
Abstract
Introduction:
Hip fractures are a cause of significant morbidity. While rare, ipsilateral hip fractures within 12 months after total knee arthroplasty (TKA) can negatively affect the functional outcome and the quality of life for patients who have had TKA. This aim of this study is to investigate (1) the incidence of hip fracture within 12 months after TKA and (2) the influence of hip fracture after TKA on functional outcome and quality of life in patients.
Methods:
Between March 1999 and February 2012, 25 patients who sustained an ipsilateral hip fracture within 12 months after TKA were included in this study. A propensity score matching algorithm was used to select a 1:3 control group without hip fracture. All patients were assessed using the Oxford Knee Score (OKS), Knee Society Function Score (KSFS), Knee Society Knee Score (KSKS), Physical Component Score (PCS) and Mental Component Score (MCS) of SF-36®.
Results:
The incidence of hip fracture was 0.16% among male patients and 0.20% for female patients. At 24 months after TKA, the OKS was 36 ± 7 in the hip fracture group versus 41 ± 5 in the control group (p = 0.003). The KSFS was 50 ± 24 in the hip fracture group versus 68 ± 21 in the control group (p = 0.001), while the KSKS was 83 ± 12 and 87 ± 8, respectively (p = 0.166). The PCS was 37 ± 12 in the hip fracture group versus 47 ± 11 in the control group (p < 0.001), while the MCS was 55 ± 10 and 54 ± 11, respectively (p = 0.664).
Conclusion:
Although hip fracture during the rehabilitation period after TKA is uncommon, these patients have poorer functional outcome and quality of life. We recommend additional caution against hip fracture after TKA.
Introduction
Total knee arthroplasty (TKA) has proved to be cost-effective and efficacious in the treatment for end-stage osteoarthritic knees. The growth in the proportion of obese population, combined with the increased demand from an increasingly elderly population, will inevitably lead to a further rise in the number of patients requiring TKA. 1 By 2030, the incidence of TKA performed will increase by 673% compared with 2005 figures. 2 This statistically emphasizes the importance of evaluating how to best treat TKA patients and what outcomes to expect.
Zhou et al. reviewed 145 patients and found that improvement in knee range of motion and Oxford Knee Score (OKS) plateaued 12 months after TKA. 3 During these 12 months, patients were also observed to have reduced muscle strength, endurance and balance as a consequence of their recovering arthroplasty joint. Hence, they are at increased risk of falling during this recovery period. 4 Lalmohamed et al. reported that patients had a 54% increased risk of hip fracture during the first 12 months after TKA, 5 while Prieto-Alhambra et al. concluded that it was a 57% increased risk in their study. 6 Both studies did report this significant finding among younger, more active patient groups but did not report similar findings in older patients – especially those aged 80 and above. 5,6
Hip fractures are associated with significant morbidity and mortality and, therefore, have been recognized to be a major public health concern worldwide. Like osteoarthritis and TKA, the incidence of hip fractures is expected to rise with an increasingly elderly population. The number of hip fractures occurring in Asia each year is expected to double from 1.24 million in 2018 to 2.56 million by 2050. 7 Earlier this year, Vries and colleagues performed a systemic review focusing on the quality of life in the elderly after hip fracture. 8
Due to the lack of literature, it remains unclear how hip fracture within 12 months from TKA will affect the patients. This aim of this study is to investigate (1) the incidence of hip fracture within 12 months after undergoing TKA and (2) the influence of hip fracture after TKA on functional outcome and quality of life in patients. We hypothesize that the incidence of hip fracture is 0.4% within the first 12 months, and it will negatively affect the functional outcome and the quality of life in patients.
Materials and methods
This retrospective study was approved by our hospital’s ethics committee (CIRB: 2015/3146) and carried out in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki.
Patient selection
Computerized medical records of 2456 male patients and 10,452 female patients who underwent a primary TKA at our tertiary hospital were reviewed. The TKAs were indicated for end-stage osteoarthritis and performed between March 1999 and February 2012. Among these patients, 25 of them sustained an ipsilateral hip fracture after a fall within 12 months from their TKA surgery. Exclusion criteria included patients with concomitant neurological or vascular disease as well as polytrauma patients with other fractures in addition to the ipsilateral hip fracture. None of the 25 patients were excluded.
A propensity score matching algorithm was used to select a 1:3 control group without hip fracture, with adjustment for potential confounders of functional outcome and quality of life after TKA including patients’ age, body mass index (BMI), gender and surgeon.
TKA surgical technique
All TKAs were performed using a standard medial parapatellar quadriceps splitting approach with patella eversion under tourniquet control at 300 mmHg. The distal femur was prepared using an intramedullary rod with the femoral valgus angle set at 5°, while the proximal tibia was prepared using an extramedullary cutting jig perpendicular to the predicted post-operative mechanical axis of the tibia, which was the line drawn through the centre of the talar dome to the centre of the resection surface. 9,10 Our surgical aim was to achieve neutral coronal alignment with a 0° mechanical axis, and femoral rotation aligned to the transepicondylar axis and checked using Whiteside’s line.
Post-TKA rehabilitation protocol
All patients completed our hospital’s standard post-operative TKA physiotherapy protocol. On post-operative day (POD) 1, our protocol included self-assisted passive knee range of motion exercises, static isometric quadriceps exercises with the knee in extension, standing, ambulating with an assistive device as per pain tolerance, continuous passive motion (CPM) and cryotherapy to the operated knee. On POD 2, patients were asked to repeat POD 1 range of motion and muscle strengthening exercises but increasing the number of repetitions to 20, increase ambulatory distance to >15 m, begin stairs climbing training, as well as CPM and cryotherapy to the operated knee. From POD 3 onward including outpatient physiotherapy after discharge, the rehabilitation consisted of repeat POD 2 range of motion and muscle strengthening exercises, further increasing ambulatory distance and stair climbing training. 11
Management of hip fractures
At our hospital, neck of the femur fracture with Garden types I and II fracture patterns were treated with cancellous screws fixation, whereas those with Garden types III and IV fracture patterns were treated with bipolar hemiarthroplasty. Two-part intertrochanteric fractures were treated with dynamic hip screw (DHS) fixation, while three- and four-part intertrochanteric fractures were treated with intramedullary nailing.
Hip fracture patients who were treated with cancellous screws or DHS fixation were kept on protected weightbearing for 6 weeks after surgery. Those who were treated with bipolar hemiarthroplasty or intramedullary nailing were allowed weightbearing as tolerated. Mortality, as well as another episode of fall with fracture after hip fracture surgery, was documented.
Clinical outcome measures
A physiotherapist assessed all patients preoperatively and at 24 months after TKA. We used the OKS and Knee Society Score as knee-specific functional outcome measures. Murray et al. described the OKS as a questionnaire comprising 12 items on daily activities, which the patient must answer. 12 Each item was scored between 0 and 4, with 4 representing the best outcome/least symptoms. Scores from each item were then added to get a global score from 0 to 48, with 48 being the best outcome. A 200-point scoring system developed by the Knee Society was used in our study: 100 points for Knee Society Function Score (KSFS) and 100 points for Knee Society Knee Score (KSKS). 13
Statistical analysis
We used the 36-item short-form health survey (SF-36®; Medical Outcomes Trust, Hanover, New Hampshire, USA) to evaluate the general health of patients. 14 It consisted of eight subscales: physical functioning, physical role, bodily pain, general health, vitality, social functioning, emotional role and mental health. Summary scores had been developed to aggregate the most highly correlated subscales as well as to simplify analyses without substantial loss of information. In our study, the medical outcome study approach proposed by Ware et al. was used to derive two higher order summary scores: Physical Component Score (PCS) and Mental Component Score (MCS). These two summary scores had been found to have good validity in discriminating between clinically meaningful groups, as well as high internal consistency and test–retest reliability estimates when used in a general population. 15
We did a power analysis prior to the conduct of this study, based on the difference in post-operative OKS between the hip fracture and the control groups. A 1:3 allocation ratio was used. To detect a minimal clinically important difference (MCID) of five points in OKS from a baseline mean score of 41 with standard deviation of 5 at a power of 0.95, a sample size of at least 18 patients in the hip fracture group would be required. 16 This calculation was done for a two-sided test with a type I error of 0.05. After including the patients who underwent a primary TKA between March 1999 and February 2012 and sustained an ipsilateral hip fracture within 12 months after TKA, we had 25 patients in the hip fracture group.
Statistical analysis was carried out in consultation with our in-house biostatistician, using SPSS® 19.0 (IBM, Armonk, New York, USA). Statistical significance was defined as a p-value of ≤0.05. The Student’s unpaired t-test was used for the analysis of continuous variables (age, BMI, OKS, KSFS, KSKS, PCS and MCS), while the Pearson χ 2 test was used for categorical variables (gender and side of operated knee).
Results
The incidence of hip fracture within 12 months after undergoing TKA was 0.16% (4 of 2456) among male patients and 0.20% (21 of 10,452) for female patients. The average age of these 25 hip fracture patients was 71 ± 8 years, while the mean BMI was 26.2 ± 3.8 kg/m2 (Table 1).
Patient demographics.

BMI: body mass index.
There were 15 patients with neck of femur fractures (4 cancellous screws fixation and 11 bipolar hemiarthroplasty) and 10 patients with intertrochanteric fractures (7 DHS fixation and 3 intramedullary nailing). Among them, seven had a fall within 3 months after TKA and six each between 4 and 6 months, 7 and 9 months as well as 10 and 12 months after TKA. None of these 25 hip fracture patients suffered mortality or another episode of fall with fracture during the follow-up period.
At 24 months after TKA, both groups of patients showed significant improvement in OKS, KSFS, KSKS, PCS and MCS compared to preoperative scores (all p < 0.05). However, the OKS and KSFS were 5 ± 1 and 18 ± 5 points poorer in the hip fracture group (p = 0.003 and p = 0.001, respectively). The PCS was also 10 ± 3 points lower in the hip fracture group (p < 0.001; Table 2).
Functional outcome and quality of life scores.

OKS: Oxford Knee Score; KSFS: Knee Society Function Score; KSKS: Knee Society Knee Score; PCS: Physical Component Score; MCS: Mental Component Score.
Lastly, the OKS, KSFS, KSKS and PCS between the neck of femur fractures and intertrochanteric fractures showed no significant differences preoperatively and at 24 months. However, the MCS was noted to be 10 ± 3 points poorer in the neck of the femur fracture group (Table 3).
Functional outcome and quality of life scores in the hip fracture group.
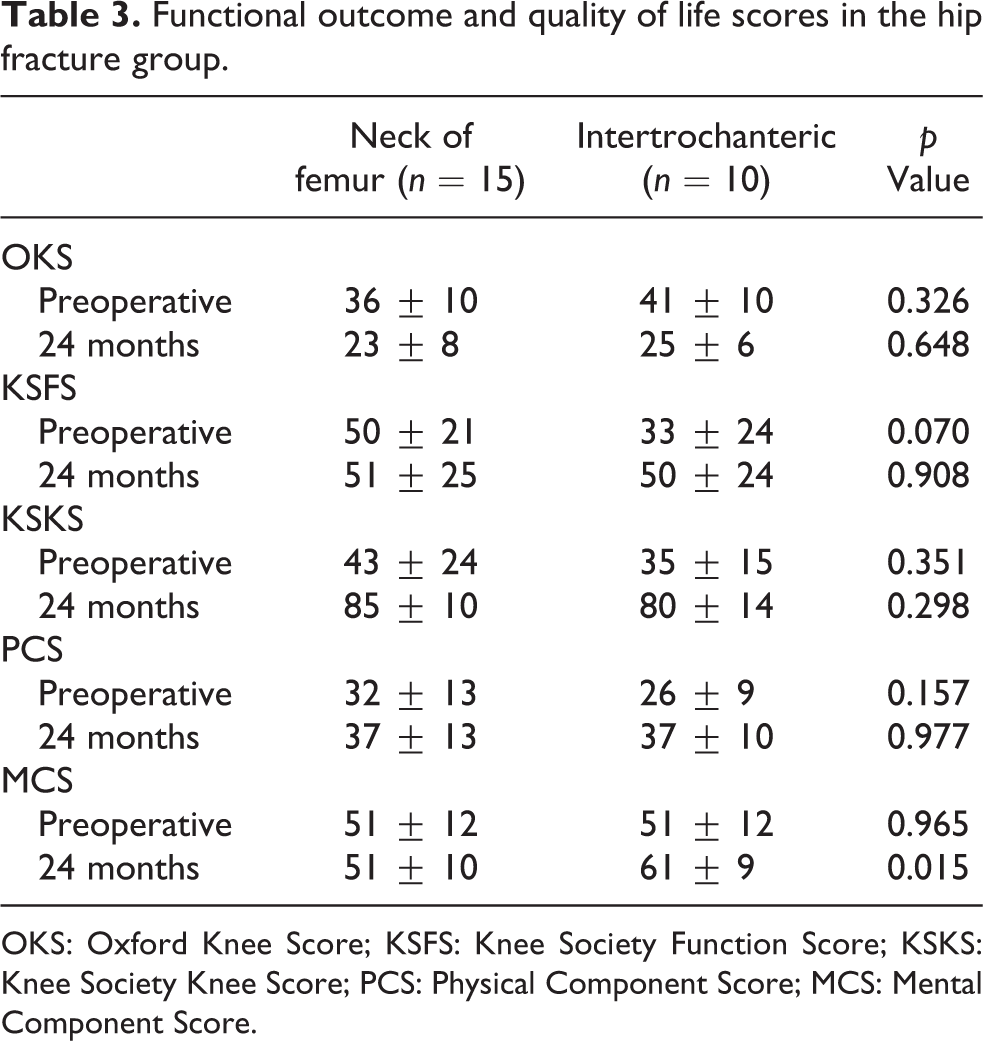
OKS: Oxford Knee Score; KSFS: Knee Society Function Score; KSKS: Knee Society Knee Score; PCS: Physical Component Score; MCS: Mental Component Score.
Discussion
The main findings of this study were (1) the incidences of hip fracture within 12 months after undergoing TKA were 0.16% and 0.20% for male and female patients, respectively; (2) the OKS, KSFS and PCS were 5 ± 1, 18 ± 5 and 10 ± 3 points poorer in the hip fracture group.
The National Working Committee on Osteoporosis reported that the age-adjusted hip fracture incidence per annum for the general population was 0.15% in male and 0.40% in female. 17 In our study, the incidence of hip fracture within 12 months after undergoing TKA among male patients was comparable to the general population. However, it was twofold lower than the general population for female patients, suggesting that TKA may actually reduce the risk of hip fracture in our population. Lalmohamed et al. also found that male patients after TKA had similar risk for hip fracture when compared to the general population, but female patients after TKA were at significantly higher risk than the general population in their study. 5 The difference in hip fracture rates in female patients after TKA is most likely attributed to cultural differences. Within the local setting, greater familial support after TKA may contribute to the decrease in fragility fractures. The majority of our patients only return to the community with dedicated and trained care givers. Other possible reasons for this decrease could attributed to the stability conferred by the TKA.
More recently, there has been increasing interest in determining how much of a difference in the OKS, KSFS or PCS is required before the difference can be considered to be of clinical relevance. Clement et al. reported that the MCID of OKS was 5.0 and 4.3 points for pain relief and function, respectively, while the MCID of PCS was 4.5 and 4.8 points, respectively. 16 Similarly, Lee et al. found that the MCID of KSFS was between 6.1 and 6.4 points. 18 In our study, the OKS, KSFS and PCS were 5 ± 1, 18 ± 5 and 10 ± 3 points poorer in the hip fracture group. These differences in the score are likely to be of significant clinical relevance.
Hip fracture after TKA results in poorer functional outcome and quality of life in patients. Zhou et al. reported plateauing of OKS and knee range of motion at 12 months after TKA. 3 Disruption of their post-TKA rehabilitation programme, prolonged immobility and bed rest due to hip fracture negatively affect post-TKA clinical function scores (Table 2). Knee range of motion and quadriceps strength are important components of OKS, KSFS as well as PCS and when not addressed adequately early after TKA, patients may not yield similar benefits compared to the control group. 19
Even with integrated orthogeriatric care for hip fracture patients, the mortality rate remains high. Stenqvist et al. reported that integrated orthogeriatric care decreased the inhospital mortality rate from 6.3% to 3.1%, 20 while Forni et al. found that it reduced the 30-day mortality rate from 4.3% to 3.4%. 21 Furthermore, Folbert et al. concluded that integrated orthogeriatric care lowered the 12-month mortality rate from 35.1% to 23.2%. 22 Of note, the 12-month mortality rate for hip fracture patients in our study was zero. We postulate that a pain-free arthroplasty joint confers patients’ better mobility and potentially reduces mortality after hip fracture.
To our knowledge, this study represents the only single series available in the literature that has evaluated the influence of hip fracture after TKA on functional outcome and quality of life in patients. With an increasingly ageing population, the number of hip fractures and patients requiring TKA will continue to rise further in the next one to two decades. The findings of our study will provide some insights for counselling patients for TKA. Another strength of our study is sample size calculation, based on the MCID of a validated OKS, has also been done to ensure that this study is adequately powered.
There are limitations to our study. Firstly, there will be inherent selection and observer biases as the patients are recruited from a single tertiary hospital. Future multicentre trials will be required to reduce these biases. Another source of selection bias may stem from patients with hip fractures having weaker muscle strength preoperatively. Muscle strength analysis pre- and post-operatively in future studies may aid in reducing such bias. In addition, the design of this study is retrospective in nature. However, given the low incidence of hip fracture within 12 months after undergoing TKA, conducting a randomized controlled trial will be impractical. Furthermore, protected weightbearing in hip fracture patients who were treated with cancellous screws or DHS fixation may have contributed to lower performance scores. Our hospital’s post-operative rehabilitation protocol has since adopted early post-operative full weightbearing mobilization for all hip fracture patients. Finally, this study addresses short-term outcomes of patients who experience a hip fracture within the first year after TKA. Future studies with longer follow-up will enable assessment of mid- to long-term functional outcomes.
Conclusion
In summary, the incidences of hip fracture within 12 months after undergoing TKA were 0.16% and 0.20% for male and female patients, respectively. Although undergoing TKA does not increase the risk of hip fracture, those patients who sustained a hip fracture during the rehabilitation period after TKA had poorer functional outcome and quality of life at 24 months follow-up. We recommend adequate preoperative fall prevention training and education for all patients undergoing TKA.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the SingHealth Duke-NUS Nurturing Clinician Scientist Scheme (13/FY2017/P1/16-A30); funding was provided for the cost of collecting the functional outcome and the quality-of-life data.