cover the wound. 6,7 However, if patient’s condition, including comorbidity, economical status, and other factors, was not adequate with free flap surgery, our department was to choose a local flap, such as a fillet flap firstly. A fillet flap is a “spare part” concept, which allows the defect to be covered without donor site morbidity. 8 The advantage of fillet flaps is simple and the ability to avoid the risks of microsurgery if the patient has peripheral vascular diseases or comorbidities. 9 For diabetics with many cormorbidities, simple surgery and short duration of treatment is better. When necrosis of only one toe is fully demarcated, the fillet flap is frequently applied. However, after the surgery, we frequently encountered necrosis on the side of the toe. The new complication like necrosis of side toe needed a longer time for diabetic foot ulcer treatment and more surgery. Therefore, in this article, we review our 107 cases of fillet flaps over the course of 5 years to find the cause of necrosis on the side of the toe (Figure 1).

(a) Preoperative clinical photo of 65 years old female diabetic foot patient with second toe necrosis. (b) Immediate postoperative clinical photo after second toe fillet flap on metatarsophalangeal joint. (c) Postoperative day (POD) 3 days, new ulceration on the third toe was occurred. (d) POD 5 days, the third toe ulceration was aggravated. (e) POD 8 days, full layer necrosis with yellow eschar formation was founded on the third toe medial side. Additional third toe fillet flap was performed on POD 10 days.
Materials and methods
Brief treatment protocol of diabetic foot ulcer in our institute
The patients’ chief complaints were color change in the toe, pain, or wounds on the foot. Patients often visited plastic surgery outpatient clinics or endocrinology offices first. If more treatment was needed, then the patient was admitted to our institute. After admission, various departments participated in developing the patient’s treatment, including doctors from vascular surgery, endocrinology, plastic surgery, radiology, nuclear medicine, orthopedics, and so on. The first step of the treatment process was vascular surgery and endocrinology. Endocrinologists tightly controlled the blood glucose levels during admission and educated the patients on healthy lifestyles after discharge. Vascular surgeons assessed the status of the patient’s vessels with the ankle–brachial index (ABI), digital artery test, and, if needed, angiography. After the assessment, vascular intervention or bypass surgery was performed. In addition, MRI and three-dimensional bone scans were performed to check for the presence of osteomyelitis or abscesses, the extent of the wound. Then, if the foot vessels fully recovered and the patients’ condition, including blood glucose level, was stable, surgical treatment was started with plastic surgery or orthopedics. The orthopedic surgeons treated bony deformities, such as Charcot joints, and so on, and plastic surgeons controlled the soft tissue of the foot with flap or graft surgery. After surgery, postoperative management was started by each department.
Patient selection and ethics
Before the study was conducted, the experimental plan was approved by the institutional review board of our medical center. The informed consent of clinical photo in this article was provided. This study was performed retrospectively, and patients who underwent a fillet flap primarily by a single surgeon due to necrosis in only one toe over the course of 5 years (from 2015 to 2019) were included in our study. Patient information was obtained through electronic medical records, and patients with incomplete medical records were excluded. In addition, we exclude patients who had infections, had a previous history of toe amputation, had osteomyelitis confirmed by magnetic resonance imaging (MRI), and had foot deformities. The foot deformities were confirmed using X-ray and clinical photography by a single surgeon. We obtained the following: patient age; duration of diabetes; necrosis site; preoperative ABI; previous history of illness, including hypertension, chronic kidney disease, and cardiovascular disease; amputation level; and suture direction.
Hypothesis of our study
Over a period of 5 years, we successfully performed the fillet flap operation for patients with necrosis of one toe, and in our study, we retrospectively review all of these cases. However, we found necrosis in the adjacent toe after a fillet flap; for example, after we treated necrosis in the fifth toe, the fourth toe became necrotic. We eventually realized that most of the necrosis in the adjacent toes empirically occurred at the metatarsophalangeal joint (MTPJ) amputation. Therefore, we hypothesize that MTPJ amputation causes necrosis in the adjacent toe and retrospectively studied this hypothesis by this procedure with distal amputation. In addition, using medical records, we attempted to identify other risk factors for necrosis in the adjacent toe after a fillet flap.
Study sequence and statistical analysis
We divided the patients into two groups: one group had no necrosis in the adjacent toe (group A) after the operation, and the other group had necrosis in the adjacent toe that required additional amputation after the operation (group B). The statistical analysis is as follows:
χ
2 tests and Fisher’s tests were performed to compare the differences in distribution between the two groups (groups A and B). Logistic regression tests were performed to compare the risk factors of group B with those of group A. The last study was confirmed whether a specific vessel affected the development of necrosis in the adjacent toe. The sequence described as follows: If the flow in the distal toe was not patent, some patients underwent angiography. In angiography, five vessels (superficial femoral artery, popliteal artery, anterior tibial artery, posterior tibial artery, and peroneal artery) were examined. We classified the vessel status into five grades. Then, we divided the vessel status grades into two groups. Grades 0–2 were combined and called “good,” and grades 3–5 were combined and called “bad” (Table 1). The rating was graded by vascular surgeons in our hospital. After the vessel status of the patient was classified, a logistic regression test was performed to assess whether the “bad” status of a vessel specifically affected developing toe necrosis.
Grading the vessel status with angiography.

Results
The results from “Study sequence and statistical analysis” section are described as follows: The patient demographics and differences in distribution are described in Table 2. As given in Table 2, 107 patients were enrolled, the mean age was 68.72 ± 12.12 years, the mean duration of diabetes was 17.3 ± 10.72 years, and the mean ABI was 0.8 ± 0.43; the number of patients with each condition, including hypertension, chronic kidney disease, and so on, is also described (Table 2). The χ
2 test and Fisher’s test (Table 2) revealed that there were statistically significant differences in the amputation level and amputation site between the two groups (p < 0.05). The logistic regression test revealed that the amputation at the MTPJ had a statistically significant risk of causing necrosis in the adjacent toe compared with amputation at the proximal or distal interphalangeal joints (PIPJ and DIP, respectively) (p < 0.01). The fillet flaps at the MTPJ carry 131.6 times more risk than fillet flaps at the DIP or PIPJ. Amputation of the second toe had a significantly higher risk than amputations of other toes (p < 0.05). Interestingly, horizontal sutures had 6.7 times higher risk of causing necrosis in the adjacent toe than vertical sutures, which was statistically significant. None of the variables had a statistically significant risk of causing necrosis in the adjacent toe (Table 3 and Figure 2). A total of 54 patients underwent angioplasty. After dividing the patients into two groups (“good” and “bad” groups), the logistic regression test revealed that none of the vessels had a statistically significant risk of causing necrosis in the adjacent toe (p > 0.05, Table 4).
Patient demographics.

HTN: hypertension; CKD: chronic kidney disease; CVD: cardiovascular disease; MTPJ: metatarsophalangeal joint; DIP and PIPJ: distal and proximal interphalangeal joint.
a χ 2 test and Fisher’s test.
Logistic regression test to confirm the risk of developing necrosis of the adjacent toe.

ABI: ankle–brachial index; MTPJ: metatarsophalangeal joint.

(a) Horizontal suture direction after the fillet flap. (b) Vertical suture direction after the fillet flap.
Logistic regression test for developing necrosis of the adjacent toe based on the lower extremity vessel status.

SFA: Superficial femoral artery; ATA: Anterior tibial artery; PA: Peroneal artery; PTA: Posterior tibial artery.
Discussion
The foot is an important and essential structure of the human body. Sensitive changes to the gait and motion of the foot facilitate smooth walking. In patients with diabetic foot ulcers, the foot ulcer itself is the main cause of amputation. 10 During amputation surgery, the remaining toe length is an important factor, especially in the great toe. After a great toe amputation, foot deformities and foot ulcers can arise and increase the pressure on the foot. 11,12 The resulting environment allows diabetic foot ulcers to recur more easily. Therefore, even if an amputation surgery is needed, the remaining toe length is very important.
Diabetes is a disease that requires steady and constant care. We have treated diabetic foot patients for a long time and have found that treating diabetic patients requires something special. Although medical treatment is important, the rapport between the doctor and the patient is also very important. Patients with diabetic complications have many conditions that require treatment. The disease itself is difficult to cure, but patients with chronic complications have poor awareness and require long-term treatments; however, compliance with the treatment is difficult to maintain.
In this article, the study only showed the fillet flap of one toe, but recently, we treated an extensive diabetic foot with a fillet flap. Although difficulties exist in treating the diabetic foot, the treatment method was successful, and the patient was satisfied (Figures 3 and 4). At first, we choose the fillet flap instead of microsurgery because the patient had many comorbidities. As described above, diabetes is a chronic disease that eventually leads to complications, such as diabetic retinopathy and diabetic nephropathy. Microsurgery requires a long operation time and anesthesia and thus poses a high risk to patients with many comorbidities. Therefore, we choose a fillet flap or local flap procedure instead of microsurgery, if possible.
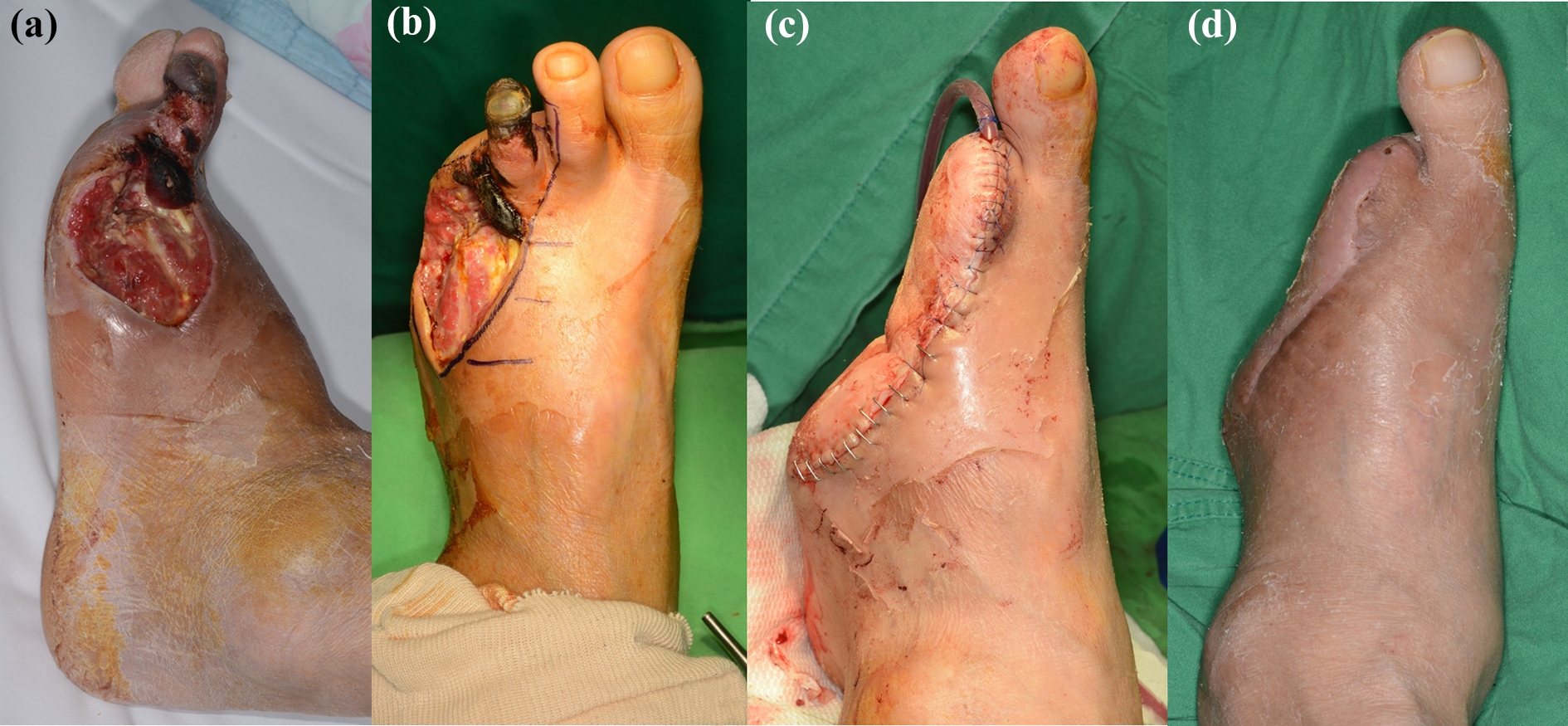
The 54-year-old male diabetic foot patient with necrosis and defect on the left foot. Patient was kidney transplant status and had many comorbidities like cardiovascular disease, dementia, hypertension, and so on. The patient refuses complicated surgery like a free flap. Therefore, fillet flap was done. (a, b) Preoperative photo and design. (c) Immediate postoperative clinical photo. (d) Clinical photo on postoperative 3 months. The patient ambulated without any other complaints and recurrence.

(a–c) The 43-year-old male diabetic foot patient with defect on fourth webspace. Fillet flap with fifth toe euthanizing was done and covered the defect. After 6 months, the patient ambulated without any other complaints and recurrence.
Necrosis of the adjacent toe was our main issue with the fillet flap. Because patients with toe necrosis patient may also have peripheral vascular disease, additional amputation is needed if necrosis of the adjacent toe occurs, which is disaster for patients who already lost one toe. We empirically confirmed that the necrosis of the adjacent toe easily occurred after proximal amputation at the MTPJ, which we then investigated in this study. We believe that there are two reasons for necrosis of the adjacent toe. One is tension, and the other is pedicle damage.
First, regarding tension, in a fillet flap at the MTPJ, more tension is applied to the side wall of the adjacent toe and because diabetic foot patients are highly likely to have peripheral vascular disease, an ulcer eventually forms the adjacent toe (Figure 5). The fillet flap at the MTPJ had a high risk of causing necrosis of the adjacent toe and has 131.6 times higher risk than the fillet flap at the DIP and PIPJ, which may be due to the tension and subsequent local vascular insufficiency.

(a) The 78-year-old male diabetic foot patient with third toe necrosis. After fillet flap closure, yellow circle area had a high tension. After 2 weeks, patient needed additional second toe fillet flap. (b) The 88-year-old female diabetic foot patient with fourth toe necrosis. After fillet flap closure, yellow circle area had a high tension. After 3 weeks, patient needed additional third toe fillet flap.
The second reason is pedicle damage. Interestingly, our results showed that horizontal sutures showed a higher risk of causing necrosis of the adjacent toe than vertical sutures. Horizontal sutures had 6.7 times higher risk than vertical sutures. The surgeon usually places horizontally sutures, and vertical sutures are only placed if there are redundant skin flaps. Therefore, in other words, vertical sutures do not require dissection around the suture site since there is already tension at the suture site; however, horizontal sutures usually need dissection around the suture site due to the lack of tension of the suture site. Between the toes, there are common digital arteries. Dissection around the suture site has a high risk of causing common digital artery damage. Therefore, there is a high possibility that diabetic foot patients have peripheral vascular disease. If damage to the common digital artery occurs, the possibility of necrosis of the adjacent toe increases. We believe that our hypothesis is logical (Figure 6).
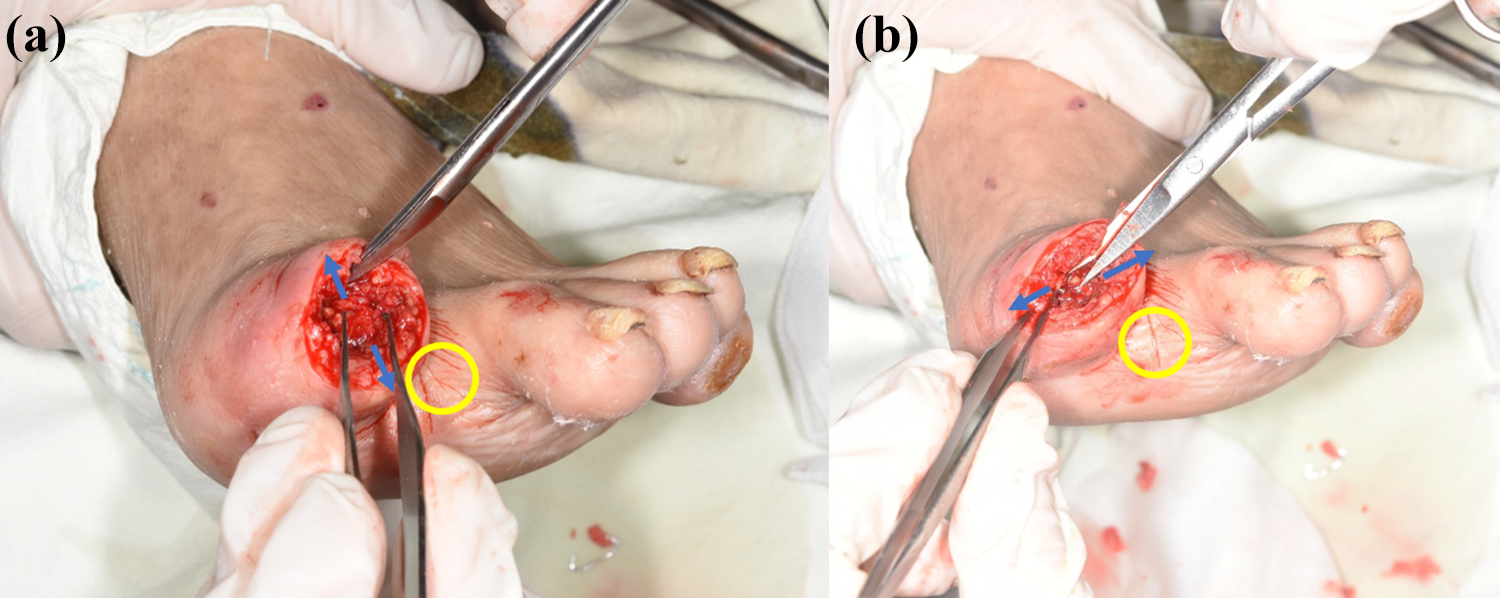
(a, b) After proximal phalanx was disarticulated, dissection toward all directions (arrow) was needed to cover the remained bone. During flap dissecting, common digital artery can be damaged if dissection was continued until the yellow circle area. If common digital artery pedicle was damaged, the adjacent toe was affected by vascular insufficiency.
In addition, there is a higher statistically significant risk of developing necrosis of the adjacent toe with a fillet flap for the second toe than with fillet flaps to other toes; the reason behind this result has not yet been confirmed completely. However, because the second toe or first interspace was the junction between the medial plantar and lateral plantar angiosomes, second toe fillet flap or dissection around the first interspace may occur the damage of mixed angiosomes, it caused side toe necrosis after fillet flap. However, this hypothesis needed additional preoperative and postoperative lower extremity angiography. It may need further investigation.
Our study is the first study about the risk factor of the adjacent toe necrosis after the fillet flap. Especially, it is the first report that there is a higher risk of adjacent toe necrosis after second toe fillet flap or horizontal suture. We think that more additional study was needed. However, there are several other limitations in our study. This study had a small sample size and was a retrospective study; therefore, our study depended on electronic medical records and the patient’s clinical images. We could not consider other variables apart from those described in the study. In diabetes, the patients have various complications, however, we could not consider another complication, for example, foot deformity or diabetic neuropathy, except the adjacent toe necrosis. In addition, vascular problems, which are the most important cause of foot necrosis in diabetes, were not fully excluded. However, according to our treatment algorithm, all of the patients were treated after distal vascular flow was established. Therefore, we believe that this point counters the limitation that vascular problems were not fully excluded. Necrosis of the adjacent toe occurred in diabetic foot patients who had previously undergone fillet flaps; further studies are needed to prevent and confirm the cause of necrosis of the adjacent toe. Finally, we already know that angiography was the most effective test for checking vascular status. However, because we could not perform angiography in all of the patients, we replace the ABI for checking vascular status instead of angiography in our study.
Conclusions
In conclusion, if a fillet flap with a second toe, fillet flap on MTPJ level, and horizontal closure after fillet flap are needed, the chance of developing necrosis of the adjacent toe and additional revisional surgery must be communicated preoperatively.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.