
Abstract
Background:
Diabetic foot ulcers and lower extremity amputations are common complications of diabetes mellitus that are associated with substantial morbidity, loss of quality of life, disability, and a high social and economic burden. The implementation of strategies to prevent these complications is a key aspect of diabetes care.
Objectives:
The objective of this article is to provide an overview of the available evidence on preventive diabetic foot care.
Study design:
Literature review.
Methods:
Narrative review based on a thorough search of previous relevant studies, systematic reviews, and clinical guidelines on diabetic foot care published in English.
Results:
We describe diabetic foot care strategies that can be categorized within defined domains for the purpose of helping clinicians to remember them. We use the mnemonic “BE SMART” (Be aware of the risk factors, Educate patients and health providers, Structured clinical assessment, Metabolic evaluation and management, Assessment of Risk, and Team care) to organize these domains.
Conclusion:
Diabetic foot ulcers and lower extremity amputations are potentially preventable complications. Clinicians taking care of patients with diabetes should know, understand, and remember the multiple aspects of diabetic foot care.
Clinical relevance
This review can be used as a reference source for those interested in the care of diabetic foot. It highlights the importance of risk factor recognition, education, a structured clinical and metabolic evaluation, and also the importance of assigning patients a risk category that can help guiding multidisciplinary management efforts.
Background
It has been estimated that the lifetime risk of developing foot ulcers in people with diabetes mellitus could be as high as 25%. 1 Community-based studies in North America and European countries have found that the annual incidence of diabetic foot ulcers (DFU) ranges from 0.6% to 2.2%.2,3 In the United States, the incidence rates are probably higher in ethnic minority groups, particularly Hispanics and African Americans. 2 The incidence of DFU is also higher in patients with known diabetic peripheral neuropathy (PN). In a large British study, Abbott et al. 4 found a 7% annual incidence of first foot ulcers among patients with diabetes and established neuropathy. DFU are associated with substantial morbidity, loss of quality of life, disability, and a high social and economic burden. 2 Foot ulcers frequently require prolonged treatments and are the source of serious infections, hospitalizations and amputation of feet and legs. Limb amputations are the most dreadful complication of DFU and may be associated with mortality rates at 5 years of up to 80%. 1 Epidemiological data indicates that diabetes accounts for the majority of non-traumatic lower extremity amputations (LEA) in most parts of the world, and that these amputations are precipitated by foot ulcers in over 75% of cases.2,5–7 Diabetic foot complications impose large costs to the society and individual patients. Ragnarson Tennvall and Apelqvist 8 calculated that the direct costs for healing infected ulcers not requiring amputation is approximately US$17,500 (in 1998), whereas the costs for LEA may range from US$30,000 to US$33,500. These costs might explain 20% of the total expenditure on diabetes in North America and Europe. 2
DFU are largely preventable complications, therefore it is important to establish foot care programs aiming to identify those at risk and to implement effective preventive strategies. Different societies and organizations, including the American Diabetes Association (ADA),9,10 the American Association of Clinical Endocrinologists (AACE), 10 the International Working Group on Diabetic Foot (IWGDF), 11 and the American College of Foot and Ankle Surgeons, 12 have published guidelines for the prevention and treatment of diabetic foot complications. Key components of these guidelines are the importance of patient and provider education, awareness of high-risk status for ulceration, the delivery of optimal preventive foot care and targeted therapeutic interventions for high-risk individuals, and the importance of following a multidisciplinary management strategy. In this review, we describe diabetic foot care strategies that can be categorized within defined domains for the purpose of helping clinicians to remember them. We use the mnemonic “BE SMART” (Be aware of the risk factors, Educate patients and health providers, Structured clinical assessment, Metabolic evaluation and management, Assessment of Risk, and Team care) to organize these domains.
Be aware of the risk factors
Diabetic foot ulceration is a multifactorial process that results from complex interactions of several etiologic factors that act synergistically to cause tissue breakdown. Diabetic PN, foot deformities, abnormal foot pressures, minor trauma, peripheral arterial disease (PAD), previous foot ulceration, and history of LEA are key risk factors for the development of foot ulcers.12–15 It is important to recognize that the presence of most of these risk factors can be easily identified by a careful history and physical examination. In a systematic review that looked at cohort studies assessing the predictive value of symptoms, signs, and diagnostic tests, Crawford et al. 14 found that duration of diabetes, history of foot ulceration, lack of protective sensation examined by a 5.07 monofilament, higher vibration perception threshold (VPT), and higher peak plantar pressures using different dynamic measuring systems, all significantly increased the risk of ulceration. In a more recently published systematic review that included 71 studies evaluating the association between more than 100 independent variables and diabetic foot ulceration, Monteiro-Soares et al. 15 found that longer diabetes duration, higher hemoglobin A1c values, diabetic PN diagnosed by various methods, higher peak plantar pressures, abnormal foot shape, rigid toe deformity, PAD, retinopathy, poor visual acuity, and previous foot ulceration or amputation were the most consistent predictive risk factors.
Diabetic PN
Diabetic PN plays a central role in the pathogenesis of foot ulcers by decreasing pain sensation and causing intrinsic muscular atrophy that leads to foot deformities and abnormal biomechanical loading.16 –19 Distal symmetric sensorimotor polyneuropathy is the most common form of diabetic neuropathy and has been estimated to occur in about 30% to 50% of patients with diabetes.20–22 The estimates of neuropathy prevalence are likely affected by the criteria and methods used to define it, but consistently appear to increase with age, longer duration of diabetes, and poor quality of metabolic control.21,22 Once loss of protective sensation (LOPS) develops as a consequence of sensory neuropathy, patients become vulnerable to suffer mechanical or thermal injuries without noticing it and thus increase their risk of foot ulceration. 1 Several methods to evaluate for sensory neuropathy are available to the clinician (e.g., light pressure assessment with the Semmes-Weinstein 5.07 (10-g) monofilament) and have been used in multiple observational studies to support the association of LOPS and increased risk of ulceration.10,14,15 Motor nerve damage is another mechanism through which distal symmetric sensorimotor polyneuropathy is associated with foot injuries. Motor neuropathy causes progressive atrophy of the intrinsic muscles of the foot leading to deformities such as hammer toes and prominent plantar metatarsal heads. These foot structural changes contribute to the development of abnormal areas of high pressure, repetitive trauma, tissue damage, and eventually skin breakdown and ulcer formation.12,17,18 Highlighting the effect of motor neuropathy, one study showed that foot muscle atrophy may occur relatively early in the course of the disease and before other clinical manifestations of neuropathy. 23 Autonomic neuropathy can also play a role in foot ulceration by causing hypohidrosis and dry skin that can easily crack and fissure. 12 Furthermore, autonomic neuropathy has been associated with functional abnormalities of the microcirculation and thermoregulatory capacity that potentially may impair tissue perfusion and microvascular responses to injury and thus increase the risk of ulceration.12,24
Deformities and limited joint mobility
Foot deformities and limited joint mobility of the ankle and foot make the foot susceptible to abnormal areas of concentrated high pressures, restrict the foot’s ability to absorb shock, and increase the risk of ulceration.25–27 Monteiro-Soares et al. 15 identified several observational studies where abnormal foot shape, rigid toe deformity, reduced first metatarsophalangeal joint mobility, and limited subtalar joint mobility were significantly associated with the development of DFU. Common deformities in patients with diabetes include hammer toes, claw toes, prominent metatarsal heads, and hallux valgus.1,12 These deformities make the plantar metatarsal heads and dorsal aspect of the toes vulnerable to excessive pressures and repetitive trauma. In patients with Charcot arthropathy or prior partial foot amputations the biomechanics of the foot is more severely affected, and therefore, these patients have a greater risk of new ulceration as well as recurrent and recalcitrant ulcers. 12 Other structural abnormalities that have been described, and may play a role in the development of DFU, include ankle equinus with restricted dorsiflexion; 28 the distal migration of the adipose pads imbedded in the flexor tendons under the metatarsal heads; 29 and thickening of skin, tendons, ligaments, and joint capsules at the ankle and foot. 12
Abnormal foot pressures
Patry et al. 19 performed a systematic review of the role of pressures and shear forces in the pathogenesis of DFU. This review identified multiple studies that have analyzed different pressure and force variables potentially involved in the etiology of ulceration. After careful analysis, only high peak plantar pressures appeared to consistently predict the development of foot ulcers. 19 Peak plantar pressure is the highest amount of pressure under the foot on a specific area, and in patients with diabetic PN, it is typically located at the forefoot.12,19 No specific cutoff value of peak plantar pressure has been adopted, but it seems that the higher the peak pressure, the higher the risk of ulceration. 19 In a large cohort study, Lavery et al. 30 evaluated the effectiveness of dynamic plantar pressure assessment to determine the risk of foot ulceration. In this study, the peak plantar pressures were significantly higher in the group of patients that developed ulcers, although the optimal cut point estimated by receiver operating characteristic analysis (87.5 N/cm2) only yielded a sensitivity of 63.5% and a specificity of 46.3% after excluding patients with LOPS. 30 This study supports the notion that elevated peak plantar pressure is a risk factor for the development of DFU, but when used independently may be a poor tool to predict ulceration.
Trauma
Foot trauma in patients with LOPS is an important component of the multifactorial process that leads to diabetic foot ulceration. 12 While accidental (e.g., blunt injury) or self-inflicted trauma (e.g., toenail cutting) are clearly described as triggers of ulceration, repetitive trauma from day-to-day activities and ill-fitting footwear appear to be the leading precipitants of foot injury.1,12,31 In a prospective cohort study, Macfarlane and Jeffcoate 32 found that rubbing from footwear was the most common precipitant of ulceration, causing 21% of 669 foot ulcers. Reiber et al. 33 also identified minor foot trauma as part of a clinical triad (together with neuropathy and deformity) that was present in the majority of patients with diabetes that developed ulcers. These observations support the importance of preventing foot care as a way to avoid external precipitants of injury.
PAD
Several studies have demonstrated a significant association between PAD and DFU development. 15 PAD (atherosclerotic occlusive disease of the lower extremities) is a major risk factor for the progression of diabetic foot complications and contributes to prolonged ulcer healing, recurrent ulceration, and higher rates of amputation.1,12 Tobacco smoking and diabetes are the strongest risk factors for PAD, followed by hypertension, hypercholesterolemia, and advanced age.34–36 Gregg et al. investigated participants aged ≥40 years from the 1999–2000 National Health and Nutrition Examination Survey. In this non-institutionalized US population, the prevalence of lower extremity PAD defined as ankle-brachial index (ABI) <0.9 (9.5%) was approximately twice as high among individuals with diabetes as in the overall population (4%). 37 While patients with history of tobacco smoking, hypertension, or other risk factors for PAD frequently have more severe atherosclerosis at the aortoiliofemoral level, patients with diabetes usually have a more distal disease involving the femoropopliteal and below the knee arteries. 1 Interestingly, the foot arteries are frequently spared from the occlusive disease. 1
Educate patients and health providers
Patient education
Patient education aiming to promote foot care knowledge and self-examination is advocated by most experts and clinical guidelines as an important strategy to prevent diabetic foot complications.9–12 Education of patients at high risk of ulceration is considered to be particularly important. These patients, for example, are taught to substitute the loss of sensation with alternative senses (e.g., sight or touch) and to avoid situations that may impose a risk of trauma (e.g., walking barefoot or using poorly fit footwear).9 –12 Surprisingly, however, the available body of evidence about the effectiveness of patient education programs has been inconclusive.1,38,39 A problem among studies looking at the value of education has been the significant heterogeneity of the evaluated interventions and endpoints, making the interpretation of the evidence a rather complicated task.1,38 A diverse list of education formats have been investigated (e.g., short foot care classes, weekly lectures, hands-on workshops, behavioral modification programs, telephone reminders, home education sessions) and have looked for outcomes as diverse as nail care knowledge and amputations.1,38
Recently, a Cochrane systematic review of randomized controlled trials assessed the effectiveness of simple patient education interventions on the prevention of diabetic foot complications. 39 Only five trials reported the patient-important outcomes of foot ulceration, ulcer recurrence, or amputation, and the authors were not able to pool the data due to significant heterogeneity. Participants, types of interventions, duration of follow-up, and risk of bias varied greatly between studies. Three trials were deemed underpowered, while the other two studies had contradictory results. The trial by Malone et al. 40 included patients at high risk of ulceration that were allocated to a 1-hour group education session or general diabetes care. In this study, there was a reduced incidence of foot ulceration (risk ratio (RR) 0.31; 95% confidence interval (CI) 0.14 to 0.66) and amputation (RR 0.33; 95% CI 0.15 to 0.76) in the intervention group after 1 year of follow-up.39,40 In the randomized trial by Lincoln et al., 41 patients with diabetes and newly healed foot ulcers were similarly allocated to receive either a single 1-h education session or usual care. After 1 year of follow-up, the RR for ulceration was 1.00 (95% CI 0.70 to 1.44) and the RR for amputation was 0.98 (95% CI 0.41 to 2.34).39,41 Short-term improvements of patient’s self-reported self-care behavior after patient education was found in seven of nine randomized trials. 39
Therefore, there is little evidence to support the effectiveness of simple patient education interventions in reducing diabetic foot complications. We agree, however, with Dorresteijn et al. 39 in that this situation should be interpreted as a “lack of evidence rather than evidence of no effect.” It is important to note that regular care in the control groups may not have differed enough from the simple educational interventions, and that further evaluation of the effectiveness of more comprehensive and structured educational strategies, particularly in the highest risk groups, is still needed. Few studies have provided encouraging, but still inconclusive, results. In a randomized trial by McCabe et al., 42 high-risk patients followed at diabetic outpatient clinics were randomly assigned to usual care or a detailed foot ulceration risk assessment with weekly diabetic foot clinic evaluation, podiatry care, education on daily hygiene, support hosiery, and protective footwear. After two years of follow-up, there were 7 amputations in the intervention group compared with 23 amputations in the control group (RR for amputation 0.30; 95% CI 0.13 to 0.71). 42 Other randomized controlled trials have also investigated the effect of educationally orientated complex interventions and more intensive approaches, but have been limited by methodological flaws and lack of power.43 –46 Until further evidence is gathered, we agree with the current recommendations from clinical guidelines regarding the importance of teaching preventive foot care, particularly in those with sensory neuropathy. Table 1 describes several foot care and self-examination recommendations for patients with diabetes at high risk of ulceration.
Recommendations to prevent diabetic foot complications in patients at risk. a
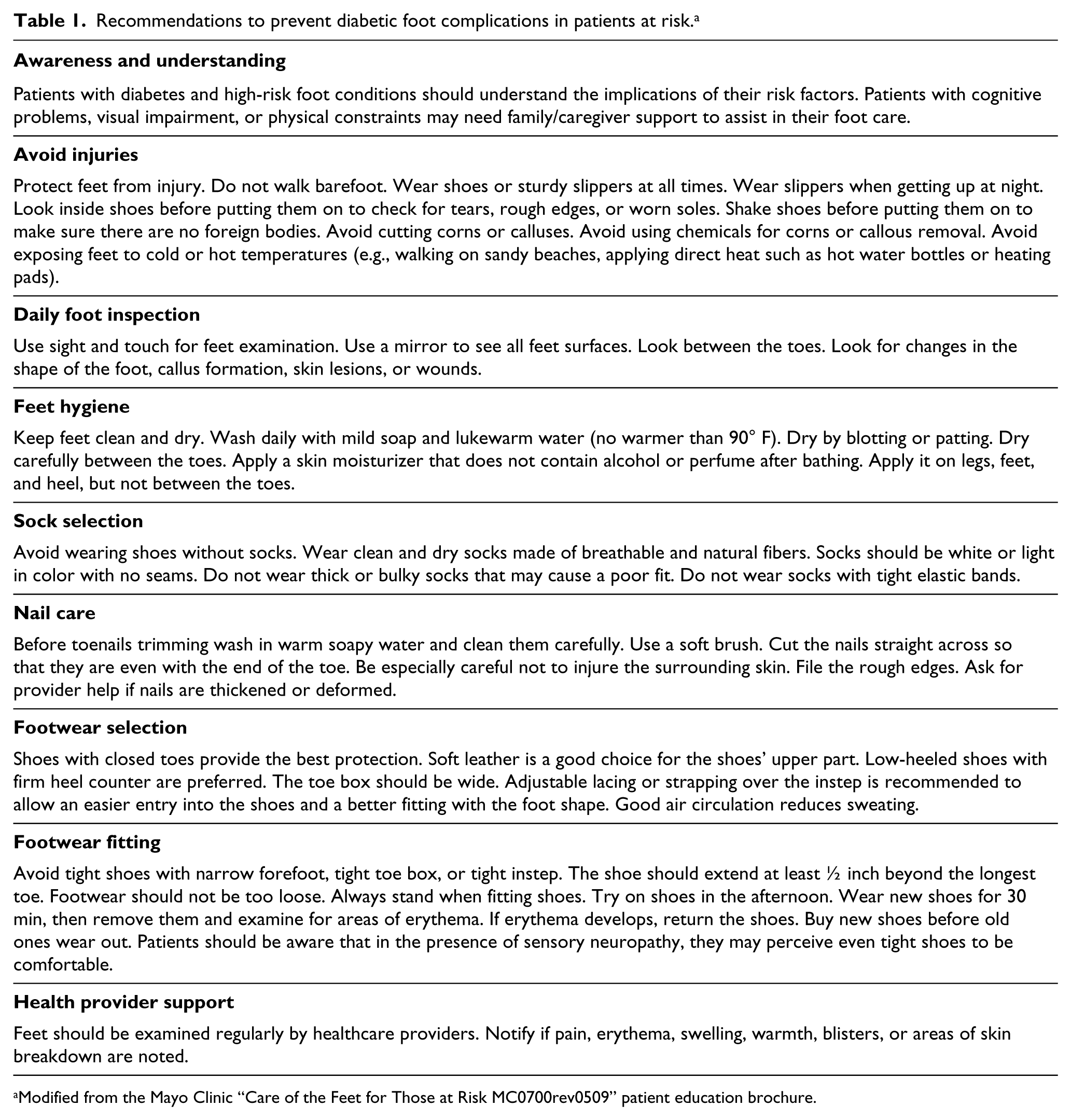
Modified from the Mayo Clinic “Care of the Feet for Those at Risk MC0700rev0509” patient education brochure.
Physician education
Clinicians taking care of patients with diabetes should be able to identify risk factors for the development of foot complications and provide preventive education. It therefore seems advisable to implement strategies oriented toward the improvement of physicians’ diabetic foot knowledge and management skills. Accordingly, the IWGDF recommends that healthcare professionals should receive periodic education to improve the care of high-risk individuals. 11
Structured clinical assessment
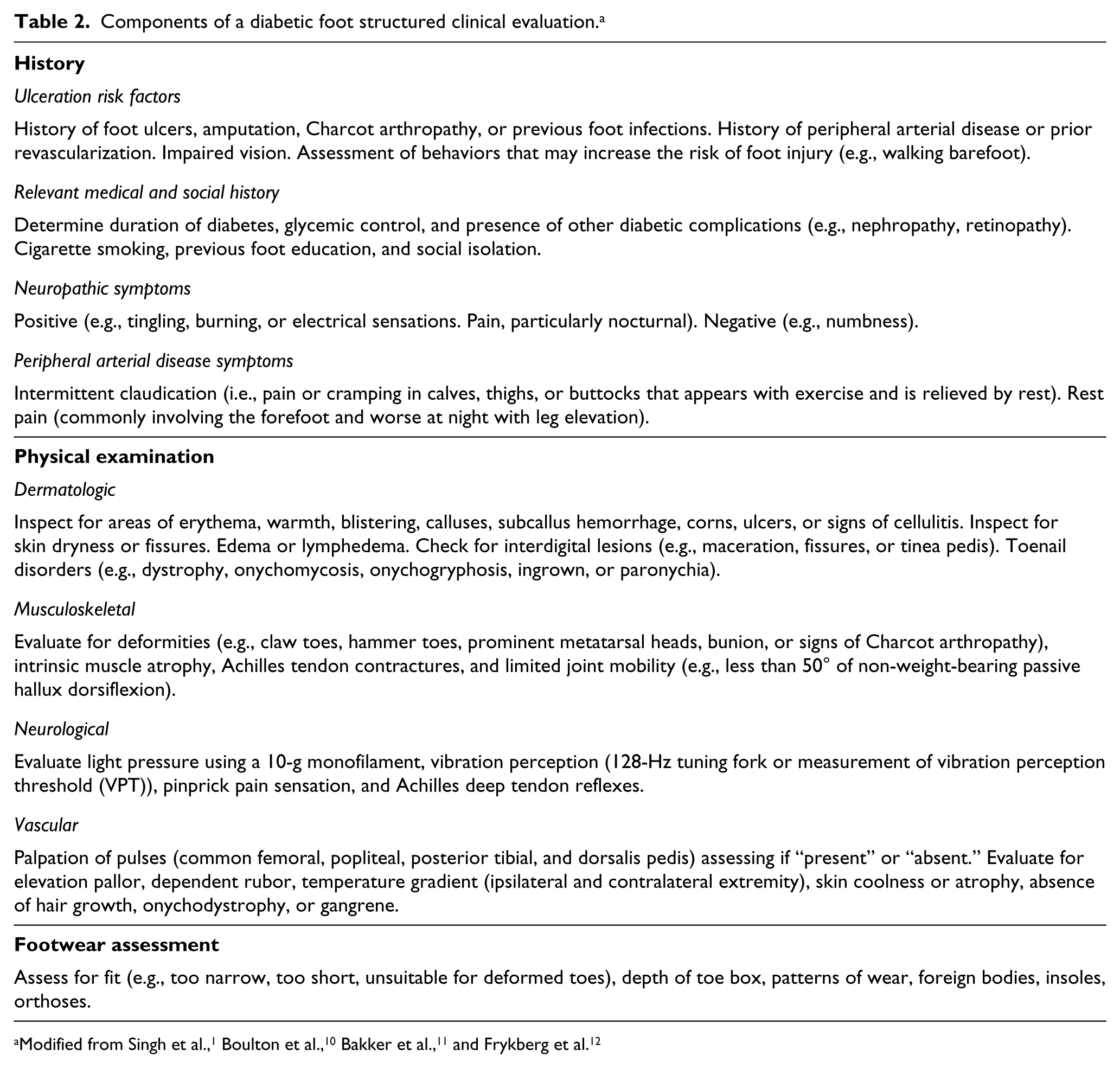
A diabetic foot oriented structured clinical evaluation that systematically collects relevant data from the history, physical examination, and footwear inspection is a key component of the assessment of patients with diabetes (Table 2). Risk factors for foot ulceration should be identified, as well as obstacles for self-care, or potentially risky behaviors that may increase the risk of foot injury. It is particularly important to identify a history of previous foot ulcers or amputations, as these have been consistently recognized as strong risk factors for further foot complications. 15 Clinical guidelines recommend that all patients with diabetes should have a thorough foot examination at least once annually, and more frequently if high-risk foot conditions are identified.9,11 The ADA also advises that visual inspection of the feet should be performed at every healthcare visit. 9
Components of a diabetic foot structured clinical evaluation. a
Skin and musculoskeletal evaluation
Skin examination can provide clues for the presence of areas of increased pressure when erythema, warmth, or calluses are observed. 9 Not unfrequently, an ulcer may develop under a callus, and therefore, careful examination is required. 47 The skin should be inspected for its integrity and for the presence of abnormalities like dryness, fissures, or tinea infections that may facilitate skin disruption. 1 DFU are commonly located on the plantar toes, forefoot, and midfoot, but can also be seen on the dorsal surface of the toes and heels.12,33 Reduced joint mobility and rigid foot deformities, such as prominent metatarsal heads, hammer toes (extension of the metatarsophalangeal joint, flexion of the proximal interphalangeal joint, and hyperextension of the distal interphalangeal joint), or claw toes (hyperextension of the metatarsophalangeal joint, flexion of the proximal interphalangeal joint, and flexion of the distal interphalangeal joint); should be identified, as they can be associated with high-pressure points, skin injury and ulceration.15,48 Significant flattening of the plantar arch associated with swelling and other signs of inflammation should raise the suspicion for Charcot arthropathy. 10
Assessment of LOPS
The ADA recommends that the neurological examination should be directed to identify the presence of LOPS. 10 This can be achieved by the evaluation of light pressure using a Semmes-Weinstein 5.07 (10-g) monofilament, vibration perception (128-Hz tuning fork or measurement of VPT), pinprick pain sensation, or ankle reflexes. 10 Ideally, the 10-g monofilament sensation plus another of the above-mentioned tests should be performed, and LOPS should be established when any of them is abnormal. 10 Nerve conduction studies are not required for the diagnosis of LOPS, although they should be considered when patients present with a rapidly progressive PN, asymmetric symptoms, proximal greater than distal signs, or other clinical findings atypical for diabetic PN. 49 The techniques for the assessment of LOPS as per the ADA, AACE, and the IWGDF are described in Table 3.
Loss of protective sensation assessment techniques.
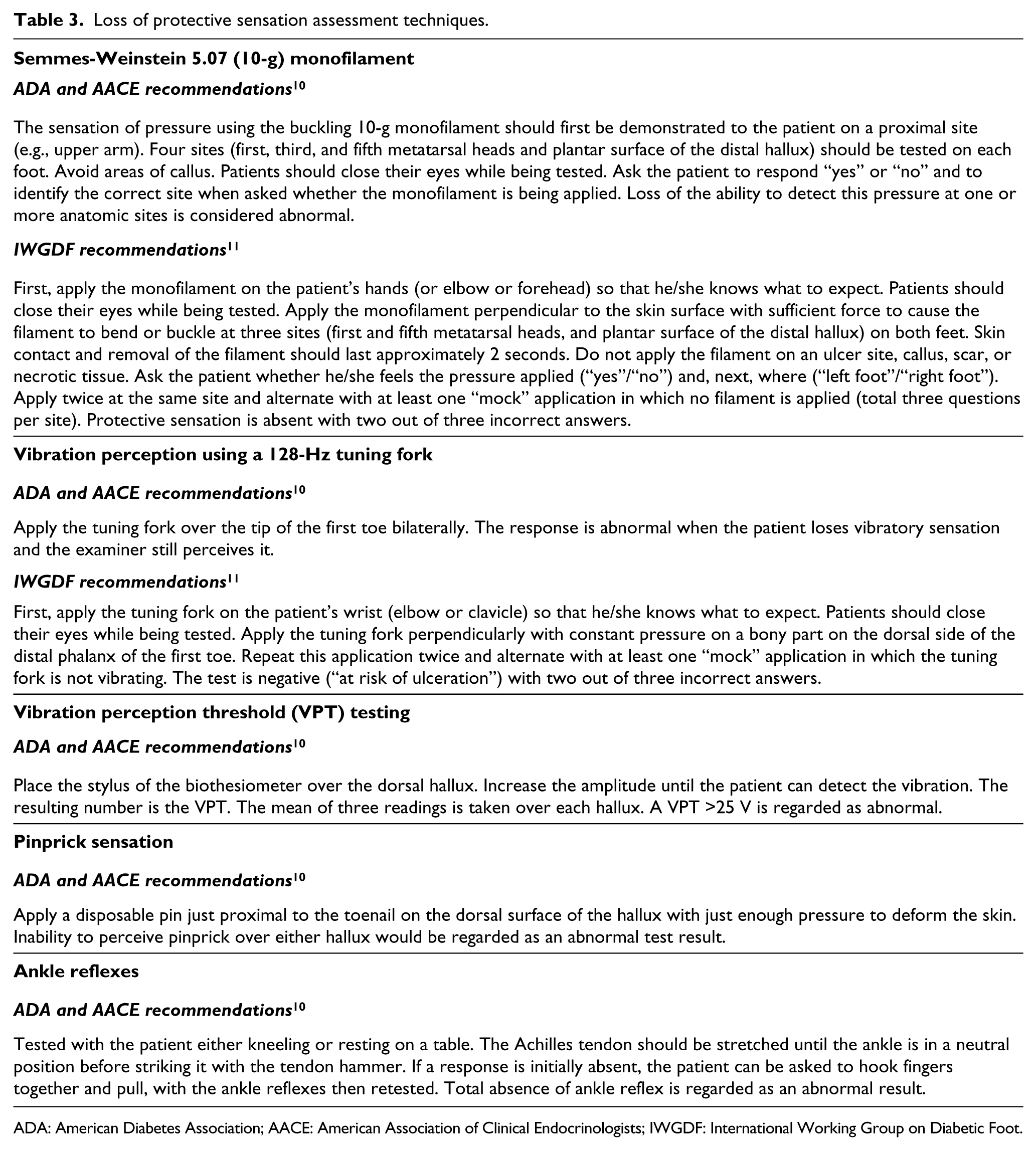
ADA: American Diabetes Association; AACE: American Association of Clinical Endocrinologists; IWGDF: International Working Group on Diabetic Foot.
Many prospective cohort studies have found a significant association between inappropriate pressure sensation using the 10 g force of a 5.07 monofilament and an increased risk of future ulceration and amputation.1,15,50,51 Singh et al. calculated that an altered Semmes-Weinstein monofilament perception had a positive predictive value (PPV) between 18% and 39% and a negative predictive value (NPV) between 94% and 95% for the identification of people at increased risk of ulceration.1,52–54 It should be noted that the location and number of application sites tested with the monofilament, and the diagnostic cut-offs used to define LOPS, varied among the evaluated studies limiting the ability to compare the test accuracy and reproducibility.15,52–54 There is currently no universally accepted method on how to use the monofilament (Table 3). Nevertheless, most studies have evaluated the plantar hallux and the first, third, and fifth metatarsal heads, and considered the presence of one insensate site as evidence of high risk. 50 In a study by Smieja et al., 55 testing these four plantar sites detected 90% of patients with an abnormal 16-site monofilament evaluation. Because there are differences in the accuracy and longevity of monofilaments among manufacturers, the ADA recommends using single-use disposable monofilaments or those clearly proven to be accurate.10,56
In the systematic review by Monteiro-Soares et al., 15 altered tuning fork perception, altered deep tendon reflexes, and the inability to perceive pinprick sensation were all consistently associated with DFU development, although the number of studies that investigated these tests was found to be significantly lower than the number of studies evaluating the predicting ability of the Semmes-Weinstein monofilament. The biothesiometer (neurothesiometer) is a hand-held instrument designed to measure the VPT.1,10 When a threshold of 25 V is used, PPVs between 20% and 32% and NPVs between 95% and 97% have been reported for the identification of individuals at risk of ulceration.1,54,57
Vascular evaluation
The typical symptoms of PAD (e.g., claudication, rest pain) may be subtle or absent in patients with diabetic PN. It is therefore important to take a careful history and perform a thorough physical examination looking for signs of PAD, particularly in patients that already have ulcers. 34 It should be noted that the interpretation of the palpation of pulses is limited by the ability and experience of the examiner, by a high degree of interobserver variability, by significant false-positive and false-negative results, and the fact that up to 10% of the normal population may have absent dorsalis pedis pulses. 34 Despite these shortcomings, clinicians should consider the presence of PAD when pedal pulses are absent. 34 The ABI is the ratio of the highest systolic blood pressure in the pedal arteries (dorsalis pedis or posterior tibial) to the highest systolic blood pressure in the brachial artery, and is measured using a hand-held Doppler probe and a blood pressure cuff. 58 This is a simple, objective, and reproducible non-invasive test that has been found to be over 90% sensitive and specific for the diagnosis of PAD when a threshold index ≤0.90 is used. 58 Mild-to-moderate PAD typically produces ABI values between 0.41 and 0.90, while an index below 0.40 indicates severe obstruction. Patients with long-standing diabetes may have calcified non-compressible arteries and ABI values above 1.3. 59 When this situation occurs, other vascular tests would be required for the diagnosis of PAD. 34 The ADA recommends that a diagnostic ABI should be performed in any patient with symptoms or signs of PAD, and suggests a screening ABI in all patients with diabetes over 50 years of age. If normal, this test can be repeated every 5 years. A screening ABI can also be considered in people with diabetes under 50 years of age who have other PAD risk factors (e.g., smoking, hypertension, hypercholesterolemia, or diabetes for more than10 years). 34
Metabolic evaluation and management
All patients with diabetes should have a complete metabolic evaluation (e.g., identification of the type of diabetes, duration of diabetes, patterns of hyperglycemia, levels of hemoglobin A1c, use and adherence of glucose-lowering agents and consistency of glucose self-monitoring, presence of obesity, unhealthy dietary behaviors, abnormal lipid levels, and statins use) and receive appropriate care according to published guidelines. 60 Among other risk factors for ulceration, duration of diabetes has been identified as a predictor of foot ulcer development in multiple studies. 15 For example, in a study by Rith-Najarian et al., 53 a clear increase in the incidence of plantar ulceration and LEA was seen when the authors compared groups of individuals with diabetes for <9 years, 10 to 19 years, and ≥20 years, particularly in those with insensate foot. There is also epidemiological data supporting an association between poor glycemic control and risk of amputation. Based on a meta-analysis of 14 prospective observational studies involving 94,640 participants, Adler et al. 61 calculated that for each percentage point increase in hemoglobin A1c, there was an associated 26% increase in the risk of LEA.
Adequate glycemic control is a fundamental aspect of diabetes care, 60 and although evidence from trials regarding the benefit of blood glucose lowering in reducing foot ulceration or amputations is scarce and non-conclusive, 61 stronger evidence exists supporting the beneficial effect of enhanced glucose control in the prevention of diabetic neuropathy, particularly among patients with type 1 diabetes. 62 In a Cochrane systematic review and meta-analysis, Callaghan et al. 62 found high-quality evidence from randomized controlled trials in patients with type 1 diabetes in which intensive insulin therapy and enhanced glucose control significantly prevented the development of clinical neuropathy (annualized risk difference of developing neuropathy of −1.84% (95% CI −1.11 to −2.56)). Reductions in nerve conduction and vibration threshold abnormalities were consistently observed. Enhanced glucose control from different interventions also reduced the incidence of clinical neuropathy in patients with type 2 diabetes (annualized risk difference of developing neuropathy of −0.58% (95% CI −1.17 to 0.01)), although this difference was not statistically significant (p = 0.06). 62 This meta-analysis also identified an increased risk of severe hypoglycemia with tighter glycemic control, reminding clinicians of the importance of an individualized and carefully planned management of hyperglycemia.
Assessment of risk
Following a thorough and structured clinical evaluation, patients with diabetes should be assigned a foot risk category. 10 Several stratification systems have been developed in an effort to predict the degree of foot ulceration risk (Table 4). To date, none has been universally adopted by all professional organizations. These systems assign patients to different risk categories based on the cumulative presence of important risk factors for DFU development, and can be used to guide management and monitoring strategies, as well as efficient allocation of resources.1,10,63 –66 The majority of these risk stratification systems have diabetic PN, PAD, foot deformities, and prior history of ulceration or amputation as core variables. 65 In general, studies have shown that there is a significant trend toward more ulcerations and amputations in patients at the higher risk categories, particularly in those with foot deformities, PAD, and previous ulceration or LEA.53,63,65–67
Risk classification systems.

ADA: American Diabetes Association; AACE: American Association of Clinical Endocrinologists; IWGDF: International Working Group on Diabetic Foot; LOPS: loss of protective sensation; PAD: peripheral artery disease; PN: peripheral neuropathy; LEA: lower extremity amputation.
In a retrospective cohort study of patients with diabetes attending a podiatry clinic, five risk stratification systems (including the ADA and the IWGDF systems) were compared in the same cohort in terms of their accuracy to predict foot ulceration at 1 year. 68 The investigators found that all systems predicted a larger frequency of ulceration as the risk groups were higher (p < 0.01) and also that all systems showed excellent sensitivities and NPVs. When the medium and highest risk categories were combined (risk groups 1, 2, and 3), NPVs between 96% and 100% and PPVs between 10% and 17% were found for the identification of DFU development. The highest risk categories had a PPVs between 17% and 30%. 68 The results of this study support the use of risk stratification systems as accurate methods to identify patients at low risk that could be followed less intensively by their primary care providers. Also, these data suggest that almost all patients developing a DFU could be identified by these systems. 68
Team care
The lower extremity complications of diabetes are a group of complex and diverse pathologies that are better evaluated and managed by multidisciplinary foot care teams.10,60,69,70 These teams include primary care physicians, nurses, podiatrists and subspecialists (e.g., endocrinologists, orthopedic foot surgeons, vascular surgeons) that ideally should provide a coordinated process of care. Limited evidence from few studies supports the role of multidisciplinary programs in reducing DFU and LEA in high-risk individuals.15,69,70 Several aspects of the care of these patients needs to be considered. Callus and nail pathology should be treated by trained foot care specialists. Foot deformities may require custom-molded therapeutic footwear fitted and provided by a podiatrist or orthotist. If structural abnormalities cannot be accommodated by therapeutic footwear, carefully selected patients may benefit from surgical correction. 12 Home temperature assessment of the foot is a novel method that has been shown to reduce the incidence of foot ulcers compared with standard preventive care and could be used in motivated people.71–73 Patients with a positive ABI should be referred to a vascular specialist for further assessment and consideration for surgical options. 34 Medical therapy for PAD involves risk factor modification, a supervised exercise program, antiplatelet therapy, and possibly medical therapy for claudication relieve (e.g. cilostazol). 74 Smoking cessation should be strongly encouraged and referral to a smoking cessation program is recommended.
Conclusion
DFU and LEA are common incapacitating complications of diabetes that can be prevented. Clinicians taking care of patients with diabetes should know, understand, and remember the multiple aspects of diabetic foot care. In this review, we described the available evidence and current clinical practice recommendations on this topic. Also, we explained the importance of the recognition of risk factors for the development of diabetic foot complications, the role of patient and provider education, the need of performing a thorough and structured clinical assessment and metabolic evaluation, the key role of assigning patients a risk category for guiding management efforts, and the benefits of a multidisciplinary team approach.
Footnotes
Acknowledgements
The authors would like to thank Drs. Victor M. Montori and Karen L. Andrews for providing insightful comments on an earlier version of this manuscript.
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.