
Abstract
Introduction
Total knee arthroplasty (TKA) is a well-established treatment for lowering pain and improving function in advanced knee osteoarthritis (OA).1–3 According to epidemiologic statistics, the body mass index (BMI) of patients undergoing TKA surgery has increased significantly over time, with a subsequent increase in obese patients.4–6 A high pre-operative BMI is associated with post-TKA physical disability in obese patients with OA.4,7
Previous research has linked a high BMI to a higher risk of TKA failure in terms of outcomes and quality of life.7–11 Other research, on the other hand, has found no relationship or link between BMI and post-TKA results.3,12 Obesity/high BMI is linked to reduced functional recovery and outcomes within a short follow-up period.4,8–10,13,14 Uncertainty exists about the impact of BMI on post-TKA rehabilitation's early mobility and function results. Therefore, the current study investigated the effect of BMI on early phase mobility and function outcome post-TKA.
Methods
A prospective, clinical observational research was carried out at the orthopaedic department of a teaching hospital. Adults with OA/rheumatoid arthritis (RA) who underwent unilateral TKA were recruited and followed over the first 6 months post-TKA. The study duration was from November 2019 to May 2022. The study was carried out in compliance with the principles of the Declaration of Helsinki and Good Clinical Practice (ICH-GCP) recommendations. The Institutional Ethics Committee's (IEC) clearance (approval number: DYP/IECBH/2019/44), as well as participant informed consent, were obtained
Patients who met the following criteria were included in the study: (1) OA or RA receiving unilateral TKA, (2) age >18 years and (3) either gender. The following patients were excluded (1) patients with ankylosing spondylosis, (2) symptomatic OA in the contralateral knee, (3) other lower limb orthopaedic disorders that reduced function, (4) BMI >40 kg/m2, (5) patients who did not start physiotherapy within 2 weeks post-surgery, (6) patients with neurologic impairment, (7) patients with uncontrolled hypertension or uncontrolled diabetes, (8) pregnant women and (9) patients not willing for participation or consent. The study intended to focus on the impact of BMI primarily on overweight and mild/moderately obese individuals, therefore patients with severe (grade III) obese (BMI >40 kg/m2) were excluded.
A pre-designed case record form (CRF) was prepared to record the patient characteristics, clinical examination findings, investigations (laboratory and radiological), surgical intervention and functional outcomes of each patient in a systematic manner. At the pre-operative examination, each patient's BMI was determined. According to the WHO BMI cut-off values,15,16 patients were further stratified/divided into three groups for the study: (Group 1) normal BMI (less than or equal to 25), (Group 2) overweight (greater than 25 but less than 29.9) and (Group 3) obese (equal or greater than 30).15,16
After TKA, the patients were placed on standard rehabilitation program as per the hospital policy which included standard-of-care treatment followed by physiotherapy.
The primary outcomes assessed were pain and functional outcomes during pre-operative and post-TKA periods.
Pre- and post-operative TKA evaluation
The primary outcomes of pain, functional outcome and range of movement (ROM) were measured pre-operatively and post-operatively (after TKA) at 3, 6, 12 and 24 weeks.
Pain and functional outcome was assessed using a numeric graded visual analogue scale (VAS)
17
and Lysholm Knee Scale (LKS),18–20 respectively.
Pain – The VAS was used to assess the level of pain, a numeric scale ranging from 0 to 10, with 0 signifying ‘no pain’ and 10 denoting ‘severe pain’.
17
Functional outcome – The LKS was used to evaluate the knee's functional outcome. The LKS is a patient-rated questionnaire that has been proven to be a reliable and accurate scale for assessing the restoration of functions after knee surgery.18–20 LKS includes eight measures that assess (1) walking gait, (2) knee locking, (3) pain discomfort frequency, (4) stair climbing, (5) external support, (6) body stability, (7) joint swelling and (8) squatting capacity.18–20 Each of the eight measures has been assigned an arbitrary score on an ascending scale. From the patient's responses, a total score (ranging from 0 to 100 points) is computed that best reflects their functional level. A lower score denotes poor knee function, whereas a higher score denotes improved knee function.18–20
In the stratified BMI groups, the pain and functional outcome scores for the primary outcomes were assessed and compared.
Statistical analysis
SPSS software version 21 was used to analyse the data. Actual numbers, mean with SD, median with interquartile range (IQR), percentages and proportions were used to express data. The Kolmogorov–Smirnov test was used to determine the normality of variable distribution. To compare the research variables between groups, the Kruskal–Wallis test and Mann–Whitney U were utilised. For statistical significance, the alpha level was fixed at p < 0.05.
Results
Baseline characteristics
A total of 106 TKA patients were studied. (Table 1) The mean age was 67.41 ± 4.14 years. Out of the total, 61% (n = 65) were females while 38.7% (n = 41) were males. The mean BMI of the patients was 27.19 ± 4.23 kg/m2. Based on BMI distribution, 41 (38.7%) patients had normal weight, 18 (17%) patients were overweight and 47 (44.3%) were obese. (Table 1)
The characteristics of individuals undergoing total knee arthroplasty (TKA).
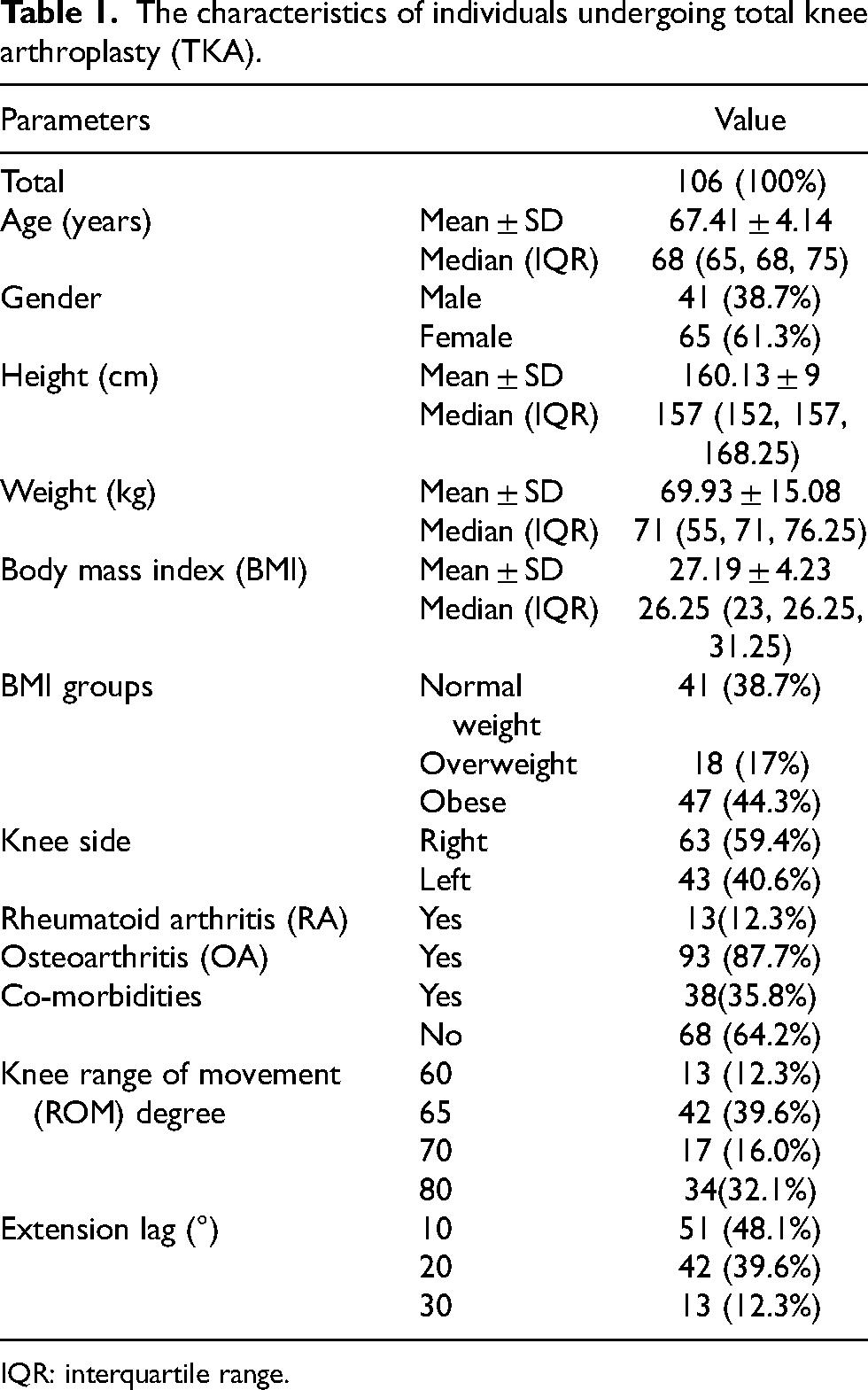
IQR: interquartile range.
Outcomes
Pre-operative LKS total score, VAS pain score and ROM
Table 2 summarises the pre-operative total LKS score, pain score and ROM of the three BMI groups. The median pre-operative LKS total score, VAS pain score and ROM did not differ significantly (LKS: p = 0.202, VAS: p = 0.71, ROM: p = 0.25) across the three BMI groups.
Pre-operative Lysholm Knee Scale (LKS) total score, pain score and range of movement (ROM) between the groups.
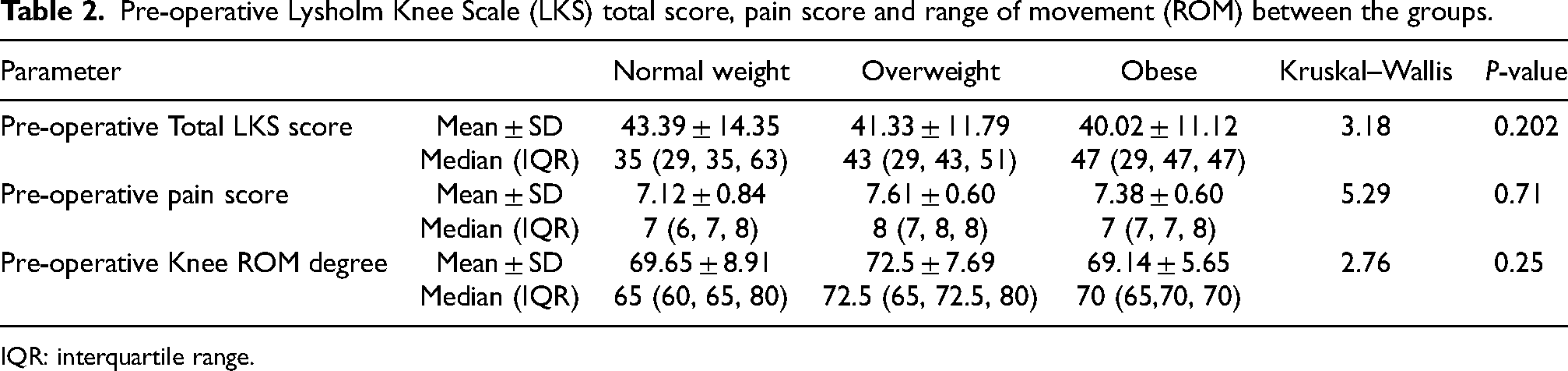
IQR: interquartile range.
Post-TKA LKS total score, VAS pain score and ROM at different time points
Table 3 summarises the total LKS score post-TKA at various time points (3, 6, 12 and 24 week post-TKA). Although the three BMI groups had improvements in the functional outcome (LKS total score) at 6 months, the median LKS total score across the three BMI groups differed significantly at 3 weeks (χ2(2) = 20.7, p < 0.001)) and 6 weeks (χ2(2) = 6.5, p = 0.038) post-TKA.
Lysholm Knee Scale (LKS) total score between the groups at various assessment time points.
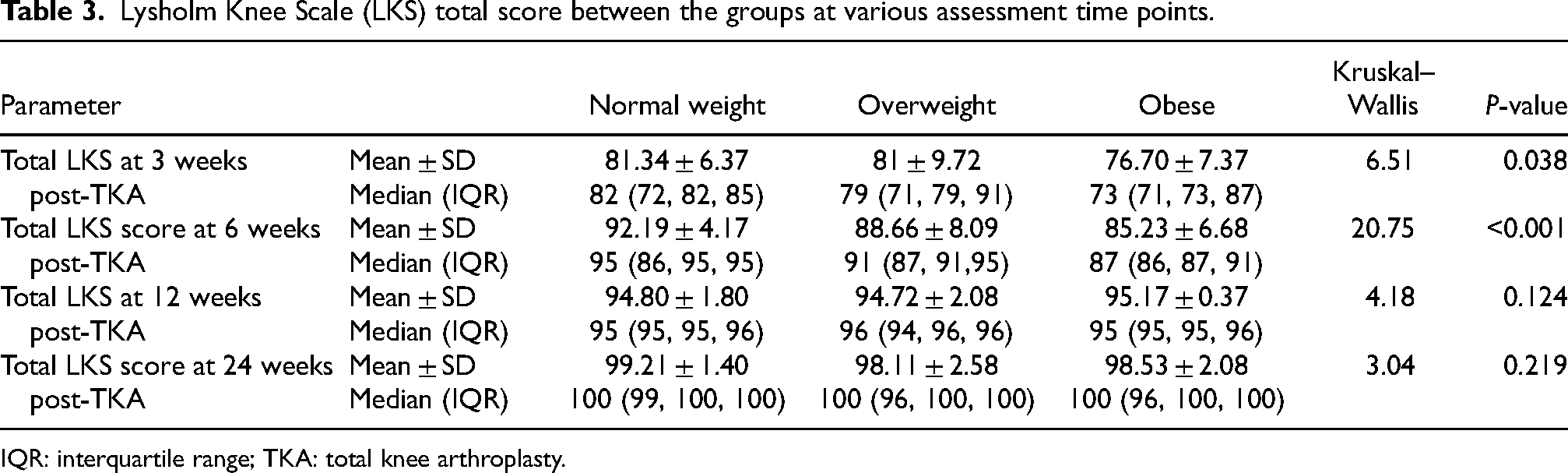
IQR: interquartile range; TKA: total knee arthroplasty.
On subgroup analysis, obesity group showed comparatively lower functional score (lower LKS total score) than other BMI groups and the difference was statistically significant when compared to normal weight group at 3 weeks (U = 685, p < 0.018) and at 6 weeks (U = 439.5, p < 0.001) post-TKA (Table 4).
Subgroup analysis of Lysholm Knee Scale (LKS) total score between the groups.
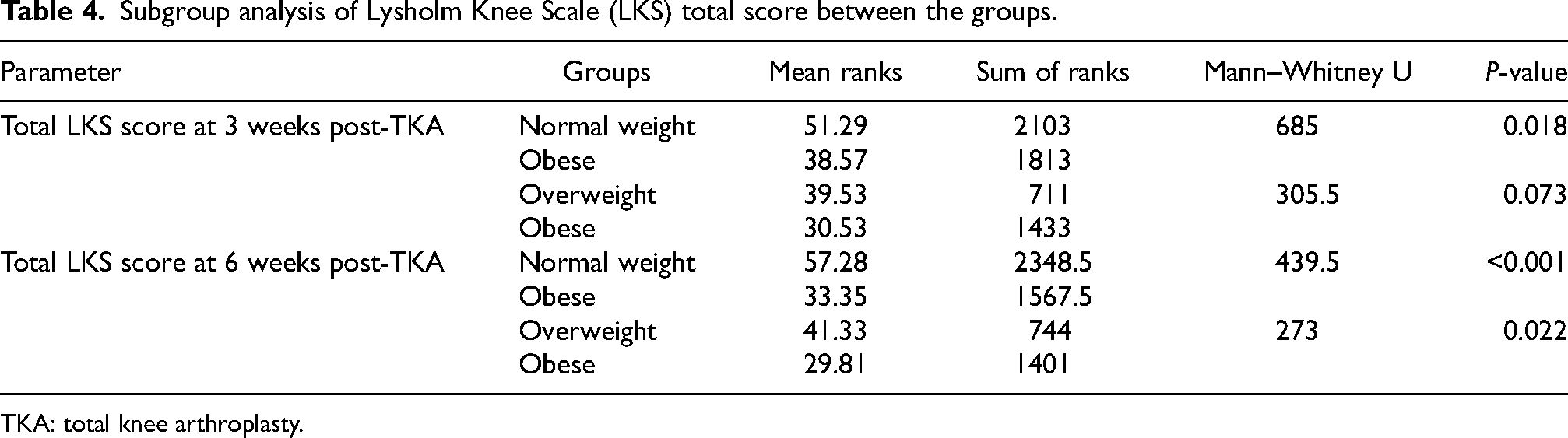
TKA: total knee arthroplasty.
The VAS pain score between the three BMI groups did not differ (p > 0.05) at different assessment time points (3, 6 and 12 weeks post-TKA) (Table 5).
Pain score between the groups at various assessment time points.
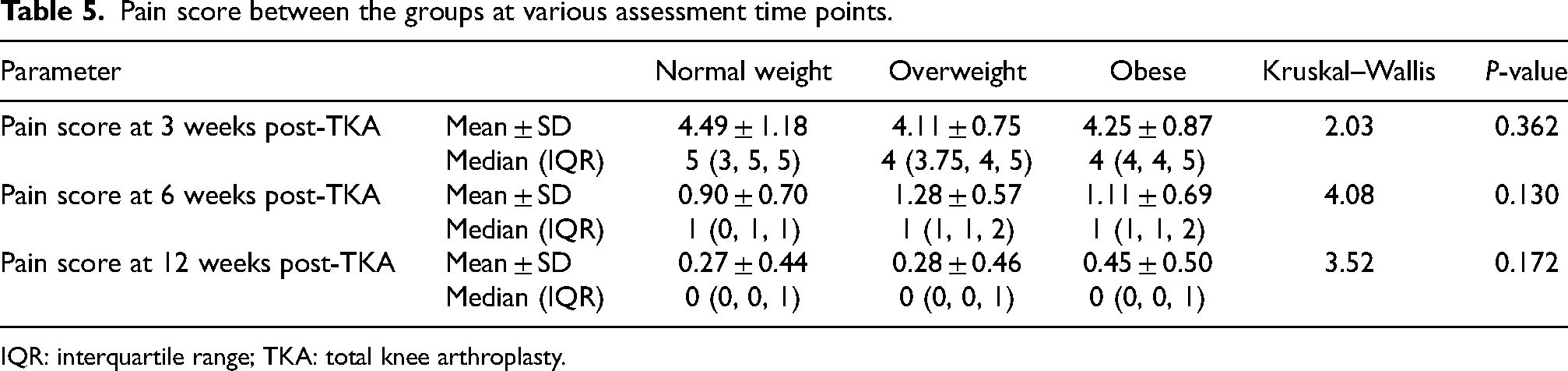
IQR: interquartile range; TKA: total knee arthroplasty.
The knee range of movement degree between the three BMI groups did not differ (p > 0.05) at different assessment time points (3, 6, 12 and 24 weeks post-TKA) (Table 6).
Knee range of movement (ROM) between the groups at various assessment time points.
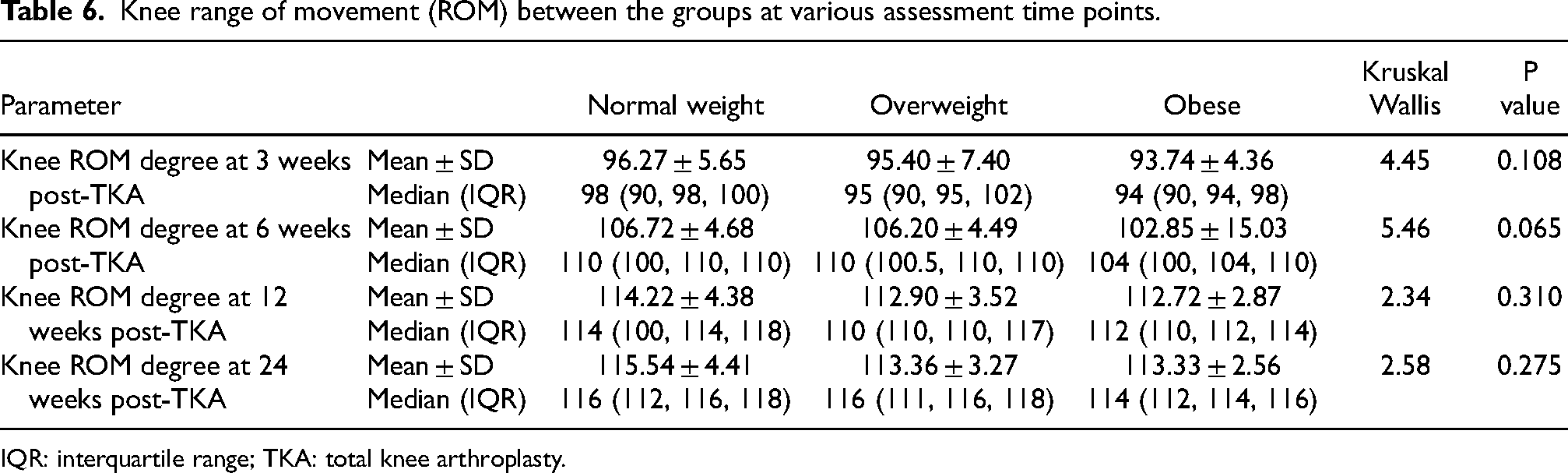
IQR: interquartile range; TKA: total knee arthroplasty.
Discussion
The main outcomes of this research demonstrated that BMI significantly affects functional outcome in the early phases of rehabilitation following TKA, with individuals with lower BMI having early improvement in the functional outcome than those with higher BMI.
TKA is a well-known orthopaedic surgical procedure that has been shown to enhance mobility, function and quality of life in patients with knee arthritis.1–3,16 It presents complications in obese individuals, ranging from linked co-morbidities to difficulties encountered during surgery, delayed wound and function recovery.21,22
Previous studies have shown that obesity has a negative impact on the clinical outcome of TKA, including poor post-operative function restoration, revisions, delayed recovery and wound healing issues.23–26
The evidence on the role and impact of BMI on pain and functional results after TKA is varied and contradictory, with some studies and systematic reviews indicating that outcomes after TKA are lower in obese than in non-obese.24–26 Amin et al., 24 compared morbidly obese (BMI more than 40 kg/m2) to non-obese (BMI less than 30 kg/m2) and documented that at less than 4 years after TKA, morbidly obese patients had lower Knee Society scores, inferior survivorship (pain and revisions) and higher complications. 24 In contrast, the same authors later reported that there were no significant variations in Knee Society scores between subgroups of 370 TKA patients divided as non-obese (BMI less than 30 kg/m2) and obese (BMI >30 kg/m2). 27 Similarly, earlier systematic reviews have shown that obesity adversely affects the outcomes post-TKA including function, risk of complications and prosthetic survival.25,26
Several additional studies, however, have shown that regardless of BMI category, individuals had similar or equivocal outcomes following TKA.28–30 Furthermore, it is still unknown if BMI affects early phase mobility outcomes and functions during post-TKA rehabilitation. As a result, the current study investigated the effect of BMI on early phase mobility and functional outcome during post-TKA rehabilitation.
The current study found that all BMI groups (normal, overweight and obese) showed substantial functional improvement at 6 months post-TKA rehabilitation, as measured by LKS scores. However, at 3 and 6 weeks post-TKA stage, we documented that the LKS score was significantly higher in normal weight than the overweight and obese group (p < 0.05). This data suggested that patients with lower BMI gain early improvement in function/ functional outcome than higher BMI in the short-term phase of post-TKA rehabilitation. At 6 months post-TKA rehabilitation, independent of BMI group, patients achieved a significant absolute functional improvement with no substantial difference in LKS scores among BMI groups. Between the three BMI groups in the present research, there was no evident variation in the VAS pain score at the time points of assessment (p > 0.05). Regardless of BMI group the improvement in pain alleviation was comparable.
The key findings of the present research demonstrated that there was no discernible difference in function or functional outcome at 6 months after TKA, regardless of BMI groups, are consistent with those of earlier retrospective and prospective investigations.3,14,23,31 Study by Stevens-Lapsley et al., 3 demonstrated that there was no significant correlation between BMI and functional performance in the subacute (1 and 3 months) or intermediate (6 months) stages of TKA recovery. 3 Similarly, Giesinger et al., 31 documented that BMI had a detrimental impact on postoperative improvement in joint awareness and satisfaction levels in TKA patients, but no effect on pain and functional outcome (Oxford Knee Score (OKS)). 31
In retrospective research by Ayyar et al., 23 the obese group (BMI ≥ 30 kg/m2) had a considerably lower preoperative OKS compared to the non-obese (BMI < 30 kg/m2). 23 Nonetheless, the follow-up or change scores of the OKS did not show any statistically significant group effects. 23
According to Crosbie et al., 14 lower BMI patients experienced improved short-term functional outcomes during rehabilitation following TKA, but they did not observe any BMI-related changes in walking capacity. 14 Similarly, Clark, 28 reported similar findings and stated that while morbidly obese may attain comparable pain relief, range of motion and ability following TKA, they are likely to be more functionally compromised. 28
Similarly, in a recent systematic analysis by Boyce et al., 32 which included 9 suitable studies out of 110, they concluded that morbidly obese individuals had a functional recovery that is equivalent to non-obese, although they have a greater risk of perioperative complications. 32
In contrast to our findings, Başdelioğlu, 33 in a retrospective study among 588 patients documented a significant difference between the BMI groups (based on WHO classification) following TKA. 33 Better functional outcomes (LKS scores) were obtained in normal BMI group in comparison to other BMI groups. Clinical and functional results decreased as BMI increased. 33 Similarly, Maniar et al., 34 and Yelamarthi et al., 35 also documented lower functional outcomes in obese patients post-TKA.34,35
In this study, pre/post-operative alignment-based evaluation was not performed since it was not a standard practice/policy of the department. However, pre/post-operative alignment might be a confounding factor influencing the outcome and rehabilitation.
Overall, the findings of this study contribute to the expanding body of literature on the effect of BMI on postoperative early function improvement in TKA patients. This study found that BMI affects postoperative early phase functional recovery in TKA patients; however, functional improvements at 6 months were comparable regardless of obesity or BMI class.
Patients with obesity/higher BMI should get extensive counselling on the advantages of TKA, as well as the increased risks and problems associated with increasing BMI following TKA, in order to make an informed shared decision about TKA. Obese individuals should be urged to reduce weight before undertaking TKA, and maintaining weight loss after TKA is recommended.
The study focused on the impact of BMI on functional outcomes following TKA rehabilitation. The study focused on the effect of BMI on early (short and intermediate) functional improvement/recovery following TKA. The ‘Lysholm-Knee-Scale,’ a reliable and validated instrument, was used to assess functional results. The grouping of BMI was based on cut-off levels indicated in the WHO classification for obesity in adults in order to maintain standardisation.
The present study has certain limitations. The study employed a patient-rated functional scoring method, and the sample size was modest. Although only one tertiary care hospital was included, it is difficult to generalise the results to the entire population. The results may have been confounded/affected since the three groups were not matched. Furthermore, some parameters, including the omission of Obesity Class III, pre/post-operative alignment measurements, long-term functional outcomes and associated complications, were not addressed, which might limit the findings of the study. Further randomised clinical studies are warranted to confirm the findings.
Conclusion
BMI influences postoperative early functional improvement in TKA patients; however, the functional benefits after TKA at 6 months were similar, irrespective of obesity or BMI class. Individuals with a higher BMI should be motivated to lose weight prior to TKA and to retain weight loss after TKA.
Footnotes
Author’s contribution
All authors have made substantial contributions to the conception and design of the study, acquisition of data, analysis and interpretation of data, drafting of the article and revising it critically for intellectual content. The final approval of the version is yet to be submitted.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Permission and approval of the Institutional Ethics Committee were obtained (approval number: DYP/IECBH/2019/44).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Statement of human and animal rights
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008.
Statement of informed consent
Informed consent was obtained from all individual participants included in the study.