
Abstract
Purpose:
Various surgical strategies including combined approach and spinal osteotomies in severe rigid scoliosis had been reported with significant perioperative complication rates. The use of single-staged posterior spinal fusion (PSF) utilizing a dual attending surgeon strategy for severe rigid scoliosis has not been widely reported.
Methods:
This was a retrospective study aimed to evaluate the perioperative outcome of single-staged PSF in severe rigid idiopathic scoliosis patients (Cobb angle ≥90° and ≤30% flexibility). Forty-one patients with severe rigid idiopathic scoliosis who underwent single-staged PSF were included. The perioperative outcome parameters were operation duration, intraoperative blood loss, intraoperative hemodynamic parameters, preoperative and postoperative hemoglobin, transfusion rate, patient-controlled anesthesia morphine usage, length of postoperative hospital stay, and perioperative complications. Radiological parameters included preoperative and postoperative Cobb angle, correction rate, side-bending flexibility, and side-bending correction index.
Results:
The mean age was 16.9 ± 5.6 years. The mean preoperative Cobb angle was 110.8 ± 12.1° with mean flexibility of 23.1 ± 6.3%. The mean operation duration was 215.5 ± 45.2 min with mean blood loss of 1752.6 ± 830.5 mL. The allogeneic blood transfusion rate was 24.4%. The mean postoperative hospital stay was 76.9 ± 26.7 h. The mean postoperative Cobb angle and correction rate were 54.4 ± 12.8° and 50.9 ± 10.1%, respectively. The readmission rate in this cohort was 2.4%. Four perioperative complications were documented (9.8%), one somatosensory evoke potential signal loss, one superficial infection, one lung collapse, and one superior mesenteric artery syndrome.
Conclusions:
Severe rigid idiopathic scoliosis treated with single-staged PSF utilizing a dual attending surgeon strategy demonstrated an average correction rate of 50.9%, operation duration of 215.5 min, and postoperative hospital stay of 76.9 h with a 9.8% perioperative complication rate.
Introduction
Scoliosis surgery is associated with serious perioperative complications. 1 –3 In severe rigid scoliosis, patient-related and curve-related factors could adversely affect the surgical outcome. Declining pulmonary function with increased curve severity could increase the likelihood of perioperative complications, whereas increased curve rigidity might necessitate the use of spinal osteotomies or combined approach. 4,5 Aggressive osteotomies, for example, vertebral column resection (VCR) led to longer operations and higher complication rates. 6 –9 The overall complication rate was 19.9% with 6.3% risk of new-onset neurological deficit, 4.0% risk of wound infection, and 1.4% risk of perioperative mortality. 10 Alternative approaches such as preoperative halo-gravity traction had also been widely studied. 11 –14 However, this approach required patients to have prolonged hospitalization which may not be cost-effective. 15
The use of single-staged posterior spinal fusion (PSF) utilizing dual attending surgeon strategy for severe rigid scoliosis had not been widely reported. This strategy could potentially mitigate the disadvantages of all other approaches. Therefore, we would like to report the perioperative outcome of this approach in our consecutive series of idiopathic scoliosis patients with severe rigid curves (Cobb angle ≥90° with ≤30% flexibility).
Methodology
This retrospective study was conducted in a single academic institution. Patients who were operated between January 2010 and March 2019 were recruited. This study was approved by our institutional ethical board.
The inclusion criteria were:
Patient with severe rigid idiopathic scoliosis with major curve Cobb angle ≥90° with flexibility ≤30% on physician-supervised supine side-bending (SSB) films.
All patients who underwent a single-staged PSF with pedicle screws using a dual attending surgeon approach.
For posterior releases, none of the patients underwent Grade 2 or more release based on the Schwab Osteotomy Classification. 16
Patients with complete records.
Exclusion criteria were patients who underwent preoperative halo-gravity traction; patients ≥40 years old or when the diagnosis of idiopathic scoliosis was unclear. During the study duration, there were 113 patients diagnosed with severe scoliosis. However, only 44 patients had major curve flexibility ≤30%. Two patients with preoperative halo-gravity traction were excluded. One patient who was more than 40 years old at the time of surgery was excluded.
Physician-supervised SSB film
In all cases, the SSB radiographs were supervised by a physician (orthopedic resident/spine fellow) who had received instruction and training on the bending films. To ensure maximum unbending of the major curve, trunk bending was performed passively by the physician in supine position. The physician would ensure the absence of pelvic rotation as well as maximum trunk bending. Cervical SSB radiographs were also performed at the same time by bending the cervical spine maximally. 17 Right and left side-bending films were performed. The patient was then instructed to maintain the position while the radiograph was captured.
The key perioperative outcomes were defined as below:
1. Estimated total blood loss: Total blood loss was estimated from the cell salvage system using this formula:
Total blood loss (mL): (Final volume accumulated in the reservoir) − (Total volume of anticoagulant citrate dextrose (ACD)) − (Total irrigation fluid used intraoperatively) + (Total unfiltered blood). The total volume of ACD and unfiltered blood (difference between weights of used and dry reservoir) was calculated while total irrigation fluid was measured intraoperatively.
Total blood loss did not include the volume of postoperative drainage from the subfascial drain.
2. Operation duration: Operation duration was calculated from the start of skin incision until the completion of skin closure.
3. Length of postoperative hospital stay: The duration of hospital stay was calculated from the time the operation was completed to the time of discharge.
4. Transfusion threshold: Transfusion threshold was hemoglobin level less than 80 g/L or when the patient was symptomatic.
The early radiographic data that was collected included:
1. Correction rate:
Correction rate (%): [(preoperative major Cobb angle − postoperative major Cobb angle)/preoperative major Cobb angle] × 100
2. Side bending correction index (SBCI):
SBCI = (correction rate/side-bending flexibility)
Other parameters, that is, demographic data, Lenke types, number of fusion level, screw density, intraoperative hemodynamic parameters using arterial blood gas, preoperative and day 2 postoperative hemoglobin, allogeneic blood transfusion rate, total patient-controlled analgesia (PCA) morphine used, as well as any perioperative complications (within 30 days postoperation) were also documented.
Selection of fusion level
Selection of the upper instrumented vertebra (UIV) was guided by the cervical SSB radiographs. By using these side-bending radiographs, the optimal UIV tilt angle was calculated. 18 The selected UIV would be the most distal vertebra with a favorable UIV tilt angle and a good proximal compensatory ability. Lowest instrumented vertebra (LIV) was selected based on the last vertebra substantially touched by the central sacral vertical line in a standing radiograph. If the LIV was L4 vertebra, an SSB film was used to determine if a more proximal level could be chosen. L3 vertebra would be selected as the LIV of choice if the L3 vertebra was bisected by the central sacral line in the preoperative SSB radiograph. 19
Surgical technique
Intravenous tranexamic acid was administered prior to skin incision. Alternate level screw placement strategy was used. By convention, there would be 3–4 base anchors. Proximally, the number of screws would depend on the amount of correction that was needed (commonly involving the proximal thoracic curve) and the strength of the screws (commonly extrapedicular screws were used due to the dysplastic pedicles). For facet resection, the entire inferior articular facet and the inferior portion of the lamina would be resected using an osteotome or rongeur to expose the superior articular facet and the ligamentum flavum centrally. The ligamentum flavum would then be thinned out without exposing the epidural space (Figure 1). Ponte osteotomies, pedicle subtraction osteotomies (PSOs), or VCR were not performed. Reduction was performed using translational or rod derotation techniques (Figure 2). Three-rod technique was used when the apex of the major curve demonstrated a very acute change of direction which might necessitate acute rod bending (Figure 3). Fusion was augmented using local bone graft harvested from spinous processes, laminae, transverse processes, and facet joints in all patients. None of the patients required allografts or bone substitutes. A subfascial drain was inserted prior to closure. Subcutaneous bupivacaine was infiltrated before skin closure.

Radical facet release exposing the superior articular facet (white arrow) and the deep layer of ligamentum flavum (black arrow).
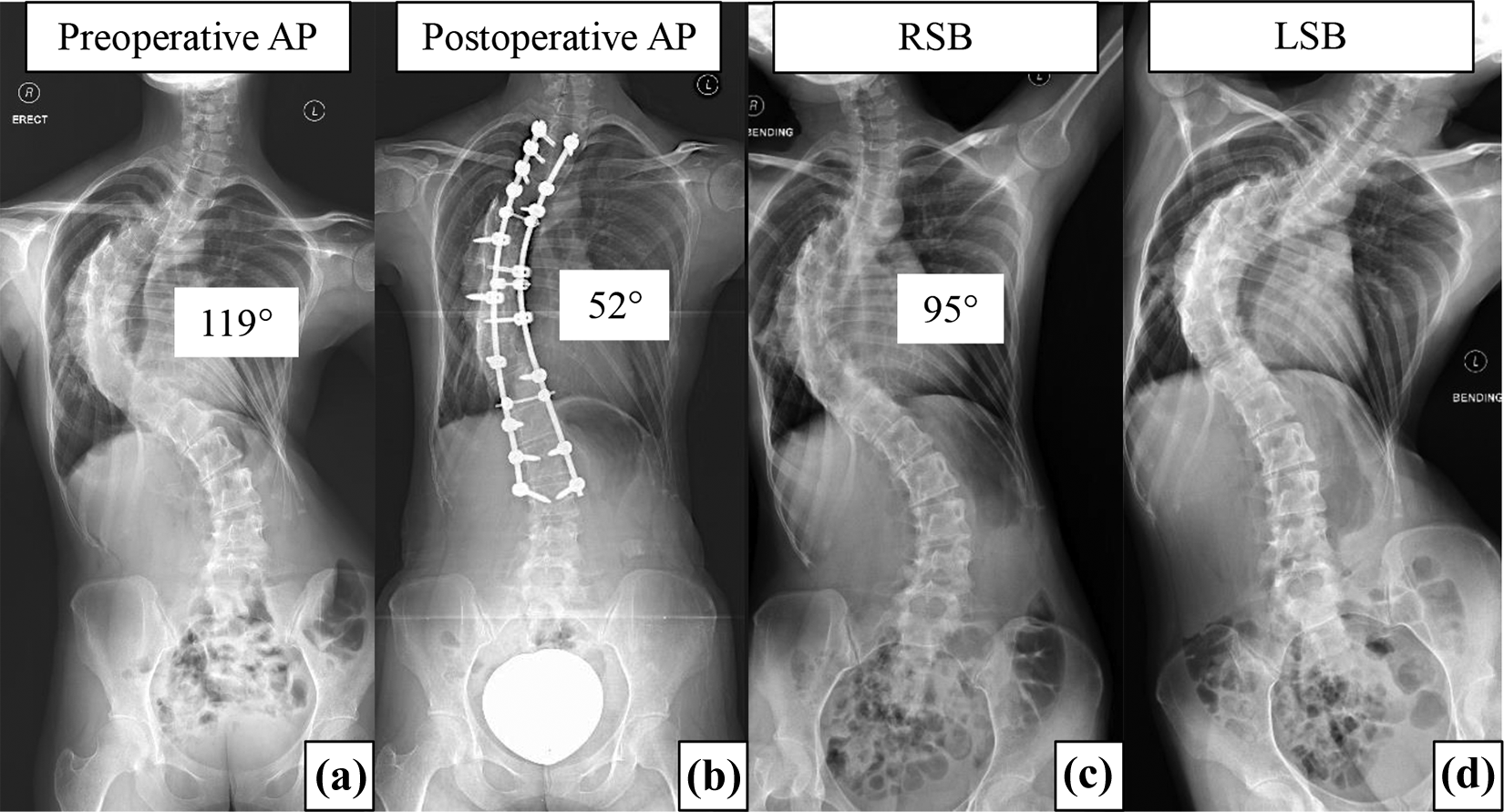
Patient no. 20: A 22-year-old presented with severe rigid scoliosis with preoperative Cobb angle of 119° and flexibility of 20.1% (a), (c), and (d) underwent single-staged PSF with two-rod technique from T2 to L3. Postoperative Cobb angle was 52° and correction rate was 56.3% (b). AP: anteroposterior; RSB: right side bending; LSB: left side bending; PSF: posterior spinal fusion.
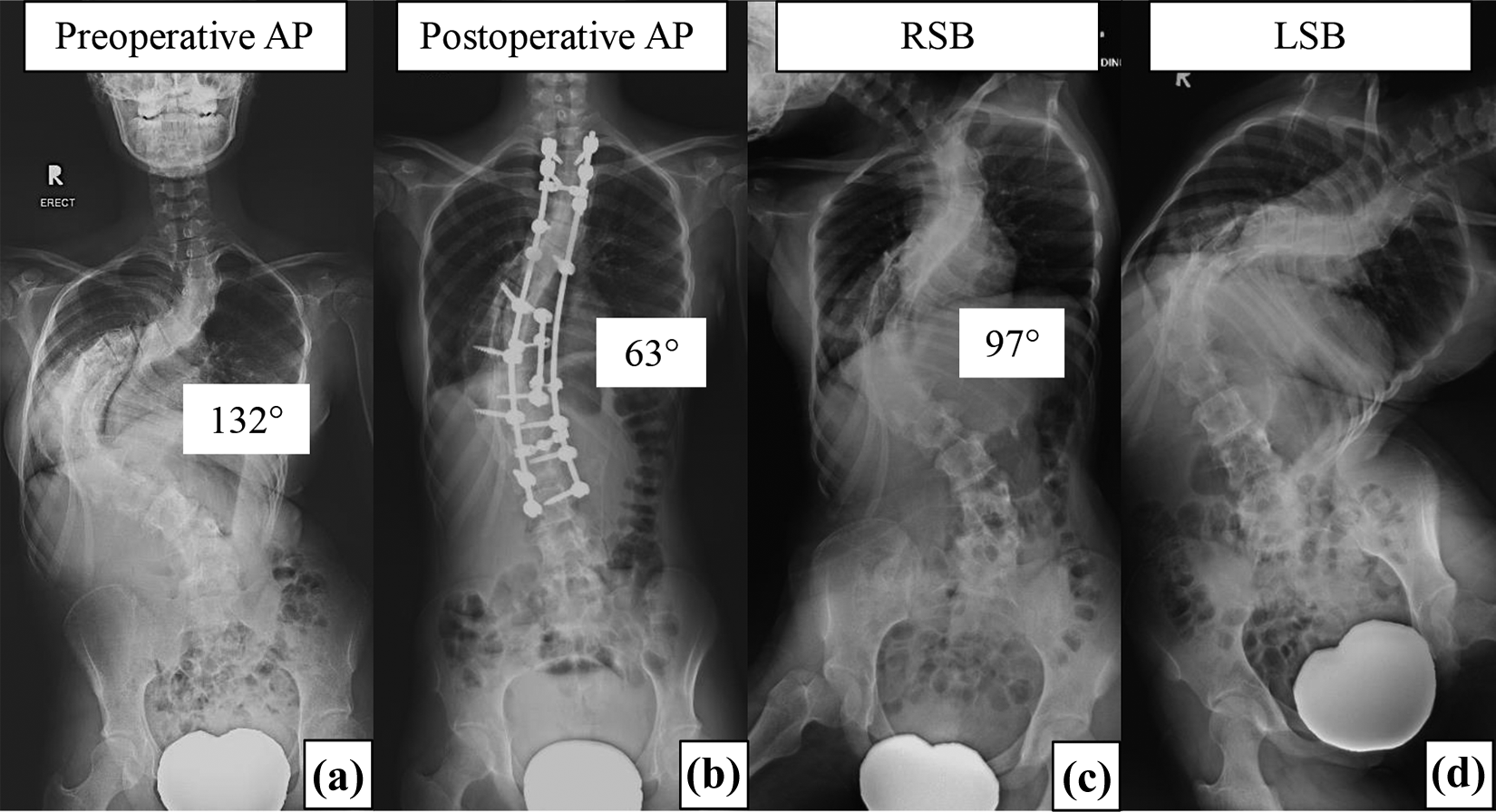
Patient no. 40: A 16-year-old girl presented with severe rigid scoliosis with preoperative Cobb angle of 132° and flexibility of 26.5% (a), (c), and (d) who underwent single-staged PSF with three-rod technique from T2 to L3. Postoperative Cobb angle was 63° and correction rate was 52.3% (b). AP: anteroposterior; RSB: right side bending; LSB: left side bending; PSF: posterior spinal fusion.
Postoperative protocol
Patients received intravenous morphine PCA, which was provided for 24–48 h postoperatively and was discontinued once consumption was less than 5 mg/24 h. Oral celecoxib (Celebrex) 200 mg once/twice daily and acetaminophen tablets 500–1000 mg six hourly were commenced. Breakthrough pain was managed with oxycodone hydrochloride (OxyNorm) capsule 5 mg. Postoperative hemoglobin was checked 48 h postoperatively.
Accelerated recovery protocol was employed. 20 Subfascial drain was removed within 18–24 h with a maximum drainage of 200 mL. Continuous bladder drainage was removed at the same time. This allowed early ambulation for the patients. Whole spine erect radiographs were performed 24–48 h postoperatively. Patients were discharged once pain score (VAS) <4/10, tolerating orally, ambulating, and surgical wound was dry.
Statistical analysis
All data were analyzed using the SPSS version 23.0 (IBM SPSS Statistics for Windows, IBM Corp., Armonk, NY, USA). Demographic variables were analyzed using descriptive statistics. Continuous variables were analyzed using Student t-tests. Categorical variables were analyzed using χ 2 test. Pearson’s correlation test was used to examine the correlation between numerical variables. All p values were two-tailed and statistical significance was set at 0.05.
Results
Forty-one patients (92.7% females) were included. The mean age of patients was 16.9 ± 5.6 years. The mean preoperative Cobb angle was 110.8 ± 12.1° with SB flexibility of 23.1 ± 6.3% (Table 1).
Demographic and preoperative data of patients with severe rigid scoliosis.
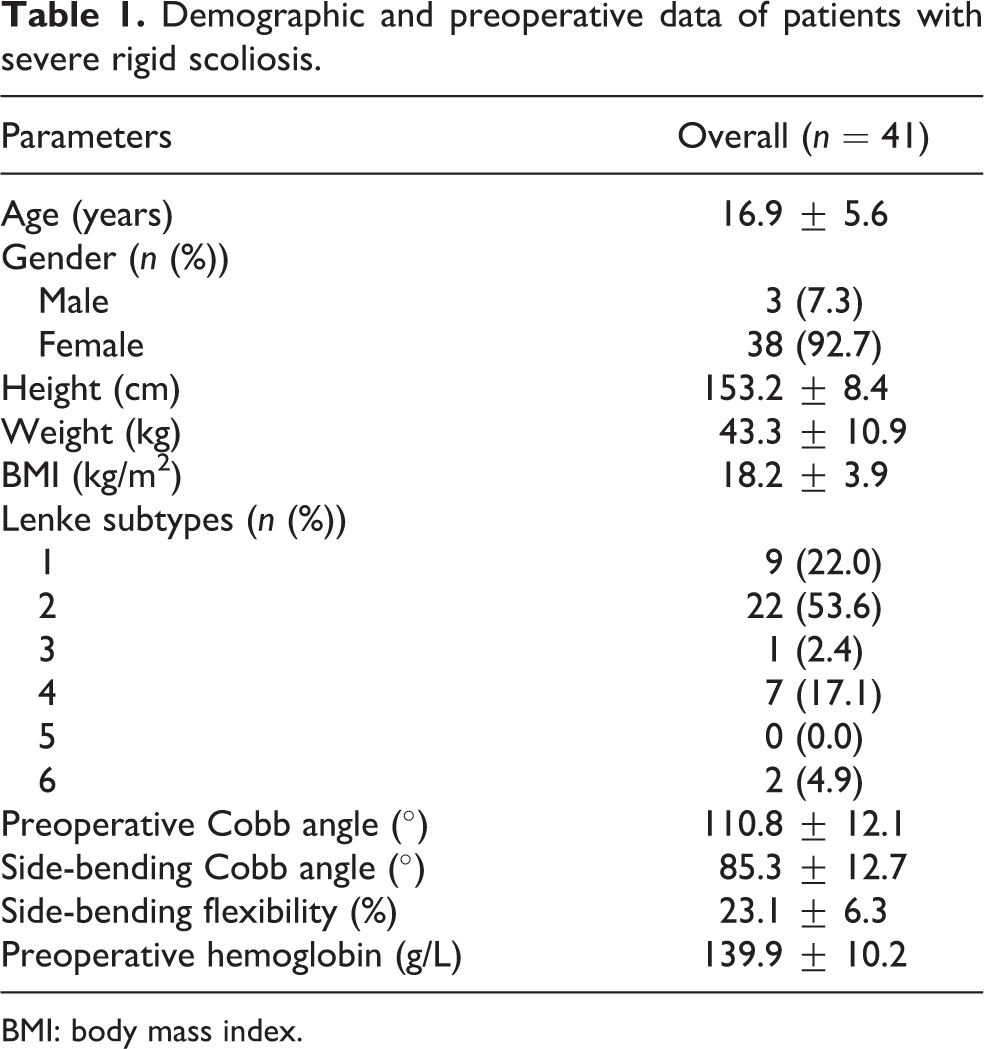
BMI: body mass index.
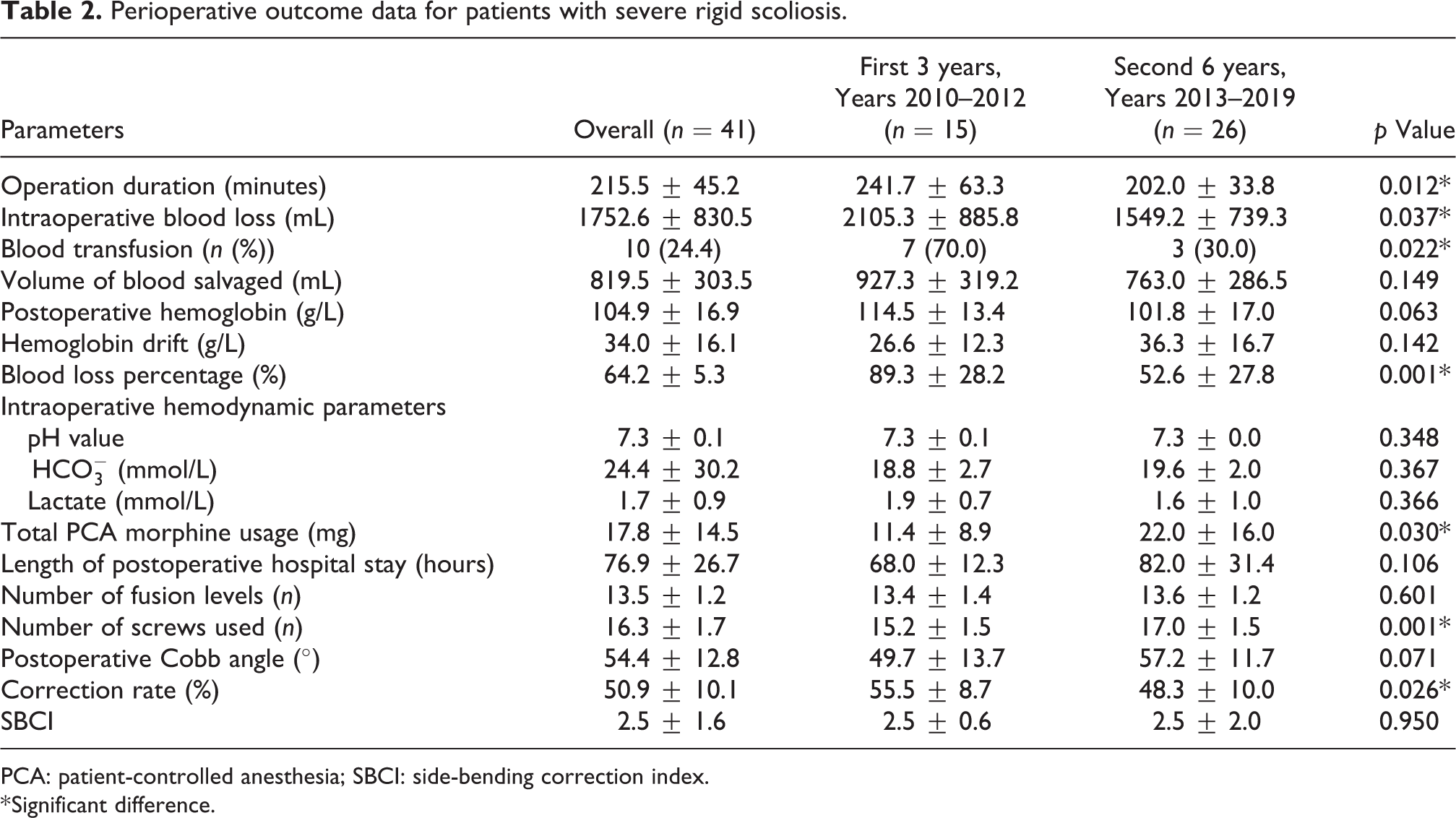
The mean postoperative Cobb angle was 54.4 ± 12.8° with a mean correction rate of 50.9 ± 10.1% and a mean SBCI of 2.5 ± 1.6. The average operation duration was 215.5 ± 45.2 min. The mean blood loss of 1752.6 ± 830.5 mL while mean blood loss percentage was 64.2% per body volume. Ten patients (24.4%) received allogeneic blood transfusion. Day 2 postoperative hemoglobin was 104.9 ± 16.9 g/L with mean hemoglobin drift of 34.0 ± 16.1 g/L. The average total PCA morphine usage was 17.8 ± 14.5 mg. The mean postoperative hospital stay was 76.9 ± 26.7 h (Table 2).
Perioperative outcome data for patients with severe rigid scoliosis.
PCA: patient-controlled anesthesia; SBCI: side-bending correction index.
* Significant difference.
We compared the differences between first 3 years (years 2010–2012) and second 6 years (years 2013–2019) of the study period as there might be variations in surgical techniques and surgeons’ experiences over a span of 9 years. There were significant differences in operation duration, intraoperative blood loss, allogeneic transfusion rate, blood loss percentage, total PCA morphine usage, number of screws used, and correction rate between both periods. The mean operation duration was 241.7 ± 63.3 min and 202.0 ± 33.8 min in the first and second period, respectively (p = 0.012). The mean blood loss was 2105.3 ± 885.8 mL and 1549.2 ± 739.3 mL in the first and second period, respectively (p = 0.037). In the second period, three patients required allogeneic blood transfusion compared to seven patients in the first period (p = 0.022). Blood loss percentage was higher in the first 3 years (89.3 ± 28.2% versus 52.6 ± 27.8%, p = 0.001). Total PCA morphine usage was lower in the first 3 years (11.4 ± 8.9 mg versus 22.0 ± 16.0 mg, p = 0.030). Number of screws used was slightly higher in the second period (17.0 ± 1.5 screws versus 15.2 ± 1.5 screws, p = 0.001). However, the correction rate was lower in the second period (48.3 ± 10.0%) compared with 55.5 ± 8.7% in the first period (p = 0.026; Table 2).
Table 3 demonstrated the radiological parameters, intraoperative parameters, and complications of all patients in the cohort. There was no significant correlation between blood loss and Cobb angle (p = 0.491), between operation duration and Cobb angle (p = 0.122) and between blood loss and operation duration (p = 0.053) (Figure 4). Furthermore, there was no significant correlation between length of hospital stay and blood loss (p = 0.701), blood transfusion (p = 0.585), and operation duration (p = 0.941) (Figure 5).
Data of the patients.

Preop: preoperative; postop: postoperative; CR: correction rate; op.: operation; SSEP: somatosensory evoked potential; SMA: superior mesenteric artery.
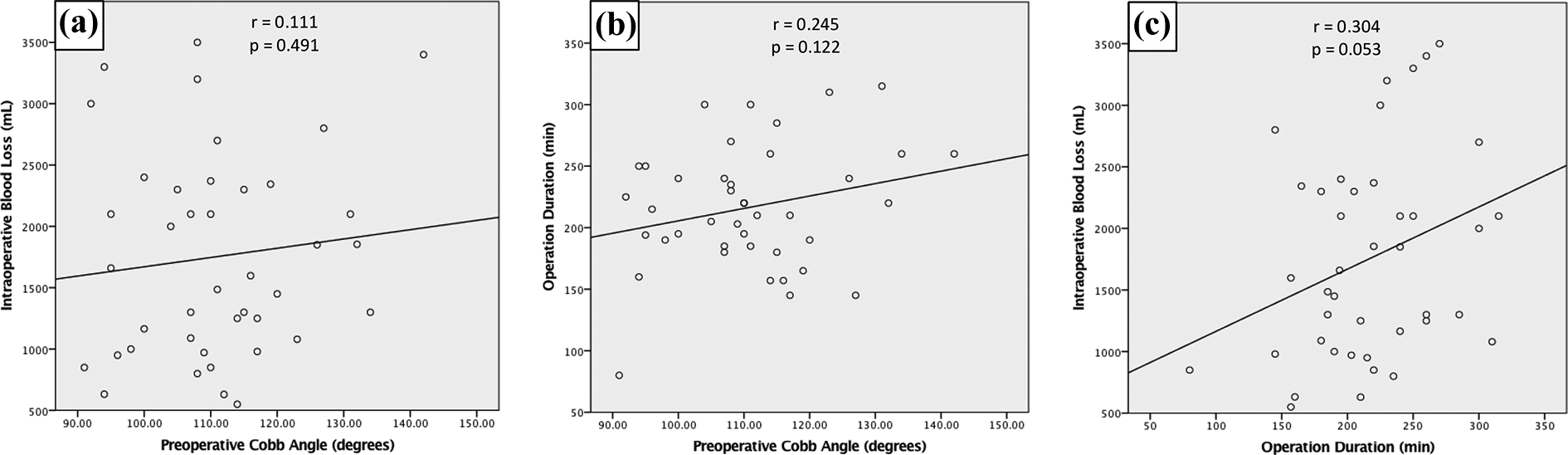
Correlation study between intraoperative blood loss and preoperative Cobb angle (a), operation duration and preoperative Cobb angle (b), and intraoperative blood loss and operation duration (c).
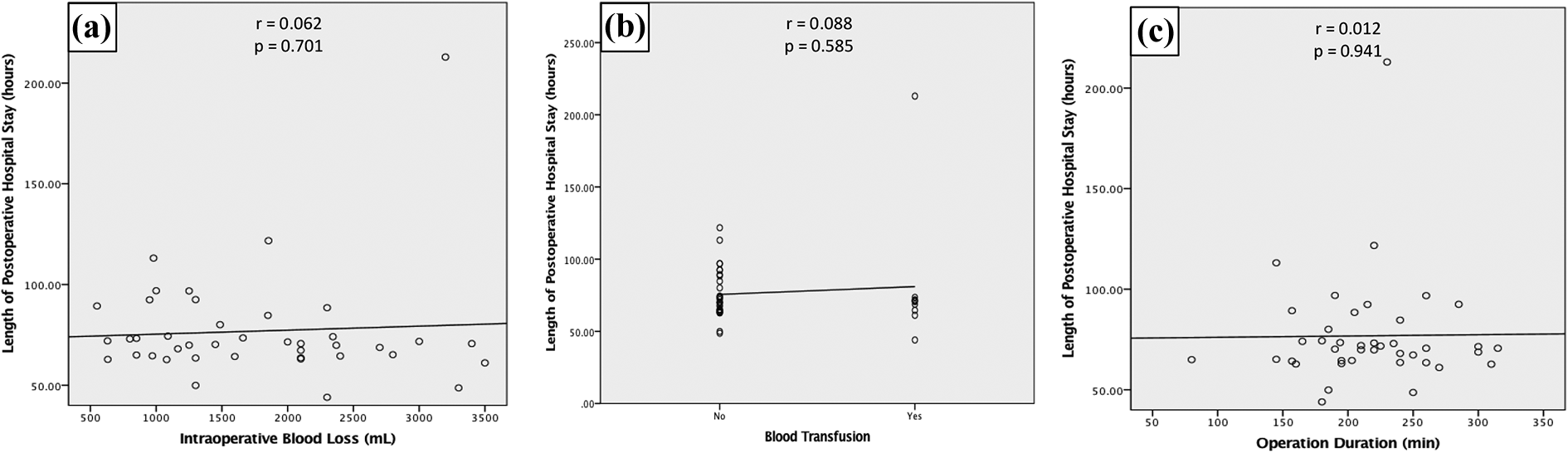
Correlation study between intraoperative blood loss (a), blood transfusion (b), and operation duration (c) with length of postoperative hospital stay.
The readmission rate was 2.4% (1/41). Four perioperative complications were documented (9.8%). One patient had somatosensory evoked potential signal loss during scoliosis correction. The signal returned to normal upon rod removal. After reducing the correction magnitude, there was no signal loss subsequently. Postoperatively, the patient had normal neurological function.
One patient developed lung collapse at day 2 postoperatively. Chest radiograph showed the collapse of right middle and lower lobes. Her condition improved after intensive chest physiotherapy and oxygen supplementation and was discharged well at day 6 postoperatively (Figure 6).

Patient no. 37: A 13-year-old girl with severe rigid scoliosis with preoperative Cobb angle of 117° (a) underwent PSF from T2 to L2. Postoperative Cobb angle was 60° and correction rate was 48.7% (b). She developed lung collapse of right middle lobe at postoperative day 2 (white arrow) (c) which resolved at postoperative day 6 with noninvasive oxygen supplementation and chest physiotherapy. AP: anteroposterior; PSF: posterior spinal fusion.
One patient had superior mesenteric artery (SMA) syndrome which developed at day 7 postoperatively. Plain abdominal radiograph showed double bubble sign. Computed tomography (CT) abdomen showed dilated stomach and first and second part of duodenum. CT angiogram revealed SMA-aorta angle of 10° and SMA-aorta distance of 2.6 mm. She was treated conservatively with gastric decompression via nasogastric tube, correction of electrolytes, and nutritional support. She responded well and was discharged at day 26 postoperatively (Figure 7).
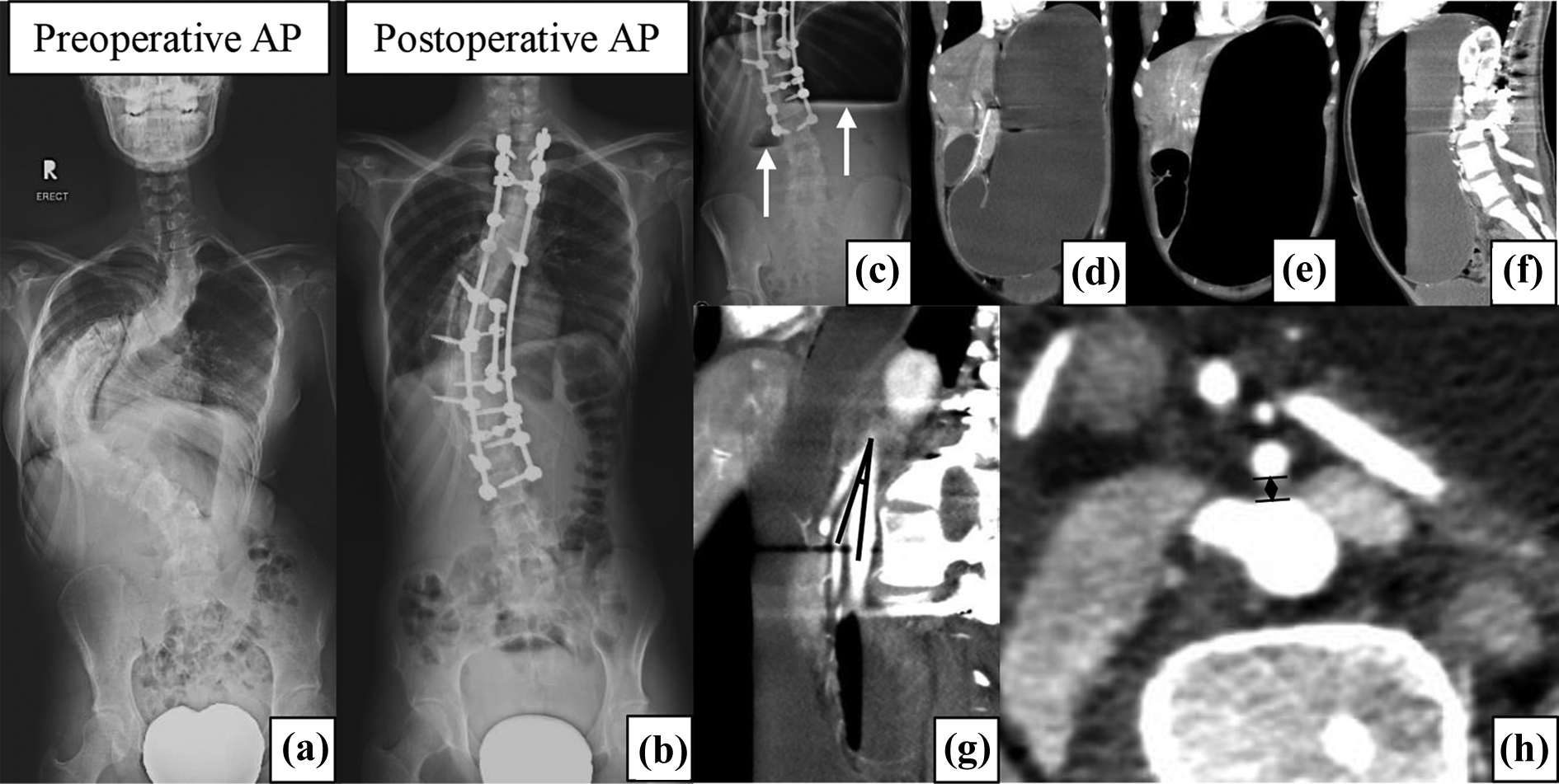
Patient no. 40: A 16-year-old girl with severe scoliosis underwent PSF from T2 to L3 (a) and (b) and developed SMA syndrome at postoperative day 7. Erect abdominal radiograph showed double bubble sign (white arrow) (c). CT abdomen showed dilated stomach and first and second part of duodenum (d) to (f). CT angiogram showing decreased SMA-aorta angle of 10° (g) and SMA-aorta distance of 2.6 mm (h) confirmed the diagnosis of SMA syndrome. AP, anteroposterior; SMA: superior mesenteric artery; PSF: posterior spinal fusion; CT: computed tomography.
There was one superficial infection at the proximal aspect of the wound. The patient underwent dressing and the wound was approximated using adhesive strips. The wound healed well. Culture was negative.
Discussion
Many studies reported the outcome of treatment for severe rigid scoliosis. 6 –8,21 –25 To have a valid comparison, the definition of severe rigid scoliosis was important. Three studies used Cobb angle ≥90° as their criteria of severe scoliosis, 21,23,24 whereas another three studies used Cobb angle ≥80°. 7,8,22 Kandwal et al. used a cutoff of 100° 6 . The assessment of curve rigidity was even more confusing. Although most authors considered flexibility ≤30% as rigid scoliosis, there was lack of standardization on the method of flexibility assessment. In three studies, the method of flexibility assessment was not well described, 7,21,25 whereas in another article, the authors described SSB as their flexibility assessment method but the case illustration in that article showed the use of standing side bending 6 (Table 4).
Literature review with criteria of severe rigid scoliosis and surgical techniques.

PSO: pedicle subtraction osteotomy; VCR: vertebral column resection; NA: not available; AIS: adolescent idiopathic scoliosis.
There was conflicting evidence on what was deemed the most accurate method to assess the curve flexibility. Tokala et al. studied 80 patients and reported traction radiographs under general anesthesia were more predictive than fulcrum bending (FB) radiographs. 26 Bekki et al. compared supine with prone SB radiograph and found both to be similar. 27 Khodaei et al. in a systematic review concluded that FB provided the best estimates for curves >45º but the quality of evidence was very low to low with moderate risk of bias. 28 He and Wong found that traction should be considered for severe curves. 29 However, to the best of our knowledge, there had been no study that evaluated the flexibility of curves ≥90º using the various flexibility radiographs. In our center, we modified the conventional SSB by having the procedure supervised by a physician. This would ensure standardization of the assessment process as maximal bending would be performed.
In complex spinal deformities, the curve magnitude and the use of osteotomies increased the risk of complications. In a review of 145 pediatric spinal deformities, the authors introduced a scoring system Foundation of Orthopedics and Complex Spine (FOCOS level) that included these two factors and found that the FOCOS level correlated with blood loss, operation duration, and complication rate. 30 Suk et al. in his study on single-staged VCR in 16 patients, reported 3 major complications; 1 had acute complete paralysis, 1 had hematoma, and 1 had hemopneumothorax. 7 Riley et al. reviewed 109 patients who underwent posterior VCR for severe spinal deformity. Out of 54 patients who were available for analysis, 30 patients (55.6%) developed postoperative complications with 5 (9.3%) sustained postoperative neurological deficits. 31 Lenke et al., in a multicenter study of 147 pediatric patients who underwent VCR, documented a 59% complication rate, with 27% rate of intraoperative neurological events. 32 Yamin et al. reported the outcome of PSO in 21 patients with 2 major complications, 1 had temporary paraplegia requiring decompression surgery and 1 had permanent neurological deficit. 22
Other authors employed a combined anterior–posterior approach for severe rigid scoliosis. Pulmonary complications were commonly encountered. Kandwal et al. reported two patients who had basal atelectasis and prolonged chest drainage. 6 Bullmann et al. reported a case of postoperative pleural effusion. 8 Shen et al. documented one pneumonia and one pneumothorax. 21 In addition, combined approaches also prolonged hospital stay. Bullmann et al. reported a hospital stay of 15 days. 8 Shen et al. reported a length of stay of 18.4 days in a single-staged approach compared to 32.7 days when the combined procedure was performed in two stages. 21
In comparison, we reported a mean postoperative hospital stay of only 3.2 days. A standardized accelerated recovery protocol was employed in all patients. 20 This approach standardized the postoperative care and therefore shortened the length of stay. Among the major complications that we encountered, one patient had lung collapse that required an additional 3 days of hospital stay. Another patient experienced SMA syndrome who had to be readmitted for 3 weeks but she recovered fully without additional surgery. The complication rate in our series was one of the lowest (9.8%) among other reports (9.5–33.3%). This could probably be due to the surgical approach and the dual attending surgeon strategy used in our institution which would reduce operation duration leading to a shorter hospital stay.
However, it is important to note that our correction rate was the lowest (Table 5). A long-term clinical study would be needed to evaluate the outcome of higher versus lower correction rate. While the correction rate was modest, the shorter operation and fewer complications of a less-aggressive approach described in our study may outweigh the benefits of the additional correction. Moreover, in severe rigid scoliosis, the correction reported was only over the major curve. In principle, a harmonious correction which considered the stiffness of the proximal thoracic, main thoracic, and lumbar curves to achieve better shoulder and trunk balance was probably more important. Some authors reported that, in patients with high implant density, a significantly better correction rate could be achieved; however, there was no difference in the postoperative coronal balance and trunk shift. 33 In contrast, Shen et al., in a retrospective study of 62 adolescent idiopathic scoliosis (AIS) patients who underwent PSF, found that there was no significant difference in the correction rate of the main thoracic curve between the low and high implant density groups. 34
Literature review of preoperative Cobb angle, flexibility, length of postoperative hospital stay, correction rate, and complication.

VDS: ventral derotation spondylodesis; MEP: motor-evoked potential; SSEP: somatosensory evoked potential; SMA: superior mesenteric syndrome.
The involvement of two attending surgeons distinguishes the current study from previous reports. The presence of a second attending surgeon might increase the total surgical cost, but the overall benefit, that is, (1) reduction of complication rates and (2) restoration of function in patients who may live (and work) for another 60–70 years, outweighs the cost. In a multicenter study involving 242 AIS patients, Merola et al. assessed the functional outcome for AIS patients 2 years after surgery using the Scoliosis Research Society Questionnaire, and reported that the postoperative functional outcome demonstrated significant improvement compared to preoperative function (p<0.001) 35 . In addition, the limited approach (PSF without halo-gravity traction or three-column osteotomies) also distinguishes the current study from other more invasive approaches reported in the literature.
There were several limitations in our study. This study spanned over a 9-year duration. There might be variations in surgical technique that could influence the outcome. This was illustrated in Table 2, as the operation duration, blood loss, and transfusion rate were lower in the second period of the study. However, more screws were used but lower correction rate of the major curve was achieved in the second period. This could be probably due to the change in the surgical technique, that is, to avoid overcorrection of the major curve (especially the main thoracic curve in Lenke 1 and 2 curves) to achieve a harmonious correction for better shoulder and trunk balance. Although this cohort was the largest to report on the perioperative outcome of severe rigid scoliosis, the durability of a lesser correction and its effect towards the overall shoulder and trunk balance as well as the patients’ health-related quality of life (HRQOL) would need to be proven in future studies. Thirdly, the sagittal parameters were not analyzed in this study. However, the main purpose of the current study was to report on the perioperative outcome of our approach. Future studies could focus on the long-term radiological as well as the HRQOL scores for severe rigid scoliosis patients. All patients underwent single-staged PSF with the majority of patients being operated by the two senior surgeons in our center. Therefore, we did not have control groups to make fair comparisons between different surgical techniques (current technique versus three-column osteotomies) or between single surgeon versus dual surgeon strategy in this study.
Conclusion
Severe rigid idiopathic scoliosis treated with single-staged PSF utilizing a dual attending surgeon strategy demonstrated an average correction rate of 50.9%, an average operation duration of 215.5 min and a mean duration of postoperative hospital stay of 76.9 h. The overall rate of allogeneic transfusion was 24.4% and the perioperative complication rate was 9.8%.
Footnotes
Acknowledgement
We wish to acknowledge Miss Siti Mariam Mohamad, Miss Siti Mariam Abd Gani, Miss Josephine Rebecca Chandren, Mrs Chua Sock Koon, Mrs Tang Suet Mooi and Mrs. Winnie Loke Lai Sing for their contribution to this paperwork.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.