
Abstract
Introduction
Geriatric distal femur fractures pose a difficult problem for orthopaedic surgeons with an aging population. The present study aims to report mortality rates following distal femur fractures from a geriatric population over 60 years old, with a primary emphasis on determining whether surgical management differentially affects mortality rate as compared to conservative management.
Methods
Patients over 60 years old with distal femur fractures for patients admitted into the New Territories West Cluster from 2012 to 2020 were identified in this retrospective cohort study. Patient demographics, comorbidities, and management characteristics were examined and analyzed. Kaplan-Meier survival analysis was done to delineate differences in mortality rates between surgical and conservative management. Further analysis was done for patients >80 years old using Kaplan-Meier survival analysis to delineate whether surgical intervention still affects the survival in this narrowed geriatric population. Subsequent multivariate cox regression was done to determine variables with significant effect on mortality in this age group.
Results
Of 168 patients, the 1-year mortality rate is 21.5%. The cumulative median survival time of the surgical group (5.98 years) versus the conservative group (2.32 years). Survival analysis on patients >80 years old revealed age, management type, ambulatory status, place of residence, dementia, chronic pulmonary disease, or chronic kidney disease had statistically different median time of survival. In these patients, a reduction in death hazard by 47% (CI 0.28–1.01, p = 0.05) was seen in those with surgical management. On the other hand, patients with chronic obstructive pulmonary disease (COPD) and moderate chronic kidney disease (CKD) show an increased death hazard by 2.61 times (CI 1.23–5.53, p = 0.01) and 7.17 times (CI 1.47–34.86, p = 0.02), respectively.
Conclusion
Compared to conservative management, surgical management resulted in higher cumulative survival in geriatric patients with distal femur fractures. Unfavourable factors that may contribute to a lower cumulative survival includes history of COPD and CKD.
Introduction
Geriatric distal femur fractures pose a difficult problem for orthopaedic surgeons with an aging population. The incidence of distal femur fractures has been recently reported to be 8.7 per 100000 per year. 1 Like hip fractures, distal femur fractures are associated with notable morbidity and mortality in elderly patients. 2 A myriad of factors has been found to influence the mortality in geriatric hip fractures; however, factors influencing the mortality rate in geriatric femur fractures are limited in the international setting,3–7 let alone the local setting. Furthermore, there is no clear consensus for the selection of patients for surgical intervention unlike those with geriatric hip fractures.
The present study aims to report mortality rates following distal femur fractures from a geriatric population over 60 years old, with a primary emphasis on determining whether surgical management differentially affects mortality rate as compared to conservative management. Secondary analysis to identify the effects of age, gender, presence of periprosthetic, displaced or intraarticular fractures, ambulatory status, places of residence and comorbidities on the mortality rate of distal femur fractures in a geriatric population will be done. This is the first large-scale local retrospective cohort study to compare the management outcomes and identify factors that may affect survivorship in the geriatric population with distal femur fractures.
Methods
This retrospective cohort study was performed in the New Territories West Cluster (NTWC) of Hong Kong with three major hospitals in the region including one tertiary centre. Distal femur fractures with and without implants involving the distal metaphyseal-diaphyseal junction to the articular surface of the femoral condyles were included in this study. We defined our geriatric population as individuals over 60 years old admitted between January 1, 2012 and December 31, 2020. Our subjects were identified using the Clinical Data Analysis and Reporting System on January 30, 2021. A total of 168 patients were identified after exclusion of pathological fractures. The average age of these patients was 84 ± 9.719 (range 60–102). A majority of our patients (86.4%) were female. The mean follow-up in our series is 2.53 years.
Patients were divided into those managed conservatively (i.e., splintage, bracing, Jones’ bandaging and traction) and operatively (i.e., nailing, plating). Demographic data, premorbid status, Charlson comorbidity index (CI), were collected to assess the mortality-influencing variables. Charlson CI was calculated according to a 19-condition weighted index (Table 1). 8
Charlson Comorbidity Index: A 19-condition weighted index.
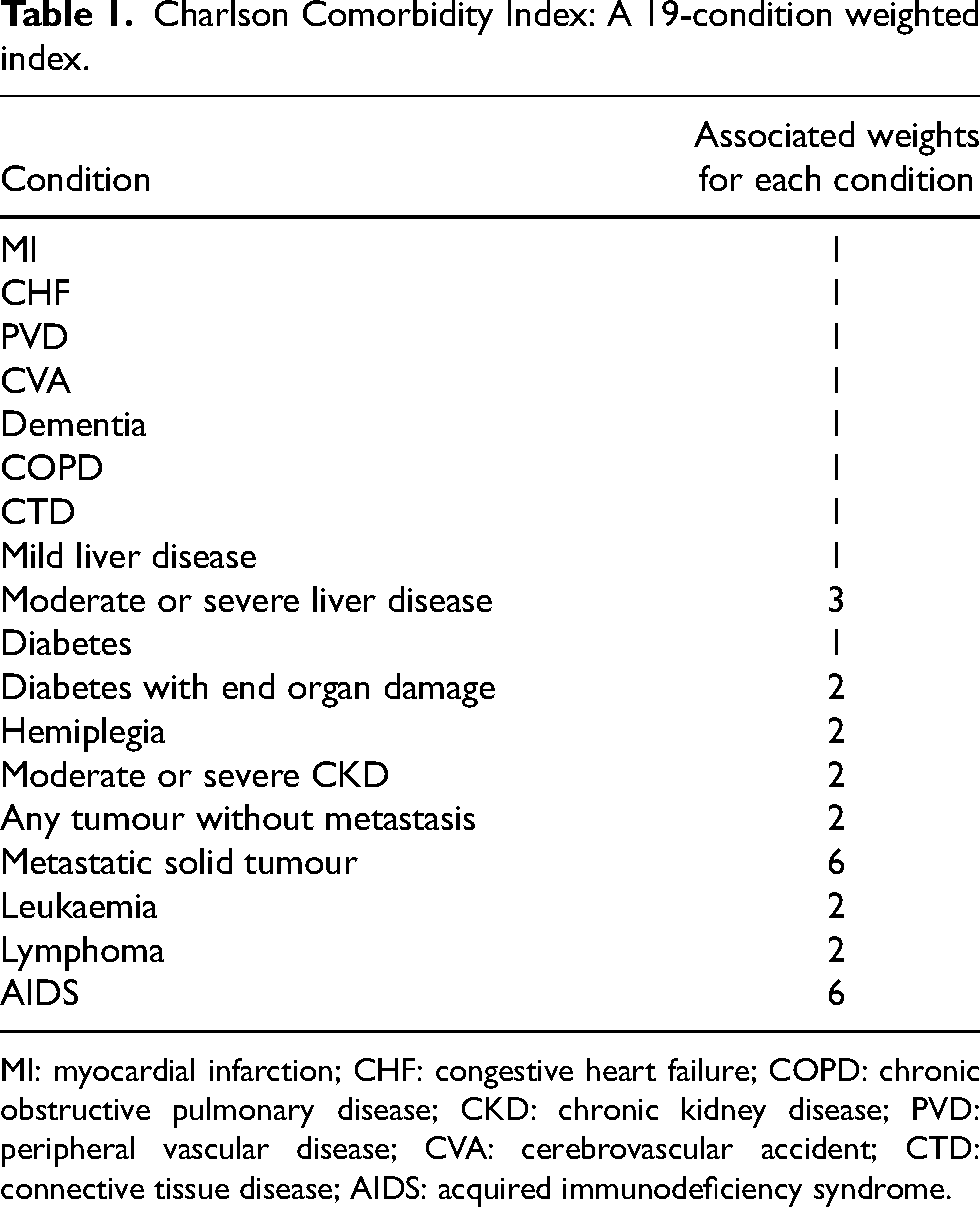
MI: myocardial infarction; CHF: congestive heart failure; COPD: chronic obstructive pulmonary disease; CKD: chronic kidney disease; PVD: peripheral vascular disease; CVA: cerebrovascular accident; CTD: connective tissue disease; AIDS: acquired immunodeficiency syndrome.
The data analysis was performed using SPSS (version 26). The cumulative mortality rates at thirty days, 6 months, 1 year and at conclusion of this study were determined. Mortality of patients by patient demographics, management types, ambulatory status, place of residence, fracture types (extra-articular vs. intraarticular and undisplaced vs. displaced), presence of a periprosthetic fracture and comorbidities as per Charlson CI were compared and plotted using Kaplan-Meier survival analysis. Further analysis was done for patients >80 years old using Kaplan-Meier survival analysis to delineate whether surgical intervention still affects the survival in this narrowed geriatric population. Subsequent multivariate Cox regression was done to determine variables with significant effect on mortality in this age group. Statistical significance was shown with p value <0.05. This study was approved by the NTWC Research Ethics Committee.
Results
General demographics and characteristics
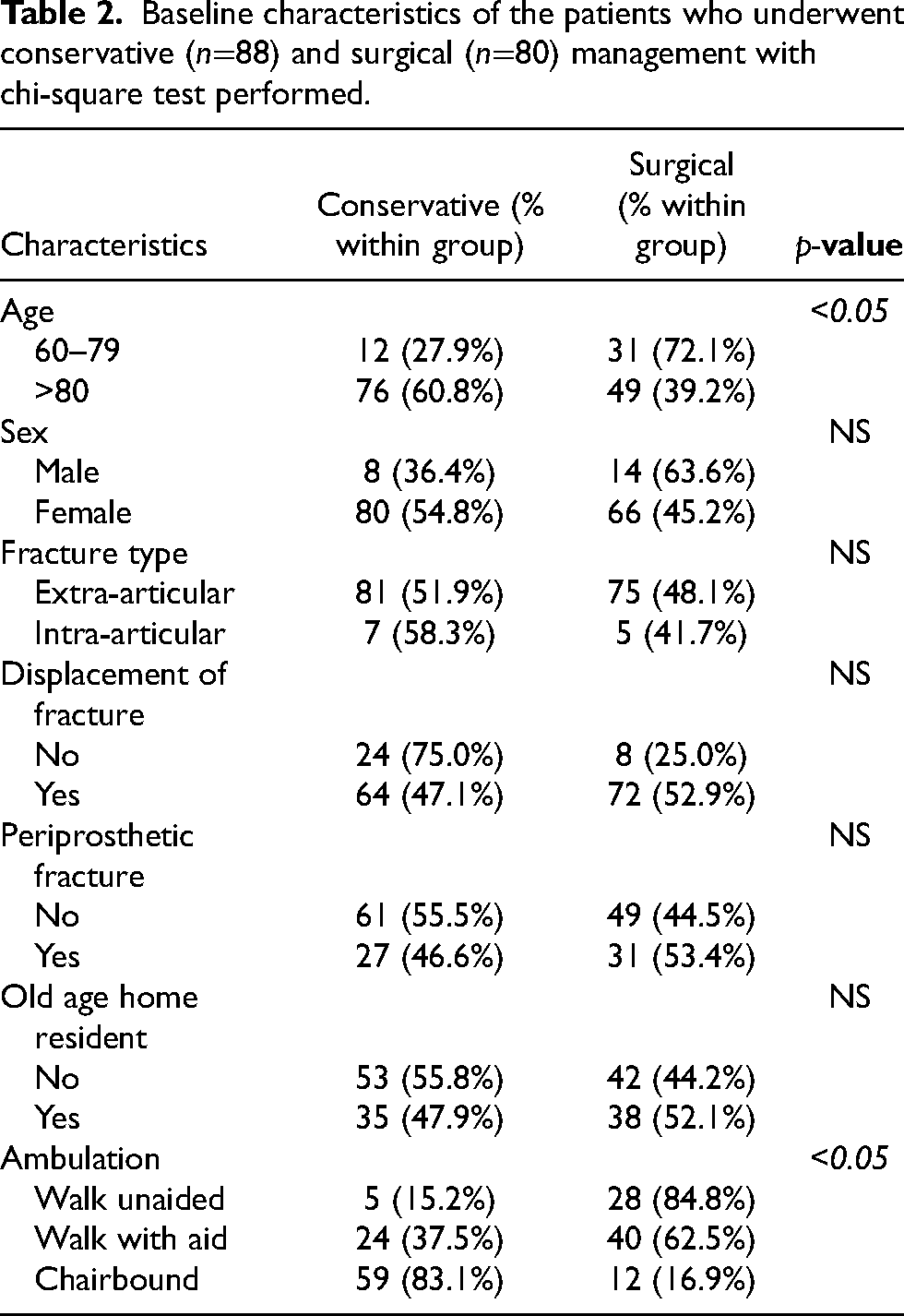
There were 88 and 80 patients who underwent conservative and surgical management respectively. Baseline characteristics of these two patient groups are summarized in Table 2, with the choice of management being differentially affected by age and ambulation status. The mean Charlson CI was compared in the two groups and showed no statistical difference. (Figure 1) Thirty days mortality rate for this cohort of patients was 5.4% while 1-year mortality rate is 21.5%. (Figure 2)
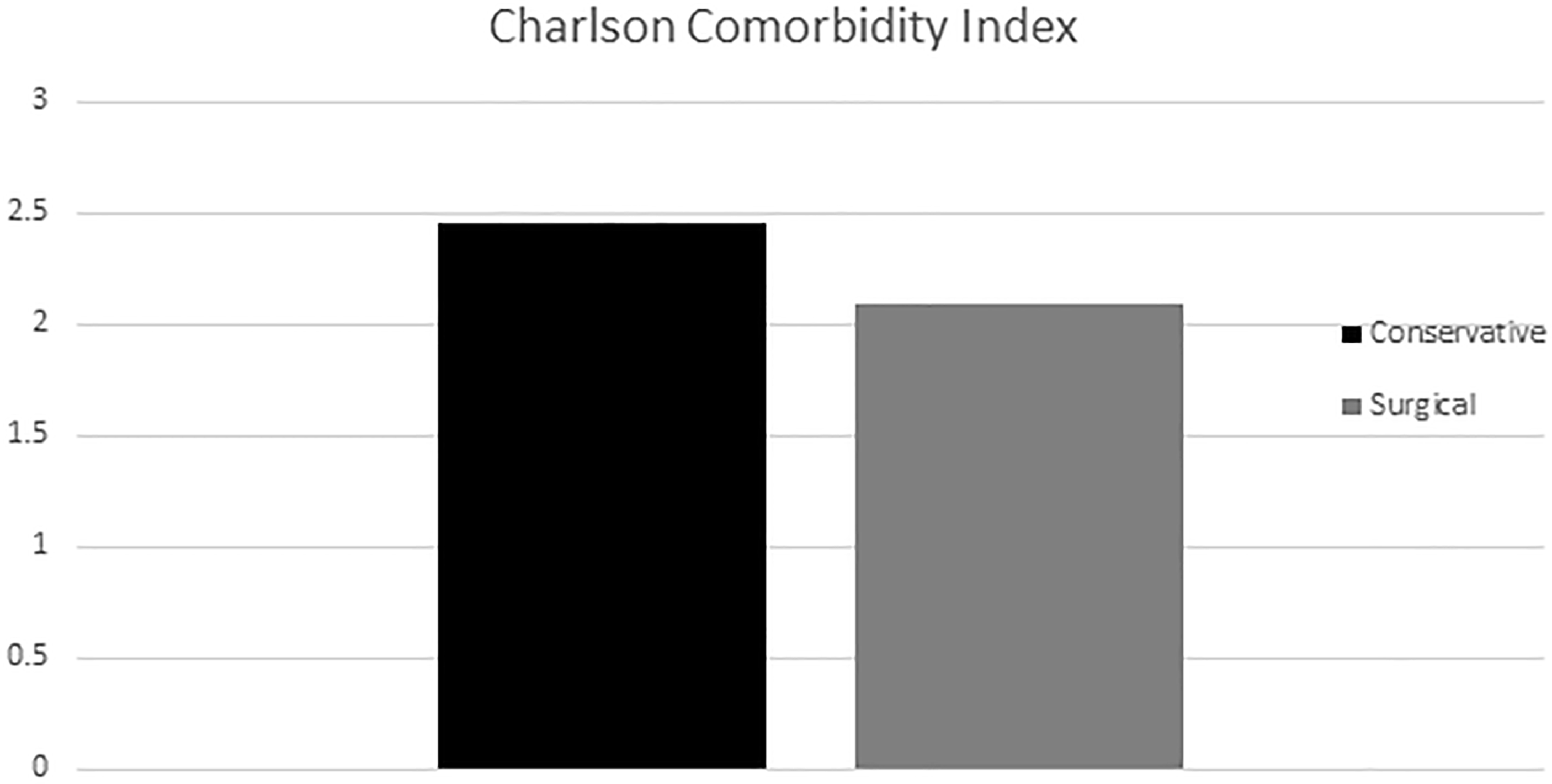
Mean Charlson Comorbidity Index (CI) for patients who were treated conservatively and surgically. There was no statistical difference in the Charlson CI for these two groups of patients.
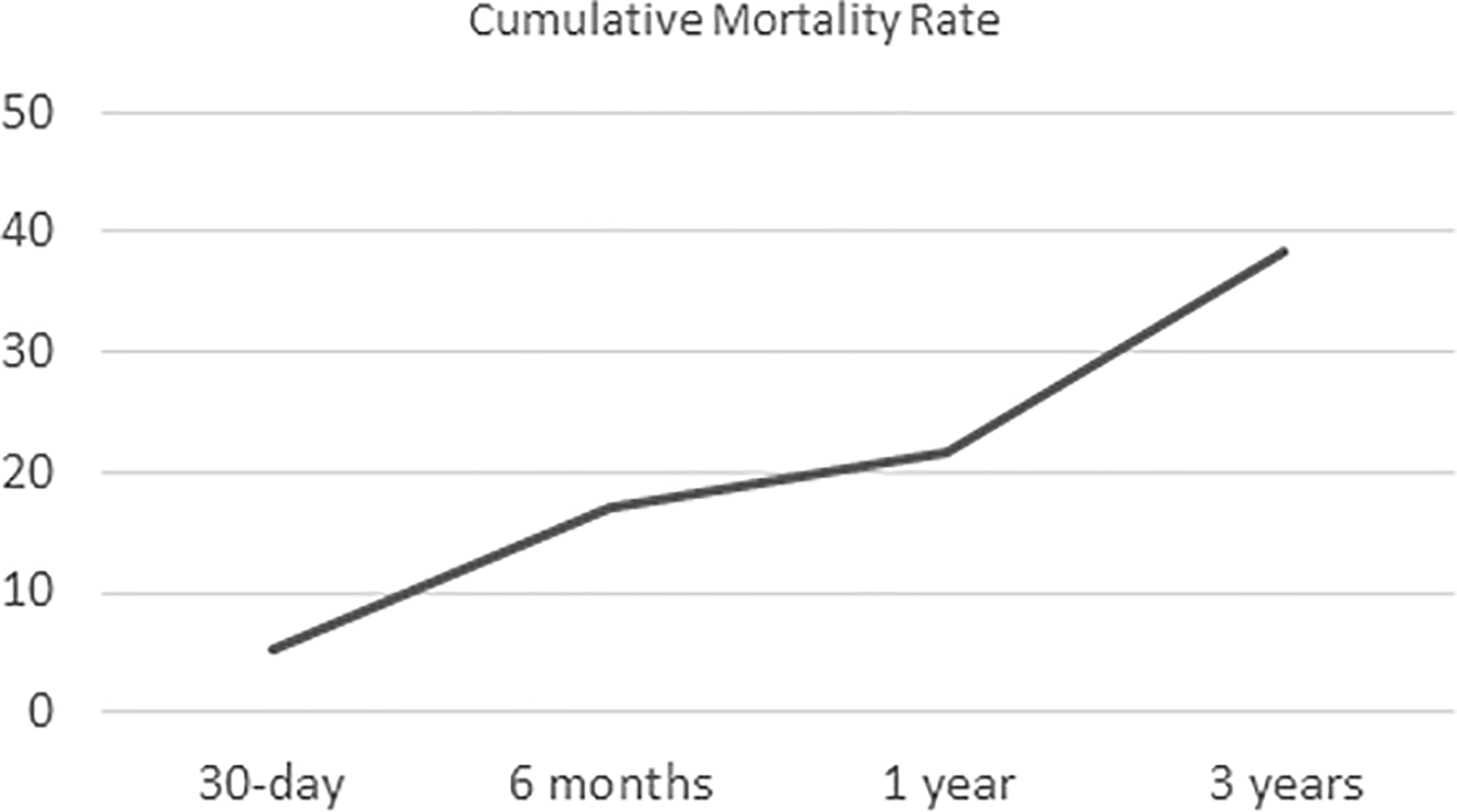
Cumulative mortality rate of patients over 60 years old with distal femur fractures admitted to New Territories West Cluster (NTWC) from 2012 to 2020.
Baseline characteristics of the patients who underwent conservative (n=88) and surgical (n=80) management with chi-square test performed.
Survival of all geriatric patients (>60 years old) with distal femur fracture by demographics, management type, premorbid status, fracture type and comorbidities
The cumulative survival of patient was found to be significantly affected by age, management type, ambulatory status, place of residence, and medical comorbidities including myocardial infraction, dementia, chronic obstructive pulmonary disease (COPD), severe chronic kidney disease (CKD) and local or metastatic tumour. Most importantly, the cumulative median survival time of the surgical group (5.98 years) versus the conservative group (2.32 years) was statistically significantly different. Those who had periprosthetic, displaced or intra-articular distal femur fracture had no differences in survival compared to those who do not. Summary of the variables analyzed in the univariate Kaplan-Meier analysis is summarized in Table 3.
Summary of variables with a median estimate for survival time at the end of the study for all patients >60 years old.
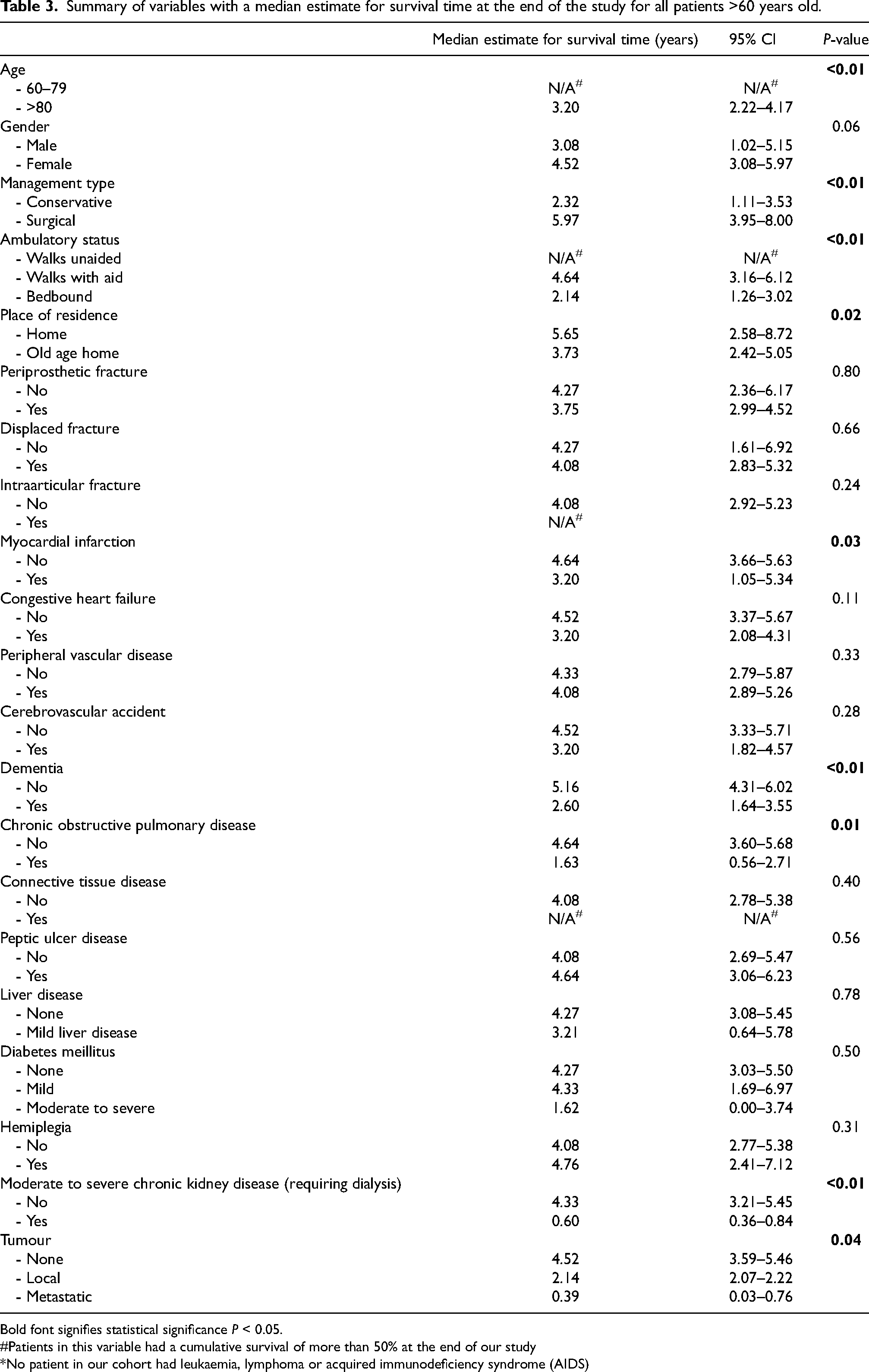
Bold font signifies statistical significance P < 0.05.
#Patients in this variable had a cumulative survival of more than 50% at the end of our study
*No patient in our cohort had leukaemia, lymphoma or acquired immunodeficiency syndrome (AIDS)
Kaplan-Meier analysis revealed that age, ambulatory status, place of residence, management type and certain medical comorbidities are statistically significant variables. (Table 4) Specifically, on comparing the management types, the cumulative median survival time in patients >80 years old of the surgical group was 4.75 years compared to the conservative group of 2.10 years. (Figure 3(a)) Patients who have different status of premorbid ambulation (Figure 3(b)) and places of residence (Figure 3(c)) had statistically different cumulative survival as well. Survival analysis on independent comorbidities as per the Charlson CI revealed that comorbid conditions including dementia, COPD or moderate CKD had a statistically decreased median estimated survival time.
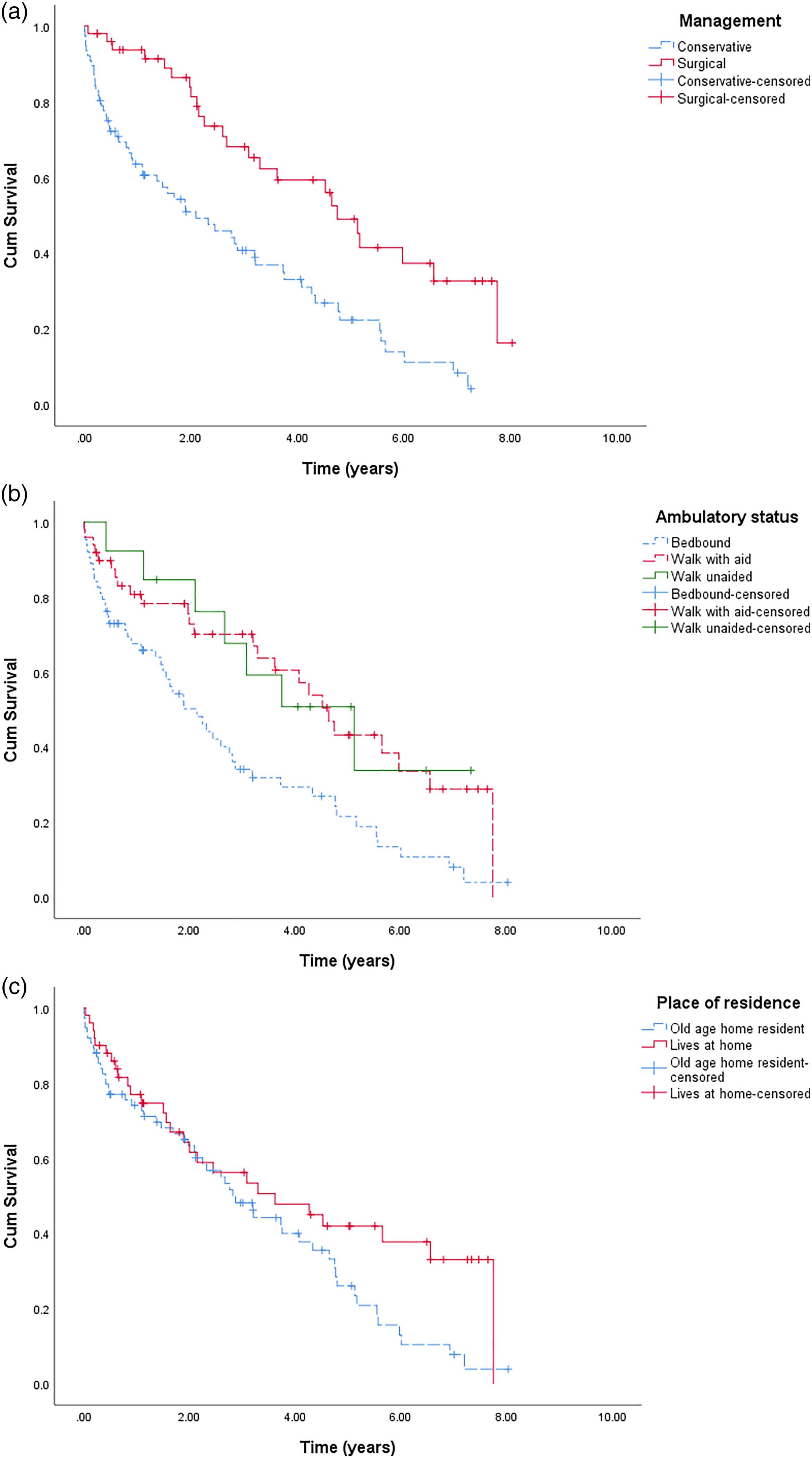
Cumulative survival of patients >80 years old with distal femur fractures by (a) management type, (b) ambulatory status and (c) place of residence.
Summary of variables with median estimate for survival time at the end of study for patients >80 years old.
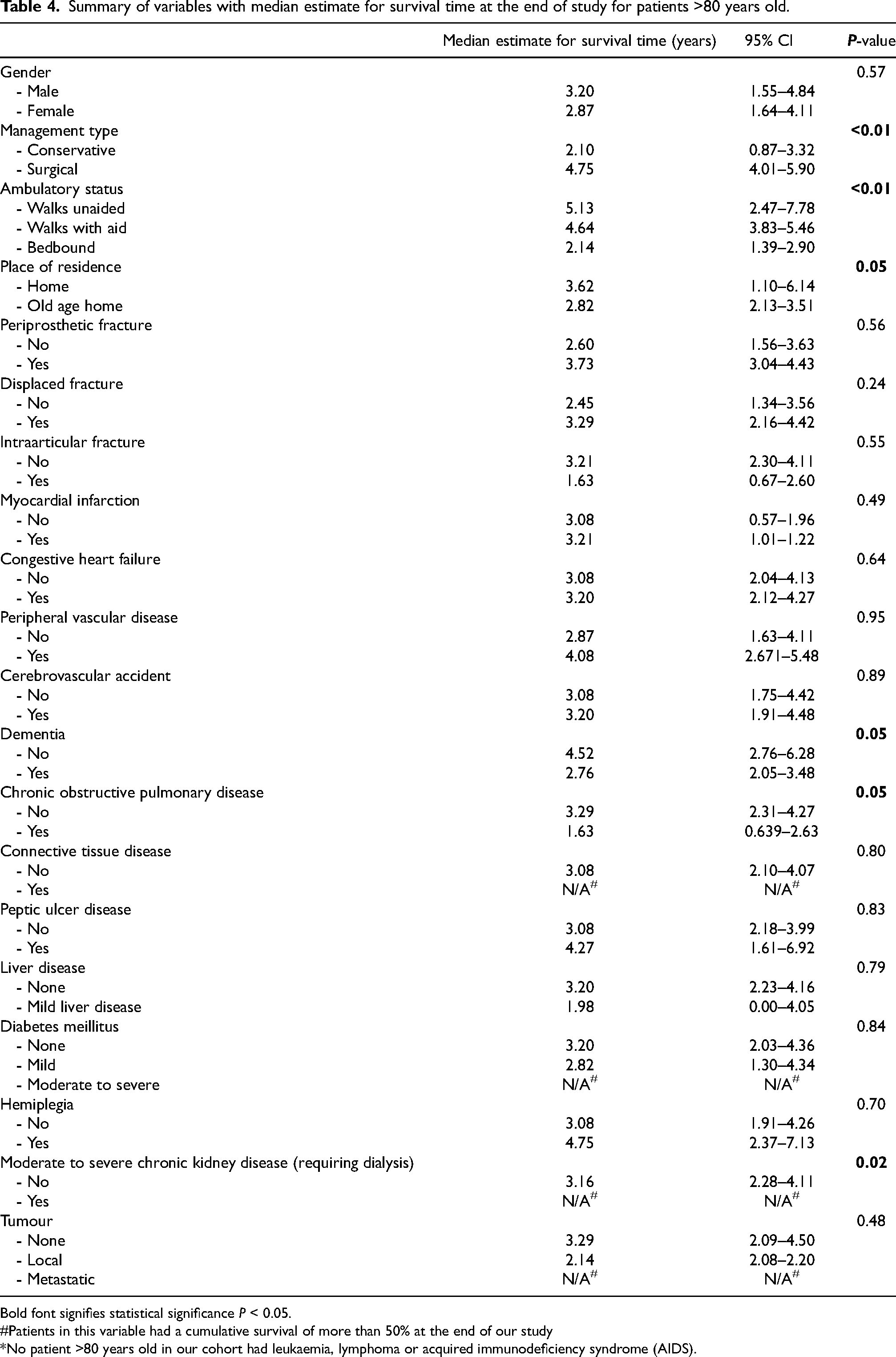
Bold font signifies statistical significance P < 0.05.
#Patients in this variable had a cumulative survival of more than 50% at the end of our study
*No patient >80 years old in our cohort had leukaemia, lymphoma or acquired immunodeficiency syndrome (AIDS).
Cox regression using the variables identified by the Kaplan-Meier analysis revealed that only management type, moderate CKD and COPD were factors affecting survival (Table 5). In patients older than 80 years old, those with surgical management will have a reduction in death hazard by 47% (CI 0.28–1.01, p = 0.05) compared to those without surgical management. For comorbidities analyzed, patients with COPD and moderate CKD show an increased death hazard by 2.61 times (CI 1.23–5.53, p = 0.01) and 7.17 times (CI 1.47–34.86, p = 0.02), respectively. Age, ambulatory status, place of residence and other comorbidities revealed no statistically significant increase in death hazards.
Predictors of mortalities with hazard ratios as per Cox regression analysis in patients >80 years old.
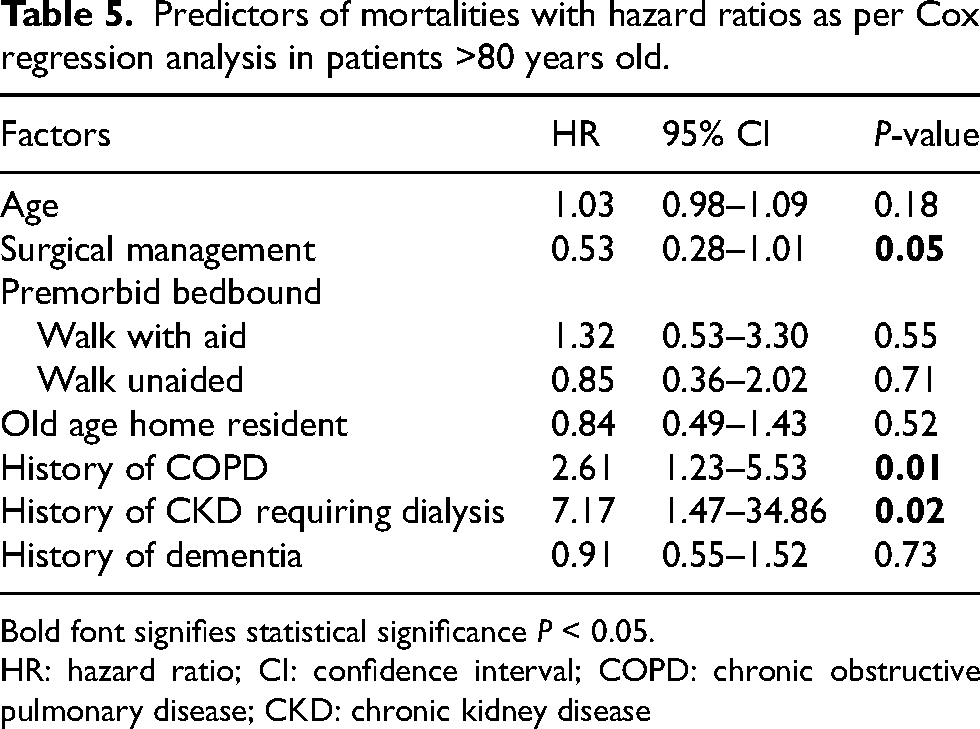
Bold font signifies statistical significance P < 0.05.
HR: hazard ratio; CI: confidence interval; COPD: chronic obstructive pulmonary disease; CKD: chronic kidney disease
Discussion
This was the first retrospective cohort study to determine the outcomes of patients with geriatric distal femur fractures in Hong Kong. We analyzed to understand the outcomes of those patients conservatively and surgically managed with potential variables that may affect the survival. Our primary parameter was mortality rate in this cohort. Our results show that the overall one-year mortality rate was 21.5%, which is comparable to previous studies. 9 Results showed that our cohort benefitted from surgical management with a cumulative median survival time of 5.98 years compared to those with conservative management of 2.32 years. The mean Charlson CI was similar in these two groups of patients, which means that the difference in cumulative survival could not be attributed to varying comorbidities patients may have.
We noted that there was an association between >80 years old chairbound patients and conservative management, which speaks to the current trend of managing such patients nonoperatively at our centre. To address a selection bias for conservative management due to age and ambulatory status and thus potentially resulting in higher survival in the surgical group, we analyzed patients >80 years old to determine the variables that affect survival. Overall, in this subgroup analysis, we found that there is a reduction in death hazard by 47% for those treated surgically compared to conservatively even in elderly patients who were >80 years old.
There was no significant difference in survival between the different statuses of ambulation and their premorbid place of residence in patients >80 years old. This is not particularly surprising as patients >80 years are likely affected by other more significant factors, such as medical comorbidities. This finding further supports our conclusion that elderly patients should be managed surgically regardless of their age, premorbid ambulatory status, and their place of residence. This is in keeping with previous findings 10 that surgically managed nonambulatory patients are less likely to have wound complications like dependent sores, supporting the case for surgical management even in bedbound patients.
Our analysis using the individual factors accounted for by the Charlson CI allows us to determine more precisely the comorbidities that may affect survival. In patients over 80 years old, we determined that the death hazard was increased by almost 2.61 times and 7.17 times in patients with COPD and moderate CKD, respectively. Our findings are in line with current literature that shows that those with multiple comorbidities as per other indices (e.g., Nottingham Hip Fracture Score) are associated with higher mortality rates. 11 Our study further looked specifically into individual predictors that may offer more insight into the specific selection of patients for surgical management, especially those who do not have COPD or CKD.
Interestingly, we found no significant difference in cumulative survival rates between periprosthetic and non-periprosthetic fractures with a median survival time of 4.27 years and 3.75 years, respectively. Previous studies showed that periprosthetic fractures had a higher survival rate likely attributed to a selection bias for surgical management. 8 In the present study, the survival time is slightly higher with patients with periprosthetic fractures albeit not significant. There was also no significant difference in survival time with displaced and intra-articular fractures compared to those without.
Strength and limitations
This study is to our knowledge the largest group of patients with geriatric distal femur fractures analyzed in Hong Kong. We included all types of distal femur fractures including periprosthetic fractures or not, allowing for appropriate subgroup analysis. Furthermore, we also looked into individual comorbidities (as per the Charlson CI) as predictors for mortality rates, which allowed us to definitively understand the interplay of specific comorbidities in the survival rate of patients with distal femur fractures. This guides our management by identifying those predictors that may improve survival in those patients whose management decisions remain controversial.
However, there are several limitations of this study. By design, it is difficult to determine causality given the retrospective nature of this study and hence limits interpretation of the results of this study. Furthermore, while some subgroups were large enough to be used to determine statistical significance, some subgroups were of limited sample size. Only preliminary inferences could be made from these data. As a result, future studies utilizing a randomized controlled design may be warranted for better and definitive delineation of the causality.
Conclusion
The current study is the largest retrospective cohort to date reported in Hong Kong with an overall one-year mortality rate of 21.5%. The results indicate that those receiving surgical intervention are associated with higher cumulative survival even when narrowed to octogenarians. Unfavourable factors that may contribute to a lower cumulative survival include history of COPD and CKD. In conclusion, there should a lower threshold for surgical intervention in those with distal femur fractures while taking consideration of specific favourable and unfavourable predictors that may affect survival.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.