
Abstract
Purpose:
The mechanisms underlying thigh pain in patients with well-fixed cementless femoral components after total hip arthroplasty (THA) remains unclear. We hypothesized that the thigh pain is correlated with the initial contact state of the stem and aimed to investigate the relation between thigh pain and the initial contact state.
Materials and methods:
A total of 209 hips of 184 patients were analysed in this retrospective case–control study. The patients were divided into a thigh pain group (n = 13 hips) and a control group (without thigh pain, n = 196). Post-operative stem contact images were three-dimensionally visualized by a density mapping function using computed tomography data, which quantified the stem contact area according to Gruen zones. Thigh pain was defined as anterior or anterolateral pain upon loading at 3-month post-operatively.
Results:
Thirteen hips (6.2%) had thigh pain; however, all the hips demonstrated stable bony ingrowth radiographically. The thigh pain group had a significantly lower contact area in zone 2 (p = 0.014). The multivariate logistic regression analysis showed that the contact area of zone 2 was negatively correlated with thigh pain [odds ratio (OR): 0.858, p = 0.018], and the canal flare index was negatively correlated with the development of thigh pain (OR: 0.336, p = 0.026).
Conclusions:
We identified an association between the initial contact state and post-operative thigh pain. Our data demonstrated that proper lateral contact prevents the occurrence of thigh pain in THA using a tapered wedge stem.
Introduction
Thigh pain is a recognized problem after cementless primary total hip arthroplasty (THA) 1 –3 and is generally considered as a self-limiting phenomenon that does not necessitate medication. 1,4 Consequently, thigh pain following THA is not perceived as a serious problem by surgeons. However, persistent thigh pain following THA can be a source of significant patient dissatisfaction. 2,5 Although some stem designs such as the tapered wedge stem are shown to reduce the prevalence of thigh pain, the pain occurs in up to 7% of cases. 6 –9
While thigh pain is associated with multiple factors, 2,10 –13 the mechanisms underlying thigh pain remain unclear. Although some reports have hypothesized that excessive stress concentration on the stem tip results in thigh pain, 11,12 data supporting this hypothesis are lacking. In this study, we hypothesized that there would be a correlation between the occurrence of thigh pain and the initial stem contact state, and a greater stem contact area in zone 2 would prevent excessive stress concentrations to the stem tip, preventing thigh pain. Our previous study showed application of computed tomography (CT)-based templating software in quantifying the area of stem contact. 14 The current study aimed to assess the correlation between the development of thigh pain and the initial contact state, using a three-dimensional CT-based density mapping system and analyse the risk factors associated with thigh pain.
Materials and methods
Ethical approval
The study protocol was approved by the hospital investigational review board and the Science Ethics Committee.
Study design and patients
This retrospective case-controlled study assessed 547 consecutive primary THAs in 461 patients between February 2009 and February 2016. The medical records of all patients were reviewed, and basic demographic data were collected. Follow-up and data collection continued until February 2017. Exclusion criteria for this study were previous hip surgery (pelvic or femoral osteotomy or arthrodesis), trauma, infection and poliomyelitis; patients who did not have tapered wedge stems were also excluded (316 THAs, 256 patients). Patients who were not followed up for a minimum of 1 year (12 THAs, 11 patients) and those without any post-operative CT data were also excluded (10 THAs, 10 patients). Remaining 209 hips (in 184 patients), which had undergone THA using two tapered wedge stems (Accolade TMZF and Accolade II; Stryker Orthopaedics, Mahwah, New Jersy, USA), were included in this retrospective study (Figure 1). The Accolade TMZF stem is made from a titanium alloy and has a proximal circumferential plasma spray that features a 50-μm-thick hydroxyapatite (HA) coating (Purefix HA; Stryker Orthopaedics) and a distal matte finish. The Accolade II stem is shorter than the Accolade TMZF which was the first-generation stem and has a size-specific medial curvature design based on a large CT database. 15

Patient selection flow chart.
Patient demographic data are presented in Table 1. Routine follow-up visits were scheduled at 3-, 6- and 12-month post-operatively and every 6 months or 1 year thereafter. Patients were asked about their pain at each follow-up evaluation. A diagnosis of thigh pain was made according to the definition of Barrack et al. 1 Pain that developed 3 months after surgery was considered anterior or anterolateral on loading. Patients with post-operative infection, dislocation, fracture or trauma, iliopsoas impingement (IPI), trochanteric bursitis, radiculopathy, stem loosening, rheumatoid arthritis and osteoarthritis of the knee joint were excluded from a diagnosis of thigh pain (Online Supplemental Table S1). Patients were diagnosed as having IPI if they had anterior groin pain with resisted hip flexion, straight leg raising or passive extension of the hip. Pain that improved after psoas tendon sheath injection with xylocaine and steroids was considered characteristic of IPI. Trochanteric bursitis was diagnosed if the tenderness of the greater trochanter (the attachment of the vastus lateralis) was present and local xylocaine injection to this site was effective. We reviewed the lower lumbar region on preoperative X-rays. When arthrosis of the spine was observed with neurologic findings (positive tests for Valleix tenderness, numbness, radial pain or straight leg raising), spinal stenosis or lumbosacral arthritis was considered to be the pain aetiology. Patients were divided into two groups: patients with thigh pain [thigh pain group, n = 13 hips (96.2%)] and those without thigh pain [control group, n = 196 hips (93.8%)]. Demographic data for each group are presented in Table 2. In all patients, symptoms improved to the level where they could perform normal daily activities. Overall, pain was absent during the final follow-up in nine hips (69.2%) and slight pain remained in four hips (30.8%). The details are presented in Online Supplemental Table S2.
Patient demographic characteristics.

BMI: body mass index; PL: posterolateral; MWJ: modified Watson Jones; ALS: anterolateral spine; CI: cortical index; CFI: canal flare index.
Demographic characteristics of the thigh pain group and the control group.
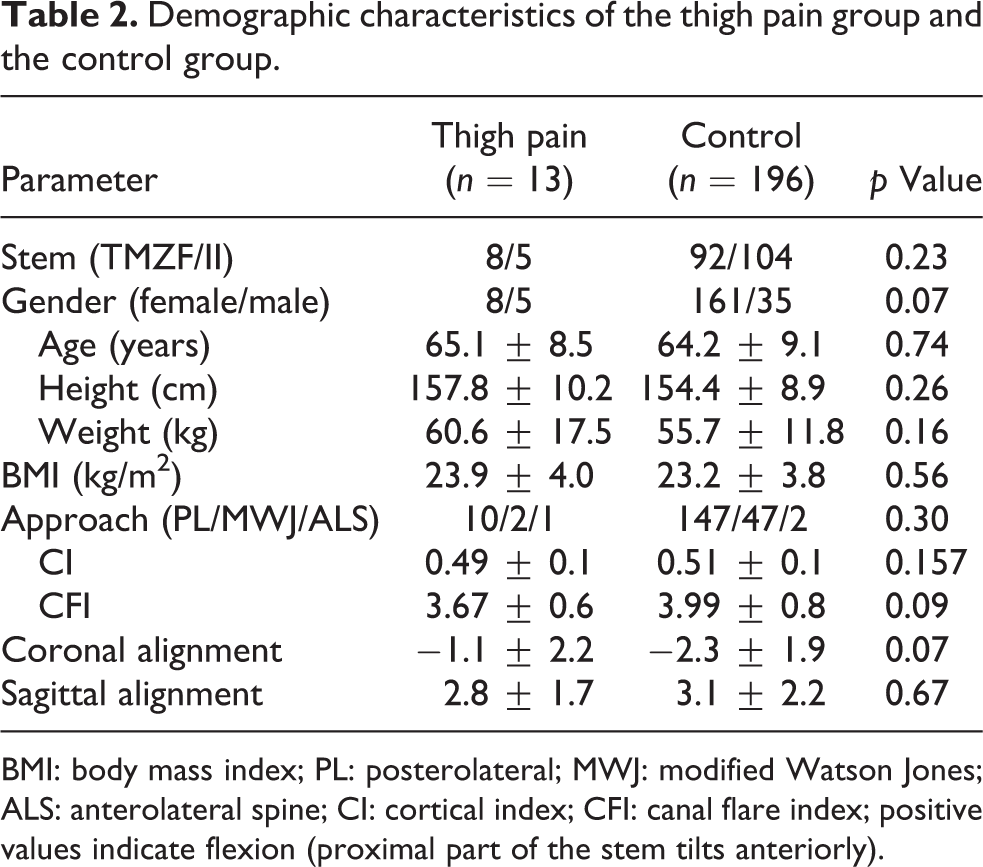
BMI: body mass index; PL: posterolateral; MWJ: modified Watson Jones; ALS: anterolateral spine; CI: cortical index; CFI: canal flare index; positive values indicate flexion (proximal part of the stem tilts anteriorly).
Surgical information and data collection
All surgeries were performed by a senior surgeon through one of three surgical approaches (posterolateral, modified Watson Jones or the anterior lateral supine approach) using a CT-based navigation system (CT-based hip, version 1.0 and 1.1; Stryker Navigation, Freiburg, Germany). Anteroposterior hip X-ray images were taken immediately following surgery and post-operatively at 2 weeks, 3 months, 6 months and every 1 year thereafter. CT scans were performed for preoperative planning and post-operative assessment 2 weeks after the operation. Scans were carried out with a helical CT scanner (Lightspeed VCT; GE Medical Systems, Milwaukee, Wisconsin, USA) to quantify the contact state of the implant and femur and to detect post-operative occult fracture – a post-THA complication. 16,17 Scans were carried out using a slice thickness of 1 mm and a pitch of 2.5 mm. All preoperative planning and post-operative evaluations were completed using a CT-based templating software ZedHip (Lexi Co, Tokyo, Japan). Stem alignment was measured in the retrocondylar plane based on the coordinate system of the femur. The width of the proximal femoral canal on the operated side was measured from the preoperative anteroposterior radiographs of the hip. For each patient, we calculated Noble’s canal flare index (CFI) 18 (Figure 2). Cortical index was measured at 10 cm below the mid-lesser trochanter 19 (Figure 2).
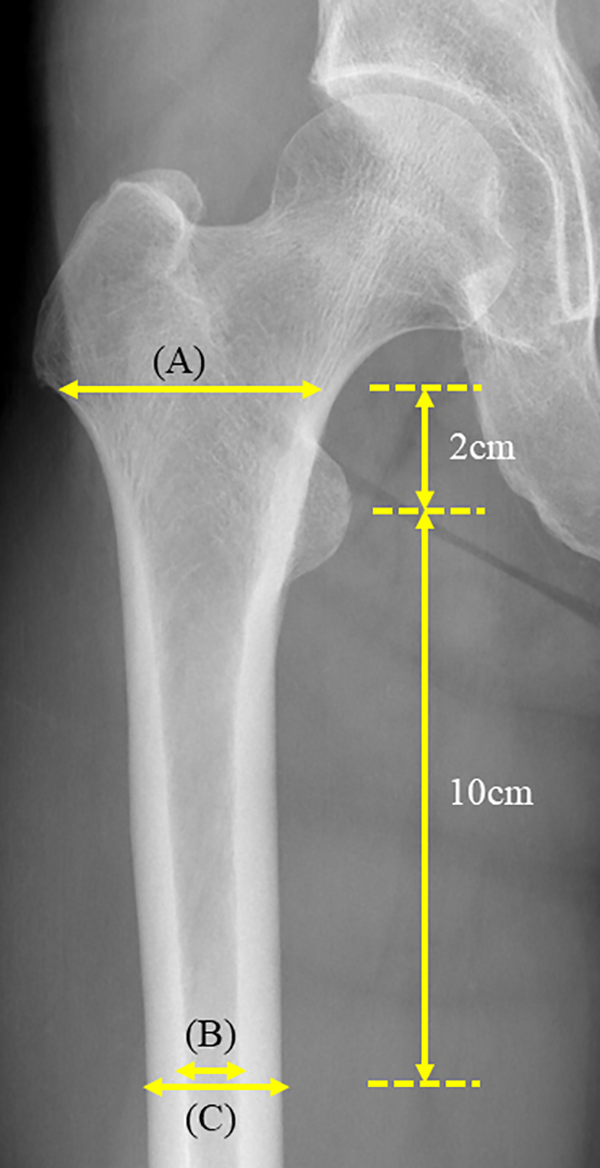
The CFI, originally described by Noble et al., 18 is defined as the ratio of the intracortical width of the femur at a point 20 mm proximal to the lesser trochanter and at the canal isthmus, which is commonly measured at a point 100 mm distal to the lesser trochanter. In this illustration, CFI = A/B. The cortical index is measured at 10 cm from the mid-lesser trochanter; C−B/C was shown in this illustration. 19 CFI: canal-flare index.
Methods of assessment
Density mapping
Using post-operative CT data, computer-aided design models of femoral stems were superimposed with the post-operative multiplanar reconstruction CT images using ZedHip. Metal halation created by implant insertion leads to difficulty in accurate measurement of the contact state using post-operative CT data. Therefore, we reproduced the post-operative state by enabling the preoperative CT data reflect the insertion angle of the post-operative implant, which allowed the measurement of the contact state of implant and femur according to the Gruen zones by density mapping. Density mapping delineates the contact state by colour based on the Hounsfield unit (HU) value, which was calculated from the CT data (Figure 3). 18 Using this technique, the contact region is shown in three colours: yellow denotes contact with the cortical bone; red denotes contact with the dense cancellous bone, and green denotes contact with the sparse cancellous bone. Density mapping function displays the results in percentages with respect to the total stem area and Gruen zone. We defined the effective contact region as the area where an implant was in contact with the cortical bone (yellow). Density threshold of the corticocancellous interface was established at 543 HU, as described in a previous report. 14 To assess intra-observer reliability, we analysed the density mapping in the first 20 patients. Inter-observer reliability was 0.870 (95% confidence interval (CI): 0.817–0.907, p < 0.001) for all zones, indicating satisfactory reliability.

Density mapping. The contact region is categorized into three zones: contact with cortical bone, dense cancellous bone and the sparse cancellous bone. Density mapping displays the results in percentages with respect to the total stem area and Gruen zone.
Radiographic evaluation
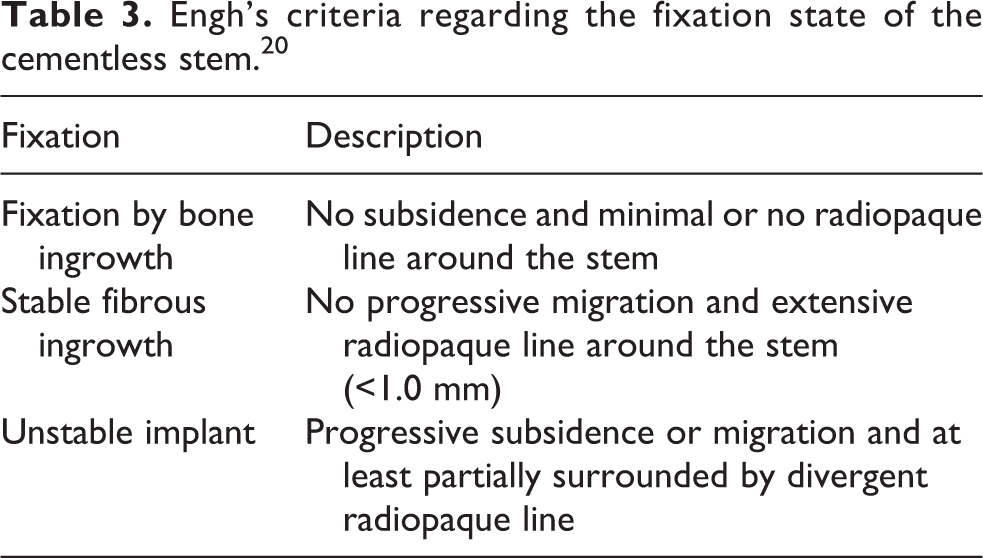
Femoral component fixation was evaluated according to the criteria of Dorr et al. 19 at the final follow-up using anteroposterior radiographs (Table 3). Subsidence of the femoral component was determined based on the relationship between the top of the great trochanter and the shoulder of the stem and was defined as a minimum reduction of 4 mm between the initial post-operative radiograph and final follow-up. Cortical hypertrophy was evaluated at the final follow-up using anteroposterior radiographs. Minimum follow-up period was 1 year (Accolade TMZF: mean 4.8 years, range 2–8 years; Accolade II: mean 2.6 years, range 1–4.4 years).
Engh’s criteria regarding the fixation state of the cementless stem. 20
Statistical analysis
Statistical analyses were performed using a statistical software package (SPSS software for Windows, version 23.0; SPSS, Inc., Chicago, Illinois, USA). Group comparisons for quantitative data were performed using unpaired t-tests, while categorical data were compared using the χ 2 test. Quantitative data are presented as mean ± standard deviation, and categorical data are presented in absolute and relative frequencies. Binomial logistic regression was applied for comparing between the thigh pain group and the control group. We analysed data using univariate and multivariate models and calculated adjusted odds ratios (ORs) and 95% CIs. Variables with p < 0.2 in the univariate analysis were considered for the multivariate model. We utilized the variable increase method for variable selection. Fidelity was evaluated using Hosmer and Lemeshow’s test with p < 0.05. Finally, the two-tailed post hoc power analysis showed that our sample size had a statistical power of 79.3% and an error of 5%.
Results
A comparison of the contact area at each Gruen zone between the thigh pain group and the control group is shown in Figure 4. The thigh pain group had a significantly lower contact area in zone 2 (p = 0.014). Univariate analysis of risk and prognostic factors showed that an increased contact area in zone 2 (OR: 0.878, p = 0.028) reduced the risk for thigh pain. No significant correlation was found between gender, BMI, age, stem type (Accolade TMZF or Accolade II), stem size, CI, CFI, stem alignment (varus or flexion) or contact percentage in any of the Gruen zones, except zone 2. Table 4 presents the results of the final multivariate analysis of the risk factors for thigh pain, which revealed that CFI (OR: 0.336, p = 0.026) and zone 2 contact percentage (OR: 0.858, p = 0.026) are significant factors for the reduction of risk for thigh pain.

Comparison of the contact area at each Gruen zone between the thigh pain group and the control group. In all patients with both stems, the thigh pain group had significantly lower contact area in zone 2 (p = 0.014) and tended towards higher contact in zone 5 than in the control group. Among the patients who underwent THA with the Accolade TMZF stem, the thigh pain group had significantly lower contact area in zone 2 (p = 0.021). Similarly, among the patients who underwent THA with Accolade Ⅱ stem, the thigh pain group had significantly lower contact area in zone 2 (p < 0.001) and significantly higher contact in zone 5 (p = 0.042) than the no thigh pain group.
Multivariate logistic regression analysis of the risk and prognostic factors.
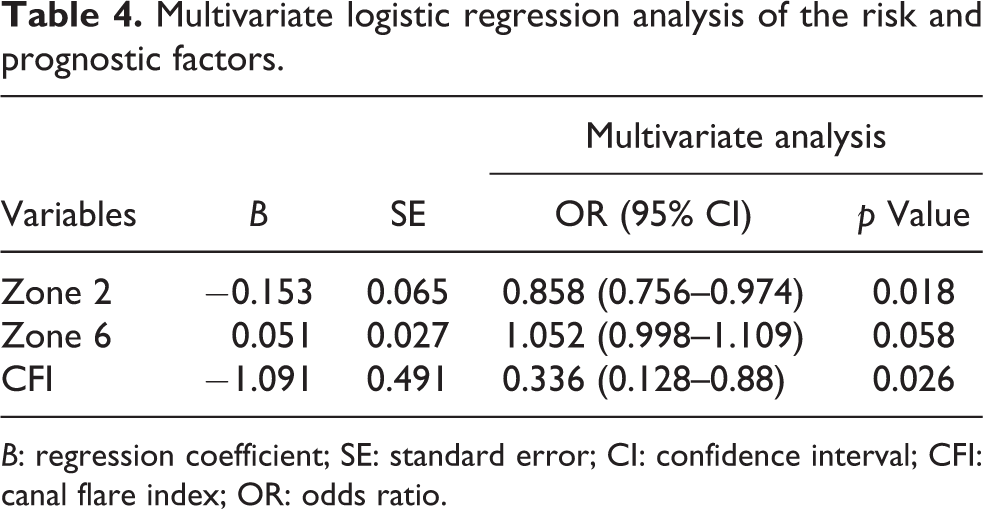
B: regression coefficient; SE: standard error; CI: confidence interval; CFI: canal flare index; OR: odds ratio.
Figure 5 presents radiographs and density mapping results of the thigh pain group as determined by the Accolade TMZF and Accolade II. Radiographs show that both stems acquired stable bone ingrowth; however, density mapping reveals a limited contact in zone 2 area of the stem.

Radiographs and density mapping of the thigh pain group. (a) Anteroposterior radiograph and (b) density mapping after THA using the Accolade TMZF stem. (c) Anteroposterior radiograph and (d) density mapping after THA using Accolade Ⅱ stem. THA: total hip arthroplasty.
Radiographic evaluation showed a femoral bone ingrowth with no stem subsidence in either hip. Cortical hypertrophy was detected in 31 patients (Accolade TMZF: 17 patients and Accolade II: 14 patients). The incidence of cortical hypertrophy did not differ significantly between thigh pain group (1 patient, 7.7%) and control group (29 patients, 15%; unpaired t-test, p = 0.70).
Discussion
This study showed a correlation between the contact state of the stem and thigh pain. Furthermore, the thigh pain group had a lower contact area in zone 2 than that of the control group. To the best of our knowledge, this is the first report to assess the correlation between thigh pain and the contact state of the stem using density mapping function.
The contact state between the stem and the bone was difficult to analyse because corticocancellous interface, which can be difficult to assess using plain radiography. 14 Sariali et al. and Hassani et al. used HipPLAN (Symbosis, Yverdon, Switzerland), a CT-based three-dimensional templating software, for the use of colour mode (namely density mapping) in preoperative planning. 21,22 The density mapping function was reported to be useful for quantifying the contact state between an implant and the femur. It was used in previous studies for clearly confirming cementless stem fit and fill parameters. 14,23 –26
Previous reports categorized the aetiology of thigh pain based on two mechanisms: stem tip micromotion at the bone–prosthesis interface 20,27 and excessive stress transfer to the stem tip. 3,28 Lavernia et al. 3 reported that the most widely accepted hypothesis for the development of thigh pain is abnormally high bone stresses at the tip of the femoral component. Stem tip pain was previously reported in revision total knee arthroplasty using a tibial stem extension component. 29,30 Inoue et al. showed that von Mises stresses are concentrated at the stem tip in an extension stem and concluded that stem tip pain may be caused by increased stress transfer to the bone at the tip of the stem extension. 23 Excessive stress concentrations are caused by a difference in the flexural rigidity between the stem and the bone. Sariali et al. 21 reported a significant reduction in femoral stress at the stem tip of a titanium implant compared to a cobalt–chromium implant. A large difference in flexural rigidity may induce stress concentration at the stem tip, resulting in thigh pain. 29 In our study, the thigh pain group had a lower contact area in zone 2 than those of the control group, based on density mapping analysis. In addition, all stems in the thigh pain group acquired stable bone fixation. The results were considered to be consistent with that of previous reports in which the aetiology of thigh pain was attributed to excessive stress transfer to the distal stem. If there is less contact between the cortical bone and the stem surface, it results in a greater difference between the flexural rigidity of the stem and bone. Furthermore, the stress on loading will be concentrated in the distal femur by contact with the cortical bone and stem distally. We hypothesized that greater stem contact in zone 2 area, which is the distal end of the porous coating, will prevent excessive stress concentration on the stem tip, possibly preventing thigh pain.
In our study, multiple logistic analysis demonstrated that a small CFI can be a significant risk factor for thigh pain. Engh et al. 20 reported on 243 patients with good preoperative radiographic bone quality who had an 11% incidence of post-operative thigh pain. Sixty-four patients with poor bone quality preoperatively experienced a much higher incidence (26%) of pain. Moreland and Bernstein 31 noted a markedly higher incidence of thigh pain in patients with preoperative radiographic osteopenia or femoral bone stock deficiency. The poor bone quality decreases Young’s modulus of bone elasticity and increases the mismatch of rigidity between the stem and bone. Therefore, a small CFI increased the risk for thigh pain because the stress at the stem tip increased. Finite element modeling may help to elucidate these relationships better.
To date, short femoral stems have been developed but are associated with a high prevalence of thigh pain. 5 Pepke et al. 32 reported that a short stem is more rigid than the conventional stem. Therefore, the indication of a short stem for poor bone quality must be considered carefully for preventing thigh pain.
There are many types of the cementless stem design, and the choice of the stem depends on the surgeon. If post-operative thigh pain, subsidence or stress shielding is predicted, the choice of the stem has to be considered during preoperative planning. Inoue et al. reported that density mapping with three-dimensional templating software could predict stem subsidence and stress shielding following cementless THA with a tapered wedge stem. 23 Altogether, our data suggest that to achieve improved treatment outcomes, appropriate preoperative planning is necessary to avoid the occurrence of thigh pain. In particular, zone 2 contact must be confirmed during preoperative planning while using a tapered wedge stem.
Large stem size, high elasticity modulus of the stem, varus stem position and osteoporosis of the proximal femur have been known as risk factors of thigh pain after cementless THA. 2,3,20 In this study, two different tapered wedge stems were used; therefore, the effect of the stem size was not clear. These two stems are made of different materials (TMZF and Ti-6Al-4 V). However, they were not considered as risk factors for thigh pain in this study although the level of thigh pain was higher in patients in whom Accolade TMZF was used than for patients in whom Accolade II was used. Furthermore, our results showed that the stem alignment was not a risk factor for thigh pain. Min et al. also reported that there was no thigh pain in cementless tapered wedge stems with varus alignment. 7 Varus alignment of the stem was associated with loosening of the cementless stem. 33 Therefore, we considered that if good osteointegration was acquired, the stem alignment should not be a risk for thigh pain.
Our study has some limitations. First, since this was a retrospective study that only considered patients with thigh pain, there may be potential bias despite our rigorous approach. Second, the definition of thigh pain was ambiguous. We diagnosed thigh pain by excluding all other sources of pain but included mild symptoms. Third, the time of the occurrence of thigh pain varied from 3 months to 3 years (Online Supplemental Table S2). Our hypothesis, which stated that there was a correlation between the initial contact state and thigh pain, does not provide an adequate explanation for this variation of the occurrence of thigh pain. Forth, we included two types of stems; however, the contact patterns were relatively similar for both the stem types.
Conclusion
In conclusion, our study demonstrated that the contact area in patients with thigh pain was significantly smaller in zone 2 than in patients without thigh pain. Our data identified a significant correlation between the initial contact area with the cortical bone and development of thigh pain, indicating that good contact in zone 2 of the stem may prevent thigh pain.
Supplemental material
Supplementary_data - The use of density mapping in the analysis of thigh pain after total hip arthroplasty in patients with well-fixed tapered wedge stems
Supplementary_data for The use of density mapping in the analysis of thigh pain after total hip arthroplasty in patients with well-fixed tapered wedge stems by Junya Yoshitani, Tamon Kabata, Yoshitomo Kajino, Takaaki Ohmori, Takuro Ueno, Ken Ueoka and Hiroyuki Tsuchiya in Journal of Orthopaedic Surgery
Footnotes
Author contributions
Study concept and design: JY and TK; Acquisition of data: JY and TN; Analysis and interpretation of data: JY, TK and YK; Drafting of manuscript: JY and TK and Critical revision: JY, TK, YK, TO, TU, KU and HT.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical standards
The institutional ethical committee on human research approved the current protocol.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.