
Abstract
Purpose:
Surgical delay due to the wait for advanced cross-sectional imaging in occult fragility hip fracture management is not well studied. Our study aims to investigate computed tomography (CT) as an alternative to the gold standard magnetic resonance imaging (MRI) in occult hip fracture workup to decrease surgical delay.
Methods:
We conducted a retrospective review of all CTs and MRIs performed between 2015 and 2017 for patients with clinically suspected fragility hip fractures and negative plain radiographs to investigate surgical delay resulting from the wait for advanced imaging and representations due to missed fractures.
Results:
A total of 243 scans (42 CTs and 201 MRIs) were performed for occult hip fracture workup over the study timeframe, of which 49 patients (20%) had occult hip fractures [CT: 6 (14%), MRI: 43 (21%), p = 0.296)]. There were no readmissions for fracture in the 12 months following a negative scan. The CT group had shorter waiting times (CT: 29 ± 24 h, MRI: 44 ± 32 h, p = 0.004) without significantly reducing surgical delay (CT: 82 ± 36 h, MRI: 128 ± 58 h, p = 0.196). The MRI group had a higher number of patients with a cancer history (p = 0.036), reflective of the practice for workup of possible metastases as a secondary intention.
Conclusion:
Advanced cross-sectional imaging wait times in occult hip fracture workup contribute significantly to surgical delay. Modern CT techniques are not inferior to MRI in detecting occult fractures and may be a suitable alternative in the absence of a cancer history if MRI cannot be obtained in a timely fashion or is contraindicated. Clinicians should utilize the more readily available imaging modality to reduce surgical delay.
Keywords
Introduction
Fragility hip fracture is an increasing global health issue with earlier estimates of hip fractures to rise from 1.66 million in 1990 to 6.26 million by 2050 worldwide due to increasing life expectancies and the growing number of elderly individuals. 1 This is a recognized major public health problem in the West and a growing problem in Asia. 1 –3 Latest estimates in 2018 using data from China, Hong Kong, India, Japan, Korea, Malaysia, Singapore, Taiwan, and Thailand have confirmed that this trend in Asia with hip fractures projected to increase 2.28-folds from 1,124,060 in 2018 to 2,563,488 in 2050 in these countries despite the availability of better fracture prevention and treatment in recent years. 4 Assuming that the rest of Asia has similar hip fracture incidence rates, the total number of hip fracture occurrences in Asia alone will reach 3.66 million. 4
The emphasis on early surgical intervention in the management of hip fractures has been advocated in recent years in light of the significantly increased mortality rates and risk of pressure sores associated with surgical delay beyond 24–48 h. 5 Occult fractures constitute 2–10% of fragility hip fractures 6 –10 and are associated with considerable delays in their diagnosis as they cannot be visualized on plain radiographs, which require advanced cross-sectional imaging to diagnose and a high index of suspicion to pick up.
Magnetic resonance imaging (MRI) has traditionally been the gold standard imaging modality as the cross-sectional imaging of choice in the investigation of occult hip fractures 10 –18 (Figure 1). Unfortunately, these may not be readily accessible and are contraindicated in some patients. 19 Recent studies show that modern multislice computed tomography (CT) may be comparable to MRI in detecting occult fractures especially when read by experienced musculoskeletal radiologists. 19,20 As CTs are usually more accessible than MRIs and do not have absolute contraindications in noncontrast scans, these may be viable alternatives to MRIs in the workup of occult hip fractures to expedite time to the operating theater, thereby mitigating the mortality risks associated with surgical delay.

(a) Plain radiograph showing no evidence of fracture in the left hip and (b) T1-weighted MRI imaging showing a subcapital neck of femur fracture of the left hip that was not visualized on plain radiographs. MRI: magnetic resonance imaging.
At present, the literature is sparse on surgical delays resulting from the wait for advanced cross-sectional imaging in the investigation of occult fragility hip fractures. Our study aims to investigate delays to surgery due to MRI and CT waiting times in the workup of occult hip fractures, representation rates due to missed fractures, and the incidence of occult fragility hip fractures in a multiethnic Asian population.
Method
Study sample
We conducted a retrospective review of all CT and MRI scans performed between 2015 and 2017 at a tertiary hospital in patients with clinically suspected hip fractures and negative plain radiographs. This was on the background of 1010 confirmed fragility hip fractures admitted during the study time frame. Patients with high-energy trauma, polytrauma, and/or age less than 55 were excluded. The choice of imaging modality was made based on patient compliance, scan availability, and surgeon preference.
The MRI scanners utilized during the study period were Siemens (Siemens Healthcare, Erlangen, Germany) MAGNETOM Skyra and Siemens MAGNETOM Avanto, while the CT scanners utilized were Philips (Philips Healthcare, Eindhoven, The Netherlands) Brilliance iCT 256, Siemens SOMATOM Force, and Siemens SOMATOM Sensation.
Assessments
The outcomes assessed were (i) surgical delay resulting from the wait for advanced imaging in the workup of the occult hip fractures, (ii) representations due to missed fractures, (iii) time from scan request to scan acquisition and time to surgery from admission, and (iv) length of hospital stay between the CT and MRI groups. Patient demographics, comorbidities, and fracture types were also assessed and compared.
Ethical approval
Ethical approval for the study was granted by the hospital’s ethics committee (Ref: 2016/2995).
Statistical analysis
The data were compiled and analyzed using SPSS version 21 (SPSS Inc., Chicago, Illinois, USA). The χ 2 and Fisher exact tests were used in the statistical analysis of categorical variables. Continuous variables were analyzed for normality using the Shapiro–Wilk test. Normally distributed variables were analyzed using the t-test for parametric analyses, and the Mann–Whitney U-test was used for nonparametric analyses otherwise. Means are presented along with standard deviations. Counts are displayed with percentages. All p values <0.05 were considered significant.
Results
A total of 1012 advanced cross-sectional imaging scans involving 545 CTs and 467 MRIs were performed for the pelvis and hip between 2015 and 2017 at our institution. Of the 1012 scans, 586 were performed in patients with hip or groin pain. One hundred twenty-nine patients did not meet inclusion criteria. Of the remaining 457 scans, 214 had positive findings on plain radiographs for hip fractures. The advanced cross-sectional imaging scans were performed in this group for further characterization of the fracture patterns to determine the underlying etiology of the fractures. The remaining 243 scans were performed in patients with clinically suspected hip fractures and negative plain radiographs to investigate for occult hip fractures. Of the 243 advanced imaging studies, 42 CT (17%) and 201 MRI (83%) scans were performed (Figure 2).

Derivation of study population from all cross-sectional imaging scans performed for the pelvis and hip between 2015 and 2017.
The demographics and comorbidity profiles of the CT and MRI groups are provided in Table 1. Both groups showed similar mean ages and similar male–female ratios. Both groups also showed a predominant Chinese patient population, reflective of our population distribution. 21 The comorbidity profiles were also similar between the CT and MRI groups except for a higher number of patients with a history of cancer in the MRI group (p = 0.036). This was for the workup of possible metastases as a secondary intention on top of the search for an occult fracture due to MRI’s superiority in the workup for malignancy.
Clinical details of patients who underwent CT or MRI with clinical suspicion of hip fractures with negative plain radiographs.

CT: computed tomography; MRI: magnetic resonance imaging; SD: standard deviation.
p values <0.05 were considered significant (Bolded text).
A total of 49 patients (20%) were found to have occult hip fractures. The proportion of patients identified with occult hip fractures in each group was similar (CT group: 6 (14%), MRI group: 43 (21%), p = 0.296; Table 1). There was no history of trauma in 5 of the 49 patients (10%). There were no readmissions for fracture in the 12 months following a negative scan.
The average waiting time for CT was 29 ± 24 h versus 44 ± 32 h for MRI (p = 0.004; Table 2). Time to surgery from admission (CT group: 82 ± 36 h, MRI group: 128 ± 58 h, p = 0.196) and mean length of hospital stay (CT group: 10 ± 6.0 days, MRI group: 13 ± 8.9 days, p = 0.522) were also shorter in the CT group although these did not reach statistical significance (Table 2).
Comparison of the types of fractures, surgical delay, comorbidities, and health services utilization in patients with occult fractures between the CT and MRI groups.
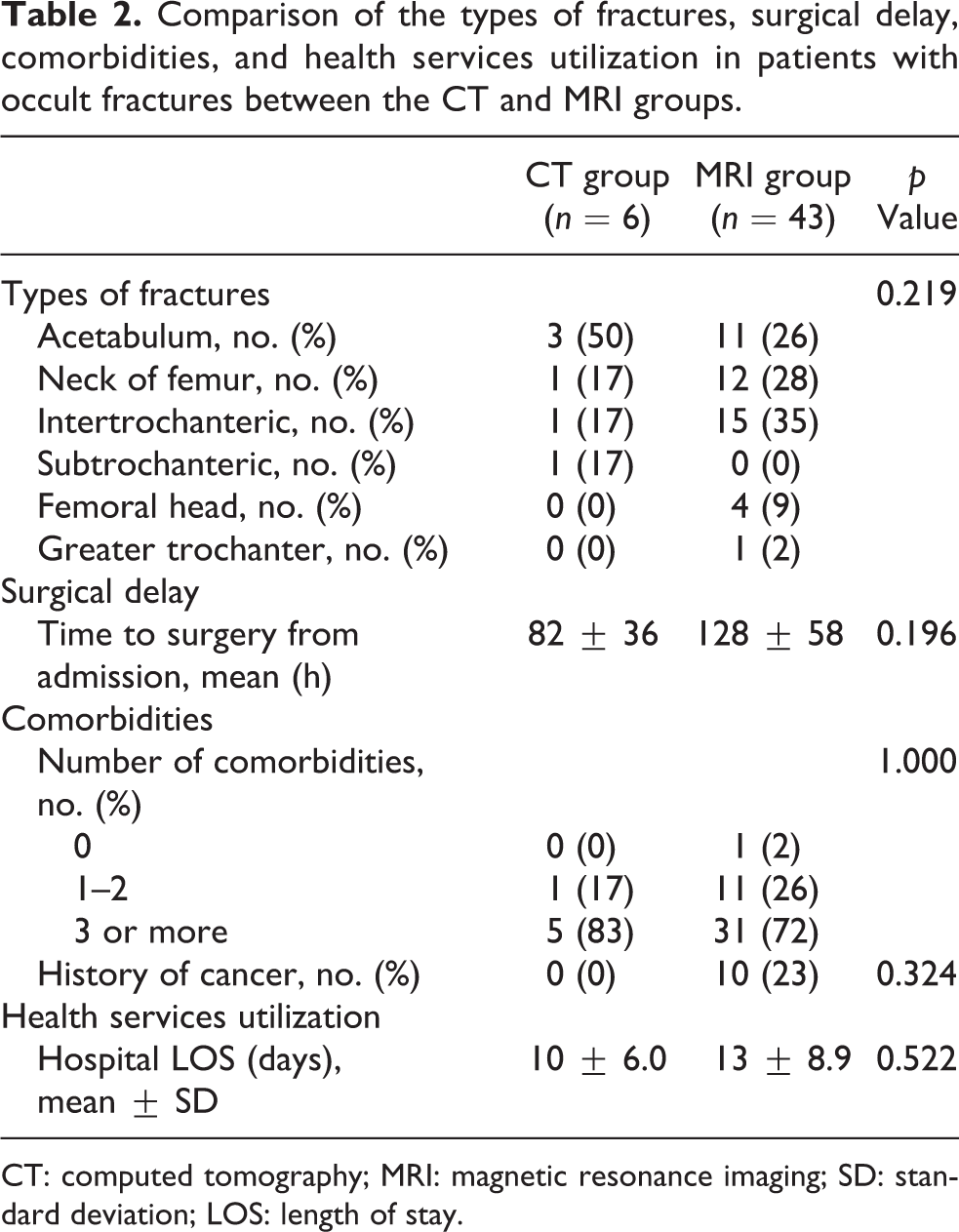
CT: computed tomography; MRI: magnetic resonance imaging; SD: standard deviation; LOS: length of stay.
The anatomical distribution of occult fractures in the hip is similar in both CT and MRI groups (p = 0.219). Occult fractures occurred most frequently in the acetabulum, neck of femur, and intertrochanteric region, common to both the CT and MRI groups (Table 2).
Of the 49 occult hip fractures, 23 were managed operatively (CT group: 3, MRI group: 20). All 23 of the occult hip fractures that were managed operatively were in the proximal femur. Twenty-two of the 23 patients were managed with fixation and the remaining 1 patient (from the MRI group) was managed with a cemented bipolar hemiarthroplasty. All fractures in the neck of femur and in the subtrochanteric region were managed operatively. The decision for replacement surgery was made in view of her advanced age at 100 years old. The remaining 26 patients underwent nonoperative treatment with varying protocols for weight bearing depending on the type of fracture. There were no complete fractures that were managed nonoperatively.
There were seven incomplete intertrochanteric fractures in the MRI group. The fracture line extended from the greater trochanter involving up to 50% of the intertrochanteric region in the coronal plane in six patients and 70% of the intertrochanteric region in one patient. The femoral calcar was intact in all seven cases. The patient that had an incomplete intertrochanteric fracture that involved 70% of the intertrochanteric region declined surgery. All patients with incomplete intertrochanteric fractures were managed with 4–6 weeks of nonweight-bearing initially on the affected limb, followed by a gradual increase in weight-bearing status, guided by their clinical progress (Table 3).
Management of patients with occult hip fractures.

CT: computed tomography; MRI: magnetic resonance imaging.
All acetabulum fractures (CT group: 3, MRI group: 11) were managed nonoperatively in our study. All 14 acetabular fractures involved the anterior column to varying degrees, 6 of which also involved the acetabular roof, and 2 others involved the medial wall. All patients with acetabular fractures involving the roof and medial wall were managed with 4–6 weeks of nonweight bearing initially on the affected limb, followed by a gradual increase in weight-bearing status (Table 3). The remaining six patients were allowed full-weight-bearing as tolerated (Table 3).
There were four femoral head fractures in the MRI group and none in the CT group. All four femoral head fractures in the MRI group were subchondral insufficiency fractures. These were managed with partial weight-bearing for 4 weeks followed by a gradual increase in weight-bearing status (Table 3). The case of greater trochanter fracture in the MRI group was managed with protected weight-bearing and with limitations to hip abduction for 6 weeks (Table 3). There were no cases of greater trochanter fracture in the CT group.
All sacral insufficiency fractures and fractures of the pubic rami identified were managed nonoperatively, hence not reported.
Discussion
A total of 49 occult fractures were identified from 243 advanced cross-sectional imaging studies performed over the 3-year study time frame. This is on the background of 1010 confirmed fragility hip fractures during the same time frame, putting our occult hip fracture rate at 4.9% in our multiethnic Asian population. A total of 194 (36 CTs and 158 MRIs) scans were negative for occult fractures. Importantly, there were no readmissions for fracture in the 12 months following a negative scan. With increased mortality rates and risk of pressure sores associated with surgical delay beyond 24–48 h, average wait times of 29 h for CT and 44 h for MRI in occult hip fractures workup contribute significantly to surgical delay.
The emphasis on early surgical intervention in the management of hip fractures has been advocated in recent years in light of the significantly increased mortality rates and risk of pressure sores associated with surgical delay beyond 24–48 h. 5
Rehman et al. reported 71 cases of occult hip fractures in 177 advanced cross-sectional imaging scans performed with either CT or MRI over a 4-year time frame. 20 Of the 177 scans performed, 77 were CTs, of which 35 were negative for hip or acetabulum fractures. 20 They too had no missed fractures that represented within 12 months postdischarge and went on to conclude that CT should be considered the first-line investigation for occult hip fractures. 20
The yield for the detection of occult fractures in the proximal femur and acetabulum was similar in both CTs and MRIs in our study irrespective of the choice of imaging modality, reflecting consistency in clinical practice and acumen of the clinicians in suspecting occult hip fractures. Despite shorter waiting times for the scan in our CT group, 83% of our advanced cross-sectional imaging scans performed were still MRIs, of which 158 of the 201 MRIs were negative for occult hip fractures. With the total number of MRIs performed for the pelvis and hip during the study time frame at 467, inclusive of MRIs performed for the investigation of other pathologies, 201 MRIs performed for the investigation of occult hip fractures contribute significantly to the imaging load and longer waiting times.
MRI is traditionally thought to be superior to other imaging modalities in diagnosing occult proximal femoral fractures and recommendations have been made for MRIs to be performed within 24 h to avoid subsequent displacement and complications. 22,23 This superiority of MRI over CTs was demonstrated in the detection of femoral head and acetabulum insufficiency fractures in Cabarrus et al.’s study of insufficiency fractures of the pelvis and proximal femur, where MRI showed a 99% detection rate (128 of 129 fractures) compared to CT’s 69% detection rate (89 of 129 fractures). 24 In Chatha et al.’s systematic review of 350 patients with occult proximal femoral fractures, where 295 (84%) underwent subsequent surgery, the authors highlighted that incomplete intertrochanteric fractures can only be diagnosed with certainty using MRI. 22 With the advent of multislice CT scanners capable of delivering high-resolution, fine-cut imaging in recent years, the sensitivity and specificity for detection of occult hip fractures have improved. In Sadozai et al.’s study of 78 CT scans using the Siemens Somatom Sensation 64 CT scanner, the sensitivity and specificity for detection of occult hip fractures were reported to be 86% and 98%, respectively. 25
The majority of the scans performed in our study were MRI scans, reflective of the practice at our institution for the investigation of occult hip fractures adhering to MRI scans as the gold standard imaging modality of choice. However, with a mean waiting time of 44 h for the MRIs, this has significantly exceeded recommendations from the National Institute for Health and Care Excellence (NICE) guidelines to consider CT if MRI cannot be performed under 24h. 23
CT is the next line of recommendation as an alternative to MRI if MRI is not available within 24 h or is contraindicated in the NICE guidelines. 23 Gill et al. reported similar pickup rates for occult hip fractures between the CT and MRI groups with a pickup rate of 38% in the CT group (23 of 61 CTs) and 36% in the MRI group (11 of 31 MRIs) 19 . Rehman et al. had a higher rate of occult hip fractures picked up on CT scans at 48% (37 of 77 CTs) compared to MRI at 34% (34 of 100 MRIs). 20 Apart from being more available after hours compared to MRI, the cost for CT is also lower. 26
Our nonoperative management of incomplete intertrochanteric fractures is consistent with earlier literature. Schultz et al. reported no difference in clinical outcomes on follow-up in their study of patients with incomplete intertrochanteric fractures that were managed surgically (n = 18) compared to those that were managed nonoperatively (n = 13). 27 Alam et al. reported no progression to a complete fracture in any of their patients with incomplete intertrochanteric fractures managed nonoperatively after a mean of 3.2 years despite patients mobilizing on discharge after a mean hospital stay of 16 days. 28
With the increasing prevalence of fragility hip fractures globally and a reported 2–10% of fragility hip fractures being occult, 6 –10 the actual numbers of occult hip fractures are significant. The strengths of our study are as follows: (i) we are one of few studies evaluating surgical delays relating to waiting times for advanced cross-sectional imaging and rates of missed diagnoses comparing MRI and CT in the investigation of occult fragility hip fractures, (ii) utilization of an electronic database for record-keeping of patient’s data and imaging eliminates loss of data from poor record-keeping, and (iii) given the recent emphasis on early surgical intervention in the management of hip fractures to reduce mortality rates and risk of pressure sores, our study adds important data on a hitherto poorly studied aspect of surgical delays in the management of hip fractures that can potentially be improved on.
However, there were also some limitations. Our study limitations include (i) the retrospective design of the study inevitably leads to some selection bias, (ii) the relatively low number of patients with occult fractures limit the power of the study, and (iii) the lack of objective functional outcome assessments limit our ability to correlate whether the increased need for rehabilitation facilities in the MRI group resulted in poorer outcomes subsequently.
Conclusion
Surgical delay resulting from the wait for advanced cross-sectional imaging in the investigation of occult fragility hip fractures is significant. Modern CT techniques are not inferior to MRI and may be considered as a suitable alternative in the detection of occult fractures in the absence of a cancer history if MRI cannot be obtained in a timely manner or in the event of contraindications to MRI. Clinicians should utilize whichever cross-sectional imaging modality more readily available at their institution to expedite time to the operating theater.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.