
Abstract
Background:
Previous studies evaluating the epidemiology of pelvic ring fractures and predictors of mortality are largely based upon non-US populations, potentially limiting their generalizability. This study sought to analyze trends of pelvic ring fractures and associated complications in the United States using the largest and most recent national data set available. The specific aims of this study were to determine whether the incidence of pelvic ring fractures changed over time, whether in-hospital mortality following pelvic ring fracture changed over time, whether hospital length of stay following pelvic ring fracture changed over time, and whether there are independent predictors of in-hospital mortality, adverse events, or nonroutine discharge following pelvic fracture.
Methods:
The National Hospital Discharge Survey was queried to identify all patients admitted to US hospitals with pelvic ring fractures between 1990 and 2007. A cohort representative of 1 464 458 patients was identified, and multivariable logistic regression was used to find independent predictors of mortality, adverse events, and nonroutine discharge to another inpatient facility.
Results:
Between 1990 and 2007, the population-adjusted incidence of pelvic ring fractures increased from 27.24 to 34.30 per 100 000 capita (P < .001). Mortality declined from 4.2% to 2.8% (P < .001) paralleling an increase in the proportion of patients treated with surgical fixation (7.22%-10.36%). All forms of internal fixation were associated with decreased odds of mortality, while external fixation was associated with increased odds of mortality. Internal fixation was also associated with lower odds of adverse events and nonroutine discharge to inpatient facilities. The average in-hospital length of stay decreased from 11.2 days to 6.5 days (P < .001).
Conclusion:
This study provides the largest and most comprehensive epidemiologic analysis of pelvic ring fractures in the United States. Knowledge of the increasing incidence of pelvic fractures and prognostic factors associated with poor outcomes may improve outcomes.
Keywords
Introduction
Often the result of high-energy trauma in young individuals 1 –3 and low-energy injury in older people, 4 –7 pelvic ring fractures are associated with considerable morbidity, 8 –10 high mortality rates, 9,11 and significant cost to the society. 12,13 Estimates report the incidence of pelvic ring fractures between 2% and 8% of all fractures, 3,5,14 although the frequency may be as high as 25% in patients with multiple trauma. 3,15,16 Additionally, with an aging population, the burden of low-energy pelvic fractures will likely continue to affect a growing number of individuals. 17 –19 Recent advances in operative management of pelvic ring fractures have improved outcomes 1 and patient survival. 20 –22 Previous studies evaluating the epidemiology of pelvic ring fractures and predictors of mortality are largely based upon non-US populations, 1,3,5,9 potentially limiting their generalizability to patients in the United States. This study sought to describe the trends in incidence as well as factors influencing outcomes and complications for patients admitted to US hospitals with pelvic ring fractures using the National Hospital Discharge Survey (NHDS), the most recently available Centers for Disease Control and Prevention (CDC) data, which is also one of the largest inpatient databases in the United States. Knowledge of factors influencing outcomes of patients admitted with pelvic ring fractures may help improve management and decrease complications.
Methods
Data Source
The National Hospital Discharge Survey, developed by the National Center for Healthcare Statistics division of the CDC, 23 was used to estimate incidence and to evaluate risk factors for mortality and inpatient complications following pelvic ring fractures. The NHDS is the principal database used by the US Government for monitoring hospital use and is considered the most comprehensive of all inpatient surgical databases in use today. 24 The NHDS is a publically available survey providing demographic and medical data for inpatients discharged from nonfederal, short-stay hospitals in the United States. 24 The survey uses International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) codes 25 to classify medical diagnoses and procedures. The NHDS uses a stratified, multistage probability design to collect demographic information (age, gender, and race), expected source of payment (insurance status), medical information of up to 7 discharge diagnoses and up to 4 procedures, length of care, hospital size, US region, and inpatient outcomes including discharge destination. 26 The NHDS uses a complex 3-stage probability design to ensure an unbiased national sampling of inpatient records including inflation by reciprocals of the probabilities of sample selection and adjustment for no response and population weighting ratio adjustments. 24 This study did not require approval by the institutional review board because the NHDS is a publically available database with no patient identifying information.
Patient selection
All patients admitted to hospitals in the United States with a fracture of the pelvic ring between 1990 and 2007 were identified using ICD-9-CM codes. Discharges with a diagnosis code (ICD-9-CM) of closed or open fracture of the pubis (808.2 and 808.3), closed or open fracture of the ilium (808.41 and 808.51), closed or open fracture of the ischium (808.42 and 808.52), closed or open fracture of the sacrum/coccyx (805.6 and 805.7), multiple closed or open fractures of the pelvis (808.43,808.44, 808.53, and 808.54), or closed or open fracture of unspecified or other part of pelvis (808.49, 808.59, 808.8, and 808.9) were identified using previously described techniques. 27 The database was subsequently queried to identify patients treated using open reduction and internal fixation (ORIF; ICD-9-CM 79.30/79.39), closed reduction and internal fixation (CRIF; ICD-9-CM 79.10/79.19), external fixation (ICD-9-CM 78.10/78.19), or internal fixation without reduction (ICD-9-CM 78.50/78.59). Demographic variables were then collected including age, sex, primary diagnosis, associated diagnoses, type of fracture (open vs closed), prevalence of comorbidities, length of stay, and discharge destination. The incidence of complications was determined using the complication screening package. 28 The variable adverse event was created based on the following variables: wound complication (998.3), postoperative bleeding (998.1), acute postoperative infection (998.5), acute postoperative anemia (285.1), acute renal failure (584), acute myocardial infarction (410), pulmonary embolism (415.1), induced mental disorder (293), pneumonia (480-486), pulmonary insufficiency (518.5), deep venous thrombosis (453.4), intubation (96.xx), and transfusion of blood (99.x).
Statistical Analysis
Because of the large sample size, we assumed a normal distribution of the data. Differences between categorical variables were compared using the Pearson chi-square test, while the independent samples t test was used to compare differences between continuous variables. To determine independent predictors of a negative in-hospital outcome (death, adverse events, or discharge to inpatient facility), all variables present in at least 2% of the population 29 were included in a multivariable binary logistic regression model. A multivariable regression model isolates the effect of individual variables on inpatient outcomes, allowing for the control of potential confounders. For in-hospital adverse events, a 1% cutoff was used due to their lower rates of occurrence, as described previously. 30 The dichotomous variables were (1) death, (2) presence of adverse events, and (3) discharge to inpatient facility. Covariates accounted for in the regression model included gender, age, region of the country, and preexisting comorbidities (anemia, obesity, diabetes mellitus, hypertension, congestive heart failure, coronary artery disease, atrial fibrillation, prior myocardial infarction, and osteoporosis). To assess for the association between individual variables and inpatient outcomes, odds ratios and confidence intervals were calculated. Correcting for multiple comparisons, a P value of <.001 was used to define statistical significance, as described previously. 30 United States census data were used to obtain national population estimates for each year of the study 1990 to 2007. 31 Rates were presented as the number of pelvic ring fractures per 100 000 standard population. All data were analyzed using the software SPSS version 20 (Chicago, Illinois).
Source of Funding
No external funding source was used for the conduct of this study.
Results
Incidence and Demographics
A cohort representative of 1 464 458 patients with a diagnosis of pelvic ring fracture was identified between 1990 and 2007 (Table 1). In 1991, 67 997 cases (27.24 per 100 000 capita) of pelvic ring fractures were recoded, while in 2007, the number of cases increased to 103 310 or 34.30 per 100 000 capita (P < .001; Table 2). The mean age of patients with a pelvic ring fracture was 64.5 years (standard deviation [SD]: 25.6 years) and 69.7% were female (Table 1). The mean age of patients with a pelvic fracture significantly increased over the study period from 62.7 years to 67.7 years (Table 2). The most frequently associated diagnosis was fracture of the acetabulum (8.87%), followed by fracture of the femur (6.73%; Table 1). Of the total cohort, 6.27% underwent ORIF (Table 1). In 1991, 6.48% of patients with a diagnosis of pelvic ring fracture underwent ORIF, whereas 7.22% of patients underwent ORIF in 2007 (P < .001; Table 2). The proportion of older patients undergoing surgery increased from 5.8% to 15% in the 56 to 75 years cohort and from 13.6% to 39% in the over 75 years cohort. The average length of hospital stay was 8.0 days (SD 9.7 days) overall (Table 1). In 1991, the average length of stay was 11.2 days (SD 13.1) decreasing to 6.5 days (SD 7.1 days) in 2007 (P < .001; Table 2).
Characteristics of Patients With Pelvic Ring Fractures in the United States From 1990 to 2007.
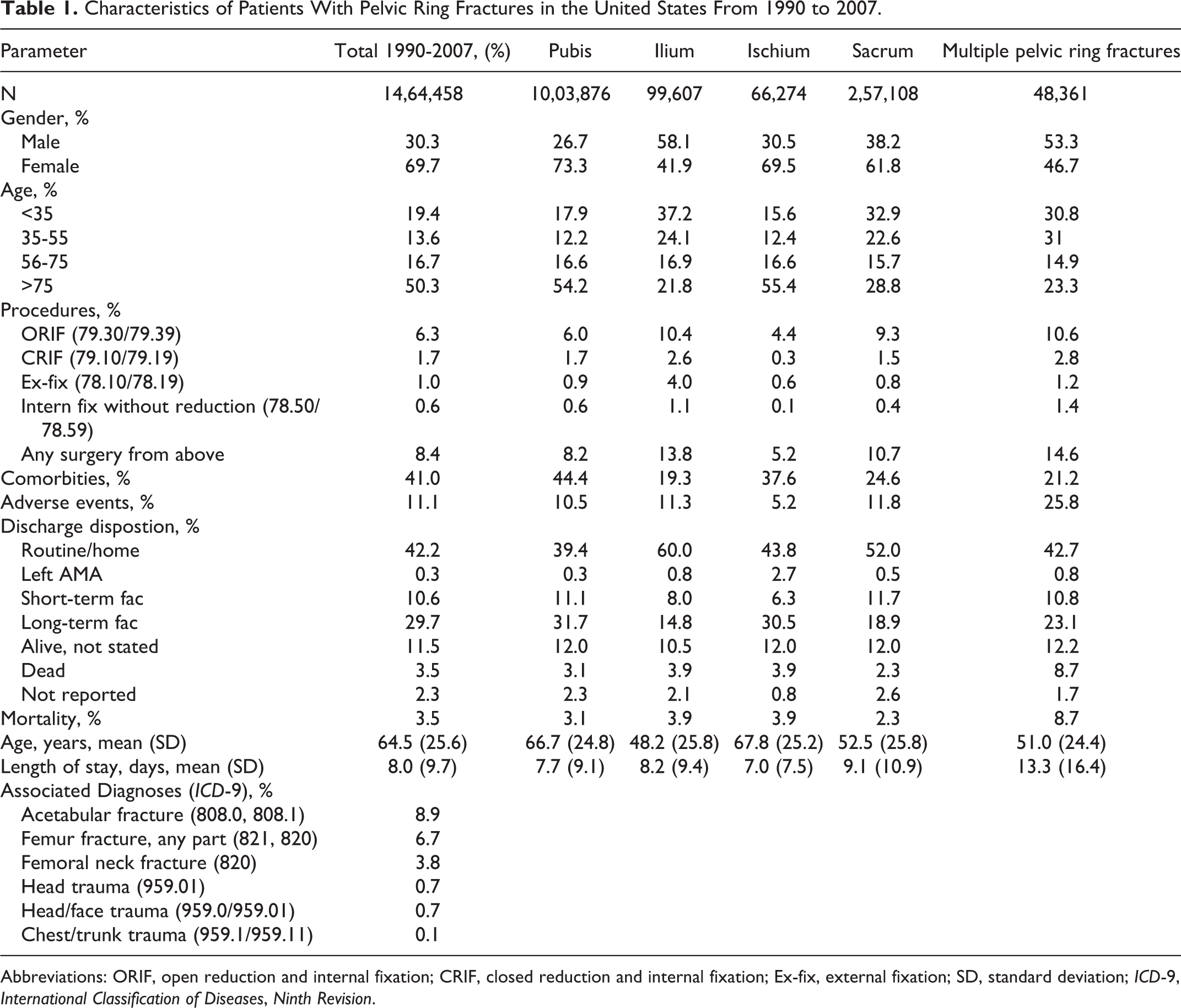
Abbreviations: ORIF, open reduction and internal fixation; CRIF, closed reduction and internal fixation; Ex-fix, external fixation; SD, standard deviation; ICD-9, International Classification of Diseases, Ninth Revision.
Patient Characteristics in 1990, 1995, 1999, 2003, and 2007 Among Patients With Pelvic Ring Fractures.
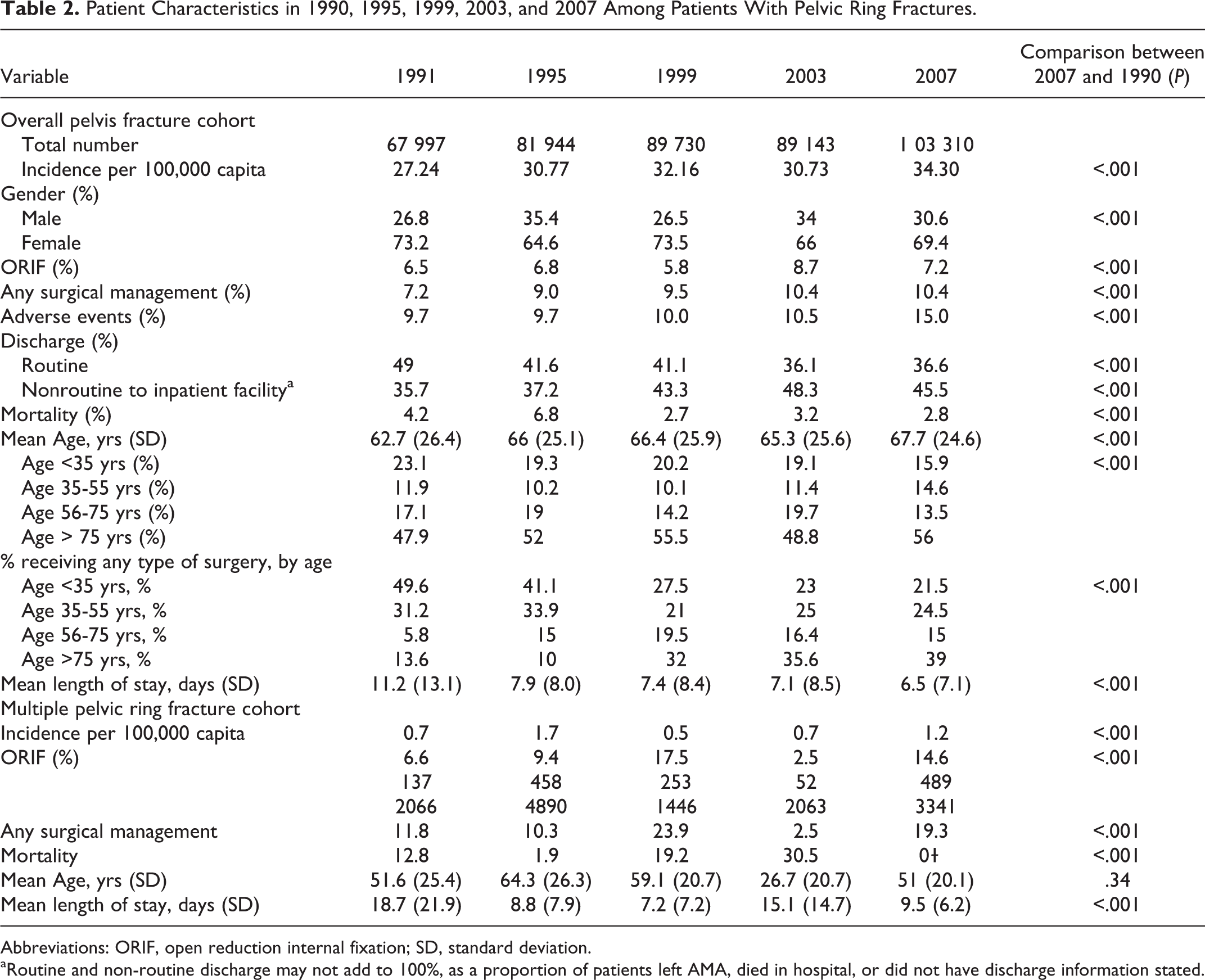
Abbreviations: ORIF, open reduction internal fixation; SD, standard deviation.
aRoutine and non-routine discharge may not add to 100%, as a proportion of patients left AMA, died in hospital, or did not have discharge information stated.
Mortality
In-hospital mortality decreased from 4.2% in 1990 to 2.8% in 2007 (P < .001; 3.5% for total cohort; Tables 1 and 2). Multivariable logistic regression analysis demonstrated any general in-hospital complication (OR 4.658, range: 4.557-4.761, P < .001), associated femur fracture (OR 3.524, range: 3.442-3.607, P < .001), and multiple pelvic ring fractures (OR 2.798, range: 2.707-2.891, P < .001) were associated with the highest odds of inpatient mortality. Treatment with external fixation (OR 2.281, range: 2.145-2.426, P < .001), male sex (OR 1.858, range: 1.825-1.892, P < .001), associated femoral neck fracture (OR 1.814, range: 1.749-1.880, P < .001), congestive heart failure (OR 1.766, range: 1.718-1.816, P < .001), or any surgery-related complication (OR 1.24, range: 1.195-1.286, P < .001) were also associated with increased odds of mortality. Treatment with ORIF (OR 0.658, range: 0.630-0.688, P < .001), CRIF (OR 0.105, range: 0.086-0.129, P < .001), or internal fixation without reduction (OR 0.217, range: 0.170-0.276) was independently associated with decreased odds of inpatient mortality (model fit: for omnibus test of model coefficients: χ2 = 11 590, P < .001, Nagelkerke R 2 = .310; Table 3).
Logistic Regression for Predictors of Mortality Among Patients With Pelvic Ring Fractures.a

Abbreviations: CI, confidence interval; OR, odds ratio; ORIF, open reduction and internal fixation; CRIF, closed reduction and internal fixation; M, male.
aN = 1 464 458. Omnibus χ2 = 11 590, P < .001, Nagelkerke R 2 = .310.
Comorbidities and Adverse Events
The prevalence of comorbidities and adverse events are listed in Tables 4 and 5, respectively. Hypertensive disease was the most common comorbidity (23.01%) followed by diabetes mellitus (8.96%). Overall, 11.09% of patients experienced an adverse event with the most common being postoperative anemia (6.13%) and blood transfusion (5.86%; Tables 1 and 5). The percentage of patients experiencing an adverse event increased from 9.65% in 1991 to 14.97% in 2007 (P < .001; Table 2). Multivariable logistic regression analysis revealed female gender (OR 3.697, range: 3.651-3.743, P < .001), osteoporosis (OR 2.820, range: 2.723-2.920, P < .001), hypertension (OR 1.801, range: 1.770-1.832, P < .001), diabetes mellitus (OR 1.592, range: 1.552-1.633, P < .001), coronary artery disease (OR 1.362, range: 1.313-1.414, P < .001), and age older than 75 years (OR 1.237, range: 1.221-1.252, P < .001) were associated with higher odds of inpatient adverse events. Compared with other types of pelvic ring fractures, fracture of the ischium (OR 1.851, range: 1.782-1.922, P < .001) and the pubis (OR 1.276, range: 1.260-1.292, P < .001) had higher odds of inpatient adverse events (model fit: for omnibus test of model coefficients: χ2 = 11 591, P < .001, Nagelkerke R 2 = .051; Table 6).
Prevalence of Comorbidities in Patients With Pelvic Ring Fractures Between 1990 and 2007.a
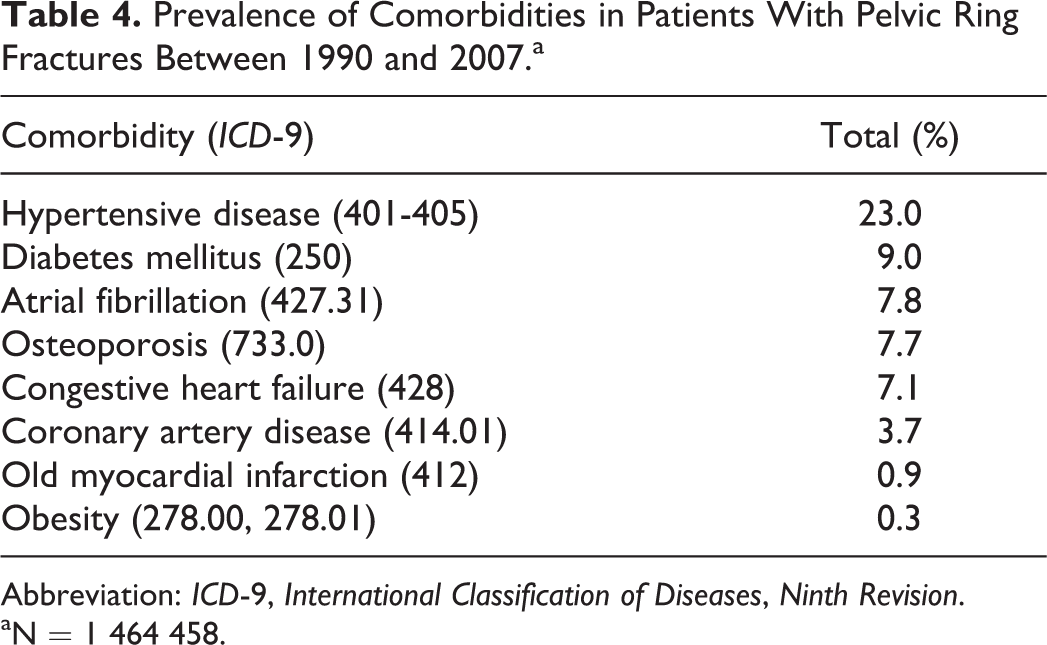
Abbreviation: ICD-9, International Classification of Diseases, Ninth Revision.
aN = 1 464 458.
Prevalence of Adverse Events Among Patients With Pelvic Ring Fractures Between 1990 and 2007.a
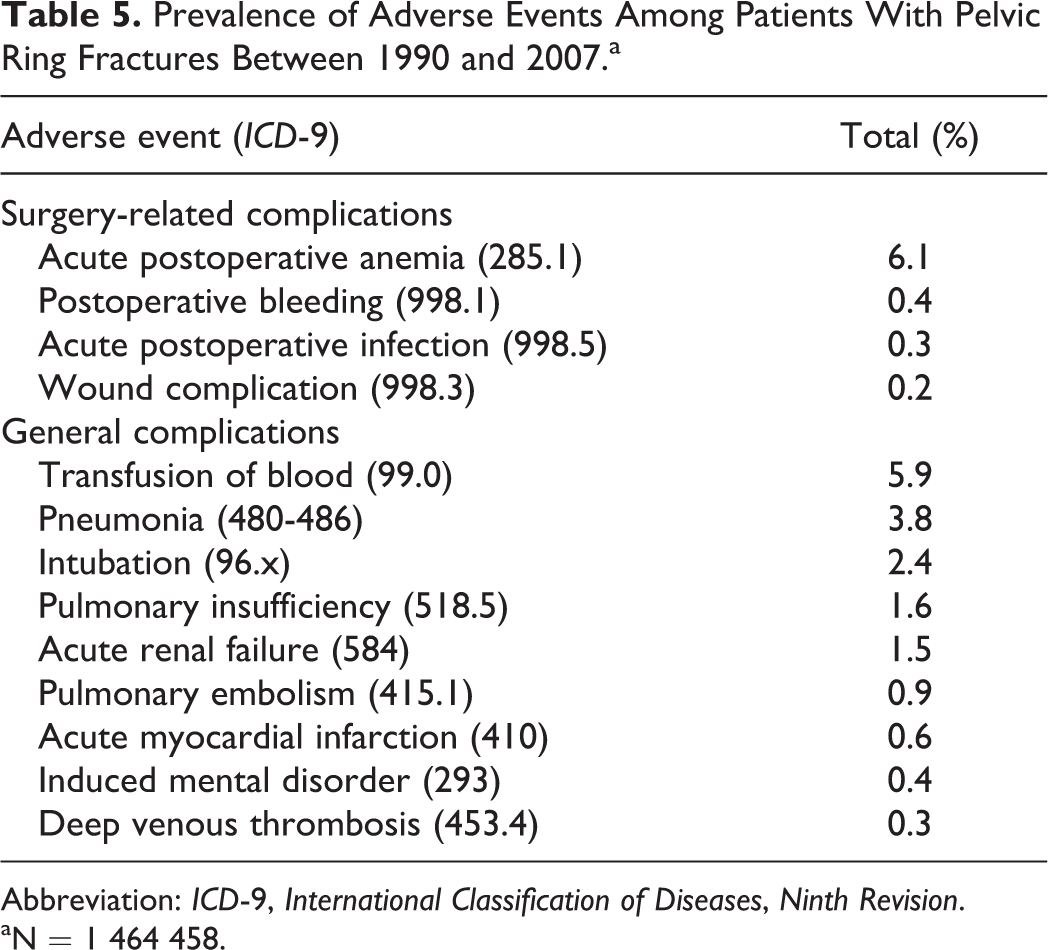
Abbreviation: ICD-9, International Classification of Diseases, Ninth Revision.
aN = 1 464 458.
Logistic Regression for Predictors of Adverse Events among Patients Hospitalized for Pelvic Ring Fractures.a

Abbreviations: CI, confidence interval; OR, odds ratio; ORIF, open reduction and internal fixation; CRIF, closed reduction and internal fixation; F, female; M, male.
aN = 1 464 458. Omnibus χ2 = 11 591, P < .001, Nagelkerke R 2 = .051.
Discharge Status
Over the 17-year study period, 40.3% of patients with pelvic ring fractures were discharged to another inpatient (short- or long-term) facility (Table 1). In 1991, 35.7% of patients were discharged to an inpatient facility, while in 2007, this percentage increased to 45.5% (P < .001; Table 2). Multivariable regression analysis demonstrated age older than 75 years (OR 4.497, range: 4.465-4.530, P < .001) and female gender (OR 2.585, range: 2.565-2.605, P < .001) were associated with the highest odds of discharge to an inpatient facility. Fracture of pubis (OR 1.405, range: 1.395-1.415, P < .001) was associated with higher odds of nonroutine discharge compared with fractures of other parts of the pelvic ring. In contrast, treatment with internal fixation without reduction (OR 0.332, range: 0.314-0.351, P < .001), ORIF (OR 0.818, range: 0.807-0.829, P < .001), or CRIF (OR 0.926, range: 0.902-0.950, P < .001) was associated with lower odds of nonroutine discharge. Age less than 35 years was associated with the lowest odds (OR 0.173, range: 0.171-0.175, P < .001) of nonroutine discharge to another inpatient facility (model fit: omnibus test of model coefficients: χ2 = 11 590, P < .001, Nagelkerke R 2 = .181; Table 7).
Logistic Regression for Predictors of Requirement for Discharge to Another Inpatient Facility Among Patients With Pelvic Ring Fractures.a

Abbreviations: CI, confidence interval; OR, odds ratio; ORIF, open reduction and internal fixation; CRIF, closed reduction and internal fixation; F, female; M, male.
aN = 1 464 458. Omnibus χ2 = 11 590, P < .001, Nagelkerke R 2 = .181.
Discussion
This study evaluated the incidence of pelvic ring fractures in the United States between 1990 and 2007 and identified prognostic factors associated with complications and death. The study demonstrated an increase in the population-adjusted incidence of pelvic fractures between 1990 and 2007 (27.24 cases per 100 000 capita to 34.30 cases per 100 000 capita). These rates are similar to the 23 per 100 000 reported by Balogh et al 5 in an Australian population but are higher than the rates reported by Chien et al (14.97 per 100 000) in Taiwan. 12 In addition, this study demonstrated that the average age of patients sustaining a pelvic fracture increased from 62.7 years in 1991 to 67.7 years in 2007.
In addition to national incidence, this study demonstrated that the proportion of patients with pelvic ring fractures treated with surgical fixation increased from 7.22% to 10.36% between 1990 and 2007. Concurrent with the increase in surgical fixation, there was a decrease in in-hospital mortality from 4.2% in 1991 to 2.8% in 2007. The rate of in-hospital mortality following pelvic ring fracture determined in this study is lower than the 4% mortality rate reported by Holstein et al 1 using the German Pelvic Trauma Registry and much lower than the rates reported by previous studies. 5,9,32 –38 Interestingly, the proportion of patients older than 75 years who underwent surgical fixation increased from 14% in 1991 to 39% in 2007. The improved survival rates may be due to advances in the operative management of pelvic ring fractures in which mechanical stabilization allows for early patient mobilization and facilitation of optimal nursing care. 1 As ORIF became the standard of care for pelvic ring fractures, 39,40 multiple reports have investigated operative timing and found early definitive fixation improves survival. 20 –22 This is similar to the findings of our study, which found ORIF to be associated with lower odds of mortality in multivariate logistic regression analysis. One must interpret these results with caution, however, as the NHDS only reports in-hospital mortality, whereas longer term follow-up may be closer to the 8% to 27% reported by others. 5,34,41 –43 Other explanations for the decreased mortality observed in this study include possible advances in patient care by intensivists. It is also possible that with the decreased length of stay and increased rate of nonroutine discharge to another inpatient facility observed in this study and that the NHDS is unable to detect a perioperative mortality that does not occur in the hospital.
Interestingly, this study found lower odds of mortality in patients older than 75. Prior studies have demonstrated an increase in the incidence of pelvic ring fractures in the elderly patients recently 7,44 and higher mortality rates when compared to younger patients with similar pelvic fractures. 45 –47 The finding that age older than 75 years was associated with lower odds of mortality may reflect the lower energy mechanism associated with pelvic ring fractures in elderly patients. 7,44,46,48 Male gender was associated with higher odds of in-hospital mortality. While a gender dimorphism of sex hormones and cytokine activity in response to hemorrhage and sepsis 1,49 may explain this result, it is also possible males have a greater tendency to be involved in higher energy accidents with more severe concomitant injuries.
Between 1990 and 2007, in-hospital days of care decreased from 11.2 days to 6.5 days. This decrease in length of stay is likely due to improved surgical technique and the implementation of early surgical intervention. 20,50 –52 Plaisier et al 22 demonstrated quicker return to baseline function, superior functional outcomes, and decreased length of stay in patients treated with early ORIF of their pelvis fractures. Additional benefits of early surgery include improved reduction in quality and ease of reduction 53 as well as control of bleeding, pain relief, and mobilization of the patient. 20 It is also possible the decreased length of stay correlates with the increased rate of discharge to other inpatient facilities, such as rehabilitation facilities, which was demonstrated in this study.
In contrast to decreasing in-hospital days of care, there was a rise in the number of adverse events between 1991 (9.65%) and 2007 (14.97%). Factors that may have contributed to increased adverse events include an aging population 54 and the growing diabetes epidemic, both of which were independently associated with higher odds of adverse events in this study.
Despite the strengths of using large, national databases for epidemiological research, 55 the present study has several limitations. Similar to other large databases, the NHDS is subject to coding error or errors in data entry. 56 Additionally, the database only allows for 7 diagnosis codes and 4 procedure codes per entry. As a result, the prevalence of comorbid conditions and adverse events may be underreported. 30 Given the frequency of associated injuries in high-energy pelvic trauma, this may have affected our ability to detect variables associated with poor outcomes in patients with pelvic fractures. Moreover, the severity of comorbid diseases cannot be appreciated when dichotomously classified as present or absent. 57 Similarly, due the limitations of diagnosis coding, the severity of pelvic ring fractures could not be determined. Previous studies have demonstrated higher mortality rates among patients with more severe pelvic injuries. 1,3,37,58 Temporal trends may also have affected the incidence data reported in this study. It is possible that during the study period, there was a pressure on hospital coders to capture more injuries. Additionally, diagnostic modalities have improved over time, and it is possible that a temporal detection bias exists between patients in the earlier years of the study and those in the later years, as the routine use of advanced imaging such as computed tomography and magnetic resonance imaging became more widely available. Another limitation is that the database only provides inpatient data, so complications that arise after discharge as well as follow-up data are unknown. Furthermore, the results of this study are limited to practice patterns in the United States from 1990 to 2007. The NHDS also does not specify the level of trauma center in which patients were treated. Future studies should evaluate trends in comparison between level 1 and level 2 or 3 trauma centers with regard to patient demographics, volume, and outcomes.
In conclusion, this study is the largest epidemiologic analysis of pelvic ring fractures in the United States and also provides predictors of in-hospital mortality, adverse events, and nonroutine discharge. The incidence of pelvic ring fractures in the United States is increasing, while mortality is decreasing. Identifying risk factors associated with poor outcomes has the potential to change treatment strategies, resource allocation, in-hospital monitoring, and discharge planning for this patient population.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.