
Abstract
Introduction:
The National Institute of Health and Clinical Excellence guidelines in the United Kingdom recommend magnetic resonance imaging (MRI) as the first-line investigation for radiographically occult hip fractures, if available within 24 hours. In our department, however, multislice computerized tomography (MSCT) is instead used as a first-line investigation due to significant delays associated with obtaining MRI. Our aim was to determine the validity and practicality of MSCT for diagnosis of occult hip fractures and its impact on timing of surgery.
Materials and Methods:
We retrospectively analyzed medical records and imaging for consecutive patients who underwent MSCT to investigate occult hip fractures between January 2014 and October 2016. We reviewed subsequent imaging and reattendances for patients with negative MSCT to exclude initially missed fractures.
Results:
Two hundred six patients underwent MSCT to investigate occult hip fracture during the study period. Hip fractures were identified in 59 patients, comprising 35 (59.3%) subcapital, 12 (20.0%) intertrochanteric, 8 (13.6%) transcervical, and 4 (6.8%) basicervical fractures. One missed hip fracture was identified: a patient with a negative MSCT was further investigated with MRI that demonstrated acute subcapital hip fracture. Multislice computerized tomography was obtained within 24 hours of initial radiograph in 145 (70.4%) patients. A total of 44.5% of occult hip fractures had surgery within the nationally recommended 36 hours of admission (hospital average for all hip fractures was 76.4% over the same period).
Discussion and Conclusions:
Multislice computerized tomography is a pragmatic approach to investigate the majority of occult hip fractures in a timely manner and minimize associated delay to surgery. However it cannot completely exclude the diagnosis, especially in abnormal anatomy. The lack of a true gold standard comparison (ie, MRI) means a true sensitivity and specificity cannot be calculated, although can be cautiously estimated by lack of subsequent reattendance or investigation. Further prospective randomized CT versus MRI trials are required.
Keywords
Introduction
Between 3% and 10% of hip fractures are occult on plain radiography, 1 –4 representing a significant proportion of patients with traumatic hip pain that warrant further investigation with advanced imaging. The National Institute of Health and Clinical Excellence in the United Kingdom recommends magnetic resonance imaging (MRI) as first line, if available within 24 hours. 5 A number of recent studies report trauma units instead offering computerized tomography (CT) as the first-line investigation, citing delays associated with obtaining MRI and improvements in modern CT imaging 6,7
Modern multislice CT (MSCT) can produce multiplanar and 3D reconstructions which allow for accurate assessment of fracture lines, displacement, and comminution. It has been suggested that the evidence base favoring MRI over CT is outdated in view of advances in modern CT technology. 8 National Institute of Health and Clinical Excellence have acknowledged that evidence of similar accuracy between the 2 modalities would have considerable implications because of the wider availability and lower cost of CT. 9
In our unit, we use MSCT as our primary method of investigating suspected occult hip fracture (OHF) due to excessive delays in obtaining MRI. In this study, we examined a series of patients who had undergone MSCT to investigate OHF in order to determine the practicality and validity of its use. Furthermore, we studied the time taken to obtain MSCT and associated delay to surgery.
Materials and Methods
Consecutive MSCT studies of the hip or pelvis performed between January 2014 and October 2016 were compiled and analyzed retrospectively. The clinical request details were reviewed and all patients undergoing MSCT to investigate suspected OHF were included. Our definition of “occult” was either negative or equivocal plain radiographs as determined by the clinician requesting the MSCT. Patients undergoing MSCT of the hip or pelvis for other indications or for surgical planning were excluded.
Data were recorded from all relevant imaging and medical records during the hospital admission in question. Further imaging or hospital admissions after the initial MSCT were reviewed to exclude missed hip fracture. This study does not have a true gold standard investigation (ie, MRI) comparison for each case, meaning the true diagnostic accuracy cannot be calculated. However, we have used the absence of readmission or further investigation for hip pain following a negative MSCT scan as a proxy for a true negative.
Admission time was taken to be from the initial emergency department plain radiograph, which occurs as part of the triage process of traumatic hip pain. Noncontrast CT examination was performed using a Toshiba Aquilion 64 scanner (Toshiba Medical Systems, Otawara, Japan) in 0.5-mm axial slices with 3 mm coronal and sagittal reconstructions. All imaging was reported by consultant radiologists.
Hospital hip fracture data for our unit from the UK National Hip Fracture Database annual reports from 2014 to 2016 were also reviewed. 10 Statistical analysis was performed using MedCalc version 17.0.4 (MedCalc Software, Mariakerke, Belgium) and The Statistical Package for the Social Science SPSS version 20 (SPSS Inc, Chicago, Illinois).
Results
A total of 557 MSCT studies of the hip or pelvis were originally identified during the study period. After exclusions, 206 patients who had undergone MSCT to investigate suspected OHF formed the basis of the study cohort. The median age was 82 years and female:male ratio was 144:62 (70%:30%).
Hip fractures were demonstrated on MSCT in 59 (29%) patients, comprising 35 (59.3%) subcapital, 12 (20.0%) intertrochanteric, 8 (13.6%) transcervical, and 4 (6.8%) basicervical fractures. Ninety (44%) of the MSCT studies were reported as no fracture, 20 (10%) pubic rami fractures, 19 (9%) greater trochanter femoral fractures, 8 (4%) acetabular fractures, and 10 other pelvic fractures (Table 1).
Distribution of Hip Fracture Pattern and Other Injuries.

Abbreviation: fx, fracture.
One patient with a negative MSCT study subsequently underwent MRI due to persistent pain that demonstrated an acute subcapital hip fracture.
Median time from admission to MSCT was 15 hours (range: 1-187 hours) and 70% were performed within 24 hours of admission. A total of 91% of MSCT scans were performed within 24 hours of being requested.
Median time to theater from admission was 36 hours (range: 15-117 hours), and 44% were performed within the nationally recommended 36 hours of admission. Median time from MSCT to theater was 23 hours (range: 2-74 hours). The National Hip Fracture Database reported 76.0% of all hip fracture patients at our unit went to theater within 36 hours during the study period (2016: 71.7%; 2015: 81.1%; 2014: 75.3%). 10
Discussion
We have demonstrated that MSCT is a useful and pragmatic investigation for OHF in the vast majority of patients in a unit where MRI is not readily available. Subcapital fractures were the most common fracture pattern in our occult fracture cohort and the majority (70%) of CT scans were performed within 24 hours of admission.
As discussed, without a gold standard true negative comparison (MRI), the diagnostic accuracy cannot be truly calculated. If, however, we use our proxy measure, we can estimate a sensitivity of 98.33% (95% confidence interval [CI]: 91.06%-99.96%) and a specificity of 100% (95% CI: 97.51%-100%) for OHF (Table 2). Clearly, these results must be interpreted with caution.
A 2 × 2 Contingency Table for MSCT and Hip Fracture.
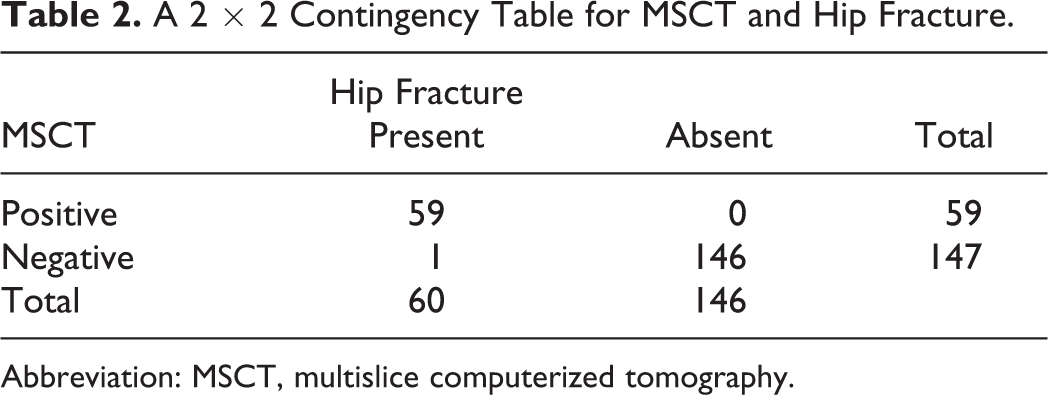
Abbreviation: MSCT, multislice computerized tomography.
With 206 consecutive patients meeting the inclusion criteria, this is the largest study to date, comparably powered to recent studies by Thomas et al, 6 Dunker et al, 11 and Hakkarinen et al 1 with 199, 193, and 155 patients, respectively. All suspected OHF undergo MSCT in our unit, which reduces the risk of selection bias compared to reports from institutions where both MRI and CT are used. 1,8,12,13
By reviewing all MSCT studies of the pelvis and hip performed at our institution, we were able to ensure accurate inclusion of suspected OHF into our cohort, avoiding attendant error associated with gathering patients based on clinical coding. All MSCT studies were performed with the same scanner and reported by consultant radiologists.
Limitations
It is possible that patients discharged following a negative MSCT scan may have subsequently attended a different unit with a missed fracture, which we would not have identified in our review. Data were gathered retrospectively and the inclusion criteria were based upon the documentation of the clinician requesting the MSCT. We did not have a “gold standard” (ie, MRI) to compare MSCT with. Additionally, comparison of delays to surgery compared to National Hip Fracture Database (UK) reports is not ideal due to inclusion of OHFs in the overall data.
Literature
Reports of the diagnostic accuracy of CT for OHF are conflicting in the existing literature, and there are marked variations in study size and methodology. Thomas et al report 100% sensitivity of MSCT for 199 suspected OHF in a retrospective study over 30 months, in a unit where MSCT is used as the primary investigation for OHFs. 6 Dunker et al found MSCT missed 2 fractures in 193 patients and falsely identified 2 fractures (specificity 98.2%; sensitivity 97.6%) but only included MSCT scans performed within 24 hours of initial radiograph. 11 Rehman et al compared MRI with CT in a retrospective study of 177 patients (MRI:CT, 100:77), although the patients were not randomly allocated to either group. 8 Both MRI and CT sensitivity were reported as 100%.
In contrast, Sadozai et al concluded from their retrospective study of 78 patients who MSCT had a sensitivity of 86% for OHF and therefore should not be recommended over MRI. 14 An 8-year retrospective study of 44 patients who had undergone MRI following CT for suspected OHF found CT missed 9 hip fractures. 15
There has been a large prospectively designed trial to compare accuracy of MRI and CT for OHF. 16 Haubro et al investigated 67 suspected OHF with both modalities and found MSCT missed 2 of 15 fractures found on MRI (sensitivity 87%). Their study was insufficiently powered to determine a statistical difference between the sensitivities of the 2 modalities.
False Negative Result
The patient in our cohort in whom MSCT did not demonstrate the hip fracture had previously sustained an ipsilateral intertrochanteric fracture which had since healed, complicating interpretation of the images (Figure 1). Magnetic resonance imaging of the hip subsequently demonstrated bone marrow edema indicating recent injury, which is not apparent on MSCT. The patient underwent cannulated screw fixation and recovered well.

Axial CT image (left) and T1-weighted MRI (right) of the missed subcapital hip fracture (previous healed intertrochanteric fracture demonstrated). CT indicates computerized tomography; MRI, magnetic resonance imaging.
Conclusions
We believe modern MSCT is a pragmatic investigation for suspected OHF in the vast majority of patients in situations where MRI is not promptly available, although the available literature remains contradictory. We have demonstrated that MSCT was unable to identify an acute fracture on the background of a previously healed ipsilateral hip fracture, suggesting it is unsuitable to rule out OHF in this uncommon situation. This may suggest MSCT is inappropriate in other causes of abnormal preexisting bony anatomy, such as previous hip surgery or pathological fractures. It therefore follows that persistent hip pain following a negative MSCT in this group of patients warrants further investigation with MRI. While the advantages of wider availability, speed, and decreased cost are clear with MSCT, further prospective randomized study of MSCT against MRI will be necessary to justify a change in best practice guidelines.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.