
Abstract
Background:
This study aimed to investigate the clinical features, current management strategies, and outcomes of open pelvic fracture patients.
Methods:
We performed a retrospective review of data on patients with blunt trauma and open pelvic fractures admitted to our trauma center over a 5-year period (January 2013 to December 2017). Demographic as well as clinical data including injury mechanism, injury severity score (ISS), fracture classifications, transfusion requirements, interventions, length of hospital and intensive care unit (ICU) stay, and prognosis were investigated. Univariate analysis and binary logistic regression were used to identify the risk variables of death. Finally, a brief literature review was performed to understand the current capacity of treatment and prognosis of this type of injury.
Results:
Forty-six patients (36 male and 10 female) were included in this study, mean age 43.2 ± 14.2 years. The overall mortality rate was 17.4%; 43.5% of the patients were hypotensive (systolic blood pressure (SBP) <90 mmHg) on arrival. The average ISS was 31.7 ± 6.7, and the average packed red blood cell (PRBC) transfusion during the first 24 h was 9.6 ± 7.4 units. Five patients (10.9%) underwent transcatheter arterial embolization in the early stage of management. The average hospital and ICU length of stay were 53.0 ± 37.6 days and 14.3 ± 15.3 days, respectively. Statistically significant differences were found in ISS, PRBC units received with the first 24 h, SBP, lactate and base excess on admission, and mechanism of injury when comparing between the death and the survival groups (p < 0.05). ISS and lactate on admission were found to be the independent risk factors for mortality.
Conclusion:
The mortality rate of open pelvic fractures remains high. ISS and lactate on admission were the independent risk factors for mortality. Optimization of the trauma care algorithms for early identification and treatment of this injury could be the key to decreasing mortality.
Keywords
Background
Open pelvic fracture is defined as a fracture of the pelvis associated with direct communication of the bony injury with the overlying skin, rectum, or vagina. Open pelvic fractures remain one of the most devastating injuries to trauma surgeons with mortalities reported to be as high as 50% in the 1970s and 1980s due to uncontrolled early hemorrhage, or late sepsis secondary to contamination of the fracture site by way of open injuries. 1 With the establishment of trauma centers and the application of multidisciplinary protocols, early aggressive fracture management and selective fecal diversion, as well as advances made in modern critical care medicine, the morbidity and mortality associated with open pelvic fracture were significantly reduced to 18% in the 1990s. 1 In the 21st century, the mortality of open pelvic fracture was reported to range from 4% to 45%. 2 –16 The development of a definitive treatment algorithm is limited by the low incidence of this complex injury. Because of the rarity of this severe injury and its poor prognosis, we conducted a retrospective study to evaluate all consecutive open pelvic fractures in patients treated in our trauma center during a 5-year period and explore the risk factors associated with mortality. Additionally, a literature review was performed to outline the current standards of care for this type of injury.
Patients and methods
Patient data collection
Data on blunt trauma patients with open pelvic fractures admitted to our trauma center during a 5-year period (January 2013 to December 2017) were retrospectively reviewed. An open pelvic fracture was defined as one with direct communication between the skin or mucous membrane and the pelvic fracture site. Patients who were under 18 years old or died of their injuries in the emergency department prior to admission were excluded from the study. According to prehospital recording system, two patients with open pelvic fracture were arrested in prehospital phase and died in the emergency department (one severe brain trauma and one cardiac trauma).
The study was approved by the Medical Ethics Committee of the authors’ institution. Our institution is one of the largest urban trauma centers in the southwest of China with more than 2000 beds. Over approximately 200 patients with pelvic fractures are admitted to our trauma center annually. The comprehensive data collected on admitted patients included gender, age, systolic blood pressure (SBP) at admission, admission physiologic data, heart rate, Glasgow coma score, artery blood lactate (Lac) and base excess (BE), time from injury to admission, time from injury to surgery, abbreviated injury scale (AIS), injury severity score (ISS), mechanism of injury, pelvic fracture type, location and severity of soft tissue injury, associated injuries, use of early diversion, use of transcatheter arterial embolization (TAE), length of intensive care unit (ICU) stay, length of hospital stay, packed red blood cell (PRBC) transfusion within the first 24 h, associated morbidity or injuries, overall medical cost, and prognosis.
Management algorithm for open pelvic fracture
Admitted patients were initially assessed according to the standard Advanced Trauma Life Support 17 protocol after arrived in the emergency department. If patients were hemodynamically stable, focused radiological evaluations such as chest, abdominal and pelvic radiography and computed tomography were performed before the patient was transferred to the operating room (OR). Focused abdominal sonography in trauma (FAST) was performed in all the patients suspected with hemorrhage in the abdominal cavity. Patients with positive FAST and failure to respond to medical treatment underwent urgent laparotomy. In patients with hemodynamical instability, the “OR resuscitation protocol” was adopted, meaning that patients were taken directly to the OR and the resuscitation, surgical, and critical care phases commenced within the OR. Wound debridement, perineal irrigation, pelvic extraperitoneal packing, selective diverting colostomy, or external fixation of the pelvis were carried out depending upon the patient’s specific condition. TAE was required in patients with hemodynamic instability after exclusion of intra-abdominal hemorrhage and controlling of external pelvic bleeding. Pelvic fractures were fixed with internal fixation 1 week after the patients were stabilized and showed no signs of local infection. In patients with wounds which did not enable internal fixation or alternatively had severe infection, external fixators were adopted as the definitive treatment for the pelvic ring disruption.
Statistical analysis
All results are presented as either the percentage of patients or means and standard deviation. Numerical data were compared using the Student’s t-test. Nominal data were compared using the Pearson χ 2 test. When the minimal expected count was less than 5, the Pearson χ 2 test with continuity correction or Fisher exact test was utilized. Binary logistic regression analysis was used to identify the risk variables. All statistical analyses were performed using SPSS software (version 13.0, Chicago, Illinois, USA). A two-sided significance value of 0.05 was used for all statistical tests.
Results
Demographic data and mechanism of injury
Between January 2013 and December 2017, we identified 46 patients (40 men and 6 women) with an average age of 43.2 ± 14.2 years who sustained an open pelvic fracture from blunt trauma and were admitted to our trauma center. Patient characteristics are detailed in Table 1. The most common injury mechanism was motor vehicle accident (MVA) accounting for 60.9% of all patients, followed by pedestrian traffic injuries (26.1%) and fall injuries (13%); 43.5% of patients were hypotensive upon arrival (SBP < 90 mmHg). The average ISS was 31.7 ± 6.7, and the average PRBC transfusion with the first 24 h was 9.6 ± 7.4 units. The average length of hospital and ICU stay were 53.0 ± 37.6 days and 14.3 ± 15.3 days, respectively. The average overall medical cost of those patients was US$57,049 ± 41,975.
Patients demographics (n = 46).
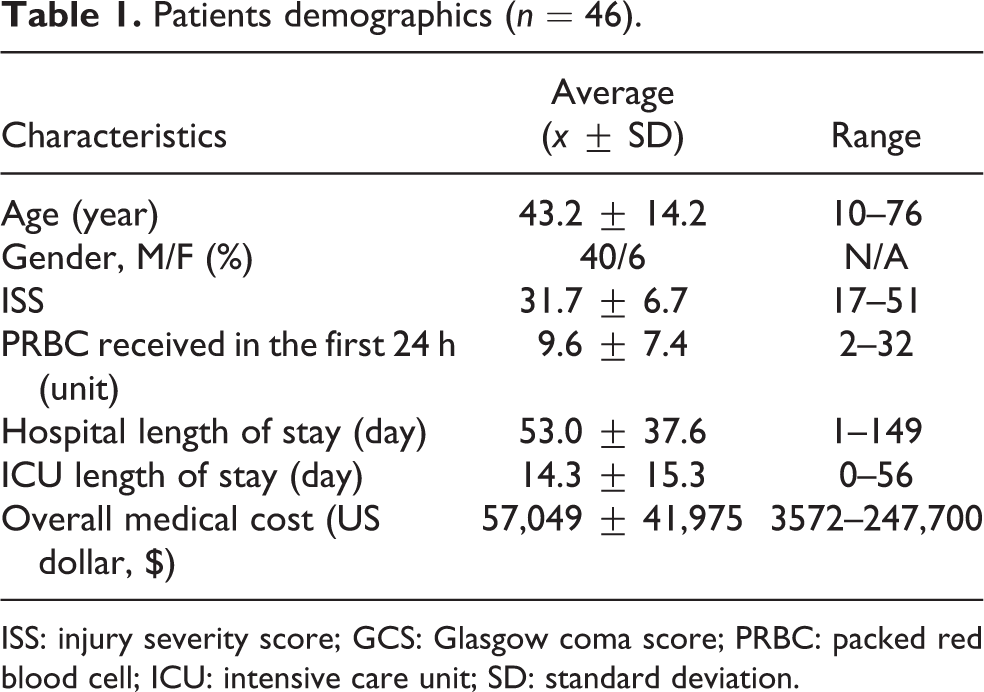
ISS: injury severity score; GCS: Glasgow coma score; PRBC: packed red blood cell; ICU: intensive care unit; SD: standard deviation.
Classification of the injuries
Bony injuries of the pelvis were classified according to Tile classification. 18 The location of soft tissue injuries was classified using the method described by Faringer et al. 19 The severity of the soft tissue injury was classified using the Gustilo–Anderson system, 20,21 and Jones–Powell classification 22 was applied to classify the severity of open pelvic fractures comprehensively. Detailed classifications and the number of patients in each group are presented in Table 2. According to the Tile classification, 23 the most common injury pattern was type B, accounting for 54.3% of all patients (25/46). Zones 1 and 2 were the most common injury areas accounting for 47.8% and 41.3% of patients, respectively. According to the Jones–Powell classification, classes 2 and 3 made up the majority of open pelvic fractures occurring in 93.5% of patients.
Classification details of the patients with open pelvic fracture (n = 46).

Associated injuries and complications
Associated injuries were defined as those with an AIS ≥ 3 for a given body region. 12 Of the 46 patients included in the study, 5 (10.9%) had head injuries, 16 (34.8%) had thoracic injuries, 41 (89.1%) had intra-abdominal injuries, and 25 (54.3%) had extremity injuries. Among five patients with head injury, two received decompressive craniectomy and one died in the first 24 h after surgery. Among 16 patients with thoracic injuries, 14 (87.5%) received closed drainage of the pleural cavity and 1 underwent thoracotomy for severe mediastinal injury. Among 41 patients with combined abdominal injuries, there were 8 rectal lacerations, 2 vaginal lacerations, 4 spleen ruptures, 10 bladder injuries, and 11 urethral injuries associated with the pelvic fractures. Nineteen patients with abdominal injuries received early laparotomy and 14 patients received fecal diversion. Five patients received TAE during the early stage of management, and one died following TAE.
Risk factors for mortality
The overall mortality rate was 17.4% (8/46) with five early deaths (within 24 h of arrival to the trauma center) and three late deaths. Of the five early deaths, one died as a result of severe traumatic brain injury, one had an associated severe mediastinal injury, and three died of hemorrhagic shock. Late deaths were mainly due to sepsis and multisystem organ failure. Differences between the death group and the survival group were analyzed using univariate analysis (Table 3). ISS, PRBC units received with the first 24 h, SBP, lactate and BE on admission, and mechanism of injury were found as having significant difference between two groups (p < 0.05). However, there is no significant difference in gender, age, time from injury to admission, time from injury to surgery, Tile classification of pelvic fracture, Gustilo–Anderson classification for severity of soft tissue injury, Faringer zone for soft tissue injury location, Jones–Powell classification for open pelvic fracture, early fecal diversion, and TAE between the two groups. A forward logistic regression model was created using all variables that have significant difference in univariate analysis. ISS (odds ratio 1.271, 95% confidence interval 1.064–1.516, p = 0.008) and lactate (odds ratio 3.820, 95% confidence interval 1.521–9.592, p = 0.004) on admission were found to be the independent risk factors for mortality.
Univariate analysis between the death group and the survival group.

ISS: injury severity score; PRBC: packed red blood cell; SBP: systolic blood pressure; HR: heart rate; BE: base excess; TAE: transcatheter arterial embolization; GCS: Glasgow coma score; MCV: mean cell volume.
a p < 0.05.
Discussion
Open pelvic fractures are rare and account for only 2–4% of all pelvic fractures. 1 In this study, 46 patients with open pelvic fractures were admitted to our trauma center over a 5-year period, averaging less than 1 patient per month. Because of the low incidence of this injury, obtaining high-level evidence is challenging and remains an obstacle to determining optimal treatment protocols. The mean age of injured patients in this study was 43.2 years old and the mean ISS was 31.7. Among our cohort, young adult males involved in MVA were the most common demographic sustaining this type of injury which was consistent with epidemiological study by Grotz et al. 1
The mortality rates of open pelvic fractures were reported to be as high as 50% in the 1970s and 1980s. 24,25 With the application of multidisciplinary protocols including early, aggressive fracture management and selective fecal diversion, as well as advances made in modern critical care medicine, mortality rates of open pelvic fractures were reduced to 18% in 1990s. 1 However, there has been little advancement in the treatment of open pelvic fractures and a lack of consensus regarding management protocols of such cases over the past two decades. We conducted a brief literature review of studies discussing open pelvic fractures since 2000 and surprisingly found that some recently reported mortality rates were even higher than those quoted above, especially in developing countries. Table 4 summarizes 21 prominent studies of open pelvic fracture from 2000 to 2019 with a total of 782 patients with an overall mortality rate of 24.4%. 2 –16,26 –31 In this study, the overall mortality rate was 17.4%, which is considerably lower than the average of other series. This finding may be attributed to the consistency of multidisciplinary teamwork in dealing with multisystem injuries which may be the most prominent challenge in the treatment of open pelvic fractures. Differences in study populations, evacuation times, and injury mechanisms may also account for the difference in mortality rates. “OR resuscitation” was adopted in dealing with bluntly injured, hypotensive patients in our trauma center which means critical casualties were taken directly to the OR and the resuscitation, surgical, and critical care phases commenced within that room. 32 In some reports with relatively low mortality rates, the authors noted the low incidence of associated injuries as a possible explanation. 10,31 In our series, the mortality rate would drop to 13.6% had we omitted two deaths stemming from associated injuries (one brain injury and one thoracic injury).
Epidemiological data of reported series of patients with open pelvic fractures from 2002 to 2019.

ISS: injury severity score.
Patients with open pelvic fractures often present with massive hemorrhage. In this study, 43.5% of the patients were hypotensive (SBP < 90 mmHg) on arrival and the mortality rate of these patients was significantly higher than those who did not present with hypotension. When dealing with hemorrhagic shock, hemostasis and volume resuscitation should be carried out simultaneously. 33
In the prehospital phase, the use of pelvic binder was thought to be an effective way to control excessive bleeding due to the “chimney effect” of open-book pelvic fractures. 34 However, the results of several recent studies challenged this notion. Ghaemmaghami et al. 35 found that early use of pelvic binders did not reduce pelvic hemorrhage when evaluating the use of an external mechanical compression device on pelvic fractures. In a multicenter retrospective study of open pelvic fractures performed by Cannada et al., 12 it was found that patients with open pelvic fractures who present in shock had a mortality rate of 33%. For those patients on whom a binder was placed, the mortality rate was 32%. In our trauma center, pelvic binders are not routinely used in open pelvic fractures. The overall mortality rate for patients with an open pelvic fracture presenting with hypotension was 30% (6/20). Routine use of a pelvic binder in these injuries could potentially decrease the mortality of open pelvic fractures and warrants further higher level clinical evidence.
Early pelvic fixation is thought to be a vital measure in the hemostatic mechanism since it is assumed that a significant proportion of ongoing hemorrhage stems from the rich pelvic venous plexuses adjacent or small arterial and venous vessels within cancellous bone. External fixation may limit both venous and small arterial vessel bleeding. 36,37 Movement of fracture fragments in the acute phase of trauma care could harbor devastating results for open pelvic fracture patients, potentially disrupting clot formation causing lethal hemorrhage. 38,39 In our trauma center, the external fixator can be placed within 20 min by experienced orthopedic surgeons. In this study, 30 of our patients received external fixation with 6 of these cases resulting in death. The mortality rate was 20% as compared with the overall mortality rate of 17.4%. Although there is no convincing evidence proving the effectiveness of early external fixation for open pelvic fracture patients, our experience indicated that early pelvic fixation did facilitate earlier mobilization, thereby improving pulmonary care, decreasing the risk of deep venous thrombosis, and limiting soft tissue damage by bony fragments. It should be noted that external fixation also brought about additional difficulties for patients with injuries in the gluteal and perianal regions, especially patients sustaining Morel-Lavallée lesions (Figures 1 and 2). In these patients, there seemed to be no suitable positioning to reduce pain or discomfort.

A 37-year-old male with an open pelvic fracture (Tile B, Faringer zone 1, Gustilo–Anderson class 2, Jones–Powell class 3) and Morel-Lavallée lesion. Extensive subcutaneous exfoliation was found in the back. The anteriorly placed external fixator restricted proper care of the posterior wound.

A 48-year-old male with an open pelvic fracture (Tile C, Faringer zone 1, Gustilo–Anderson class 3, Jones–Powell class 3) and Morel-Lavallée lesion. Extensive subcutaneous exfoliation and necrosis of the skin was found in the buttock area.
Open pelvic fractures are usually caused by high-energy mechanisms, studies have shown that the associated abdominal injury rate was greater than 50%. 40 Although management priorities in patients with open pelvic fractures have been well described and have not significantly changed in the last decade, principles of therapy for patients with intra-abdominal injury, especially in patients with multisystem trauma, have changed dramatically during the preceding decade with a strong emphasis on abbreviated laparotomy and damage control surgery. 41 Nineteen patients in this study received exploratory laparotomy for the treatment of associated intra-abdominal injury and 14 received fecal diversion. The timing of laparotomy can frequently pose a clinical dilemma, and the optimal sequence of laparotomy versus pelvic fixation remains unsettled. Moreover, a much greater emphasis was placed on intra-abdominal hypertension and abdominal compartment syndrome (ACS) in our trauma center, both primary and secondary. The abdominal pressure was routinely monitored and treated according to the clinical practice guidelines from the World Society of the Abdominal Compartment Syndrome. 42,43 Thus, we determined that no patients died of ACS in this study.
TAE was usually used when preperitoneal pelvic packing or other hemostatic measures failed to stop bleeding. Pelvic angiography is best indicated for arterial bleeding. 37,44,45 However, debates in the literature have focused on the effectiveness of hemorrhage control and consequent complications. 46 –52 In our study, five patients received early TAE, with one of these patients dying. There have also been reports of extensive gluteal necrosis after TAE in severe pelvic fractures. 47 –52 In our study, two patients (40% of TAE patients) suffered gluteal necrosis after TAE which was much higher than previous reports (Figure 3) while keeping in mind the small sample size. However, in a retrospective chart review of 20 patients with severe pelvic fractures and hemorrhage performed by Auerbach et al., 53 selective TAE of internal iliac branches including the gluteal arterial branches appears to be safe in patients with pelvic and acetabular fractures with or without orthopedic surgical treatment. Nonselective TAE of the internal iliac artery may also be safe when performed unilaterally. 53

A 49-year-old male with open pelvic fracture (Tile C, Faringer zone 2, Gustilo–Anderson class 3, Jones–Powell class 2). Extensive soft tissue necrosis transpired after transcatheter arterial embolization.
Hemipelvectomy has been reported by several authors as the final option in the management of severe unilateral open pelvic fractures with uncontrollable bleeding. 54 In this study, one hemipelvectomy was performed in the emergency phase and stopped the bleeding successfully (Figure 4).

A 32-year-old female with a devastating open pelvic fracture (Tile C, Faringer zone 1, Gustilo–Anderson class 3, Jones–Powell class 3) who arrived at our emergency department 2 h after injury with severe hypotension. Mass transfusion protocol was activated immediately, hemipelvectomy was performed simultaneously to stop excessive bleeding and the patient finally survived.
The prevention or control of post-injury sepsis in open pelvic fractures is a controversial topic. Approximately one-third of the mortality in patients suffering from open pelvic fractures is related to sepsis from an infectious source in the pelvis. 55 However, when infection occurs, it is unclear whether it occurs at the time of injury or by fecal contamination during the subsequent hospital stay. In our study, five patients underwent early diversion with one death. In the 1970–1980s, fecal diversion was regarded as an obligatory procedure to minimize infectious complications associated with open pelvic fractures. 56,57 In 1994, Faringer et al. challenged this notion and suggested selective management for fecal diversion in open pelvic fractures depending on the region of the wound. 19 Recent studies recommended that patients should undergo diversion if the rectal or soft tissue injuries in zone 1 were involved in the open wound. 58 There is still a lack of evidence on whether early colostomy guided by Faringer zones could potentially minimize pelvic infection.
It has been reported that the open pelvic fractures require higher transfusion volumes as compared with the closed pelvic fractures. 31 With the widespread adoption of damage control resuscitation and the experience gained in the battlefield, there is an increasing awareness that fluid resuscitation for casualties in hemorrhagic shock is best accomplished with fluid that is identical to that lost by the casualty. 59 According to Tactical Combat Casualty Care Guidelines for hemorrhagic shock, 60 whole blood is the first choice for fluid resuscitation followed by 1:1:1 plasma:RBCs:platelets and others. However, due to the limitations of blood product storage and pathogen screening technology, whole blood transfusion seems impractical in the current clinical situation. A massive transfusion protocol with 1:1:1 ratio of PRBC, fresh frozen plasma (FFP), and platelets was followed in our trauma center. And the average PRBC, FFP, and platelets received in the first 24 h for open pelvic fractures were 9.6 units, 7.5 units, and 4.4 units separately in this series.
The use of modern vacuum sealing drainage (VSD) dressings makes it possible to manage large wounds with better control of exudative secretions while segregating the wound from fecal contamination. It also allows for ideal conditions in terms of wound healing and granulation in high-risk locations in trauma patients. However, the application of VSD dressings in the zone 1 area may be challenging because it is difficult to guarantee the settlement of the foam material and maintain adequate sealing. In this study, 36 patients with open wounds received VSD dressing. While we failed to quantify the results of VSD placement, the overall results upon clinical examination were satisfying. In one patient with a large skin and soft tissue defect in the hip area, a rectus abdominis flap was used to cover the defect area (Figure 5).

A 49-year-old male with an open pelvic fracture (Tile C, Faringer zone 2, Gustilo–Anderson class 3, Jones–Powell class 2). Extensive soft tissue necrosis arose after transcatheter arterial embolization. Large skin and soft tissue defect in the hip area. A rectus abdominis flap was used to cover the defect area.
As previously described, the rarity and complexity of traumatic open pelvic fractures makes it highly difficult to design a standardized prospective study addressing mortality risk factors and management strategies. The prognosis of open pelvic fracture patients is highly dependent on the capabilities of trauma centers as well as injury mechanism and associated injuries. The limited sample size and retrospective nature were the main limitations of this study. Studies with larger sample sizes and prospective designs are required to optimize and standardize protocols managing such patients.
Conclusion
Open pelvic fractures are highly lethal and require a resource laden multidisciplinary approach predominantly available at large trauma centers employing standardized trauma workflows with high availability of expert personnel. ISS and lactate on admission were the independent risk factors for mortality. Optimization of the trauma care algorithms for early identification and treatment of this injury could be the key to decreasing mortality.
Footnotes
Author contributions
Qingshan Guo, Letian Zhang wrote the first draft and revision of the manuscript. Hua-yu Liu and Zhiyang Zhang contributed to data collection and interpretation. Siru Zhou and processed the data and performed the statistical analysis. Tomer Talmy and Lianyang Zhang contributed in revision of the manuscript and discussion of result. Yang Li designed and supervised the study. All the authors critically contributed to the finalization of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Project of National Key Laboratory (SKLZZ201603&SKLYQ201901) and Clinical and Teaching Innovation Cultivation Project of Army Medical University (CX2019JS109&2019CXJX018).