
Abstract
The short tapered-wedge stem is popular worldwide because it potentially preserves more bone stock during total hip arthroplasty (THA). However, stem version mismatch may affect physiological stress distribution. In this study, we analyzed the correlations between periprosthetic bone mineral density (BMD) changes and anteversion mismatch in patients who underwent THA using a short tapered-wedge stem. The study included 44 patients (44 joints) who underwent THA with a Tri-Lock stem. At baseline and at 6 and 24 months postoperatively, the BMDs in the seven Gruen zones were evaluated using dual-energy X-ray absorptiometry. BMD changes and stem alignment, that is, anteversion and stem anteversion mismatch to the anatomical canal anteversion, were analyzed. Significant negative correlations were found between BMD changes and absolute anteversion error in Gruen zones 1 and 7 at 6 and 24 months postoperatively (zone 1, 6M; RR= −0.48, p < 0.001) (zone 7, 6M; RR= −0.46, p = 0.002) (zone 1, 24M; RR= −0.47, p = 0.001) (zone 7, 24M; RR= −0.40, p = 0.007). We further demonstrated that excessive stem anteversion mismatch to the anatomical canal anteversion causes stem point contact with the cortical bone in the distal portion and affected proximal periprosthetic BMD loss after THA. We recommend that the native anatomical anteversion angle should be used as a reference for inserting the tapered-wedge stems.
Introduction
Total hip arthroplasty (THA) has become a common procedure with excellent results for treating osteoarthritis, osteonecrosis, and rheumatoid arthritis of the hip. 1 Load bearing on periprosthetic bone is an important issue for maintaining bone strength. 2 Stress shielding causes poor bone density. 3 Stress shielding in the femur often occurs in the calcar region, because it is highly unlikely that the loading and stress distribution in the proximal femur will ever be replicated in the presence of an intramedullary metal prosthesis, 4,5 and this decrease in bone density may lead to aseptic loosening, stem subsidence, and periprosthetic fractures. 4,6 Therefore, implants should aim to replicate the physiological stress distribution. 7
Dual-energy X-ray absorptiometry (DEXA) is a well-documented method for monitoring patients after THA, 8,9 and it detects even small bone mineral density (BMD) changes around a stem. 10,11 DEXA is considered the most reliable method in assessing proximal femoral remodeling leading to implant fixation or periprosthetic bone stress shielding after THA. 12
Bone-preservation strategies involve the development of neck-preserving short stems designed to avoid stress shielding and increase periprosthetic bone formation. 3 The Tri-Lock BPS stem (DePuy Orthopaedics, Warsaw, IN, USA) is a short tapered-wedge stem with small shoulder shape, short anterior–posterior width, and short length. Similar short bone-preserving cementless stems have gained popularity, as they address some of the limitations of long stems. Compared with long stems, short stems potentially preserve more bone stock, which improves proximal load transfer, and have lower stress shielding. 13,14 We recently reported that periprosthetic BMD remained almost constant in the proximal femur, especially in Gruen zone 1, after THA with the Tri-Lock BPS stem. 15
We hypothesize that excessive change in femoral anteversion after prosthesis implantation may affect physiological stress distribution, leading to stress shielding. Therefore, in this study, we analyzed the correlations between periprosthetic BMD changes and changing of stem anteversion in patients who underwent THA with a short tapered-wedge stem.
Patients and methods
Patient characteristics
This prospective cohort study enrolled 44 consecutive patients (44 joints) with osteoarthritis (grade 4 according to the Tönnis classification) who underwent THA with the Tri-Lock BPS stem at our institution between January 2013 and November 2013. Patients with distorted proximal femoral anatomy, osteoporosis (lumbar spine BMD <0.8), or evidence of metabolic bone disease were excluded. To analyze the contribution of anteversion change, stems with malalignment of over 2° varus or valgus cases were also excluded from the study.
All procedures were performed using the mini anterolateral supine approach by a single senior surgeon at Kobe University Hospital. Postoperative follow-up included evaluation with DEXA, and clinical factors, including the Harris hip score (HHS), body mass index (BMI), and age at surgery, were assessed 24 months postoperatively.
DEXA measurement
In all cases, DEXA was performed using a DPX-L scanner (GE Lunar Corporation, Madison, WI, USA). DPX-L total body scans were performed using software version 1.35, which set the appropriate transverse speed at 16, 8, or 4 cm/s depending on the height of the subject. Patients were positioned supine with their leg in neutral position, with knee and foot support, to facilitate the scanning of the anterior–posterior projection of the proximal femur, including the area distal to the prosthesis using an edge-detection technique. The BMD was determined preoperatively and perioperatively in seven regions of interest based on the Gruen zones. 16 The values were expressed as areal BMD in grams per square centimeter. The BMD around the stem was assessed within 2 months postoperatively (baseline BMD) and at 6 and 24 months postoperatively. BMD changes were calculated by dividing each BMD value at 6 and 24 months postoperatively by the baseline BMD value.
Measurement of stem alignment
Preoperative and postoperative computed tomography (CT) scans from the pelvis to the knee joint were performed and transferred to a three-dimensional template software (Zed Hip; Lexi, Tokyo, Japan). Computer-aided design models of the implants were manually adjusted for postoperative multiplanar reconstruction in CT images. Stem anteversion and anatomical canal anteversion angles were measured with respect to the posterior condylar line axis of the femur. 17 We compared the anatomical canal anteversion and postoperative stem anteversion, and the anteversion error was defined as difference between the stem anteversion and the anatomical anteversion.
Contact situation between stem and cortical bone surface
The distance between the stem and the cortical bone surface was analyzed using the Zed Hip software. The color changed from red to blue according to the distance between the stem and the cortical bone surface. A green color indicates a distance <0.2 mm, and red or yellow colors indicate close contact between the stem surface and the cortical bone. Especially, red color indicated the stem surface contact with the cortical bone. Further, we analyzed the relationship between stem point contact and absolute stem anteversion error or BMD loss. The number of red color positive area according to Gruen zones was compared with anteversion error or BMD change.
Statistical analysis
All data are expressed as mean ± standard deviation unless otherwise indicated. The correlations between periprosthetic BMD changes and stem alignments were analyzed using Pearson’s correlation value (Figure 1). Intergroup comparisons were evaluated using Mann–Whitney U test (Figure 2). A p-value of <0.05 was considered significant.

(a) Correlations between periprosthetic bone mineral density changes and absolute stem anteversion error in the seven Gruen zones at 6 and 24 months postoperatively. Correlation coefficients and p-values are presented. Boldface values indicate p < 0.05. (b) Plotting data of periprosthetic bone mineral density changes and absolute stem anteversion error in the seven Gruen zones in zones 1 and 7 at (a) 6 and (b) 24 months postoperatively.

Influence of contact situation between the stem and the cortical bone surface on absolute anteversion error or periprosthetic bone mineral density changes in the Gruen zones 2, 3, 5, and 6 at 24 months postoperatively. (a) Comparison between stem contact situation and absolute anteversion error in Gruen zones 2, 3, 4, and 5. Columns indicate mean values of absolute anteversion error. (b) Comparison between stem contact situation and proximal periprosthetic bone mineral density changes in Gruen zones 2, 3, 4, and 5. Columns indicate mean values of proximal periprosthetic bone mineral density changes.
Ethics
The study protocol was approved by our institutional review board on September 8, 2011 (No. 1220), and informed consent for participation in the study was obtained from all participants.
Results
Patient characteristics and stem alignment
The mean patient age at surgery was 65.0 ± 10.3 years. At clinical evaluation performed 24 months postoperatively, the mean BMI was 23.8 ± 3.8 kg/m2 and HHS was 89.4 ± 9.2. The mean stem anteversion was 31.3° ± 9.6°, and the anatomical canal anteversion was 31.7° ± 11.3°. The mean absolute anteversion error (stem anteversion − anatomical canal anteversion) was 5.9° ± 5.9°.
Stem anteversion error correlated with proximal periprosthetic BMD loss
To analyze the influence of stem alignment on periprosthetic BMD changes, we compared the periprosthetic BMD changes and the stem anteversion error. Significant negative correlations were found between BMD changes and absolute anteversion error in Gruen zones 1 and 7 at 6 and 24 months postoperatively (Figure 1(a) and (b)). These findings indicate that stem version error affected proximal periprosthetic BMD loss.
Excessive version error causes stem point contact with cortical bone surface in the distal portion
To determine why absolute anteversion error negatively correlated with BMD changes, we analyzed the contact situation between the stem and the cortical bone surface (Figure 3). We showed subject-specific differences. In case 1, the absolute stem anteversion error was 21.8° (excessive stem anteversion) and the stem contact with the cortical bone was only seen in Gruen zones 3 and 7 (Figure 3, case 1). Meanwhile, in case 2, the stem anteversion error was only 2° and the stem contact with cortical bone was broad and encompassed Gruen zones 2–7 (Figure 3, case 2). Furthermore, in case 3, the absolute anteversion error was 15.1° (stem retroversion) and the stem contact with cortical bone was seen in Gruen zones 2, 3, and 7.
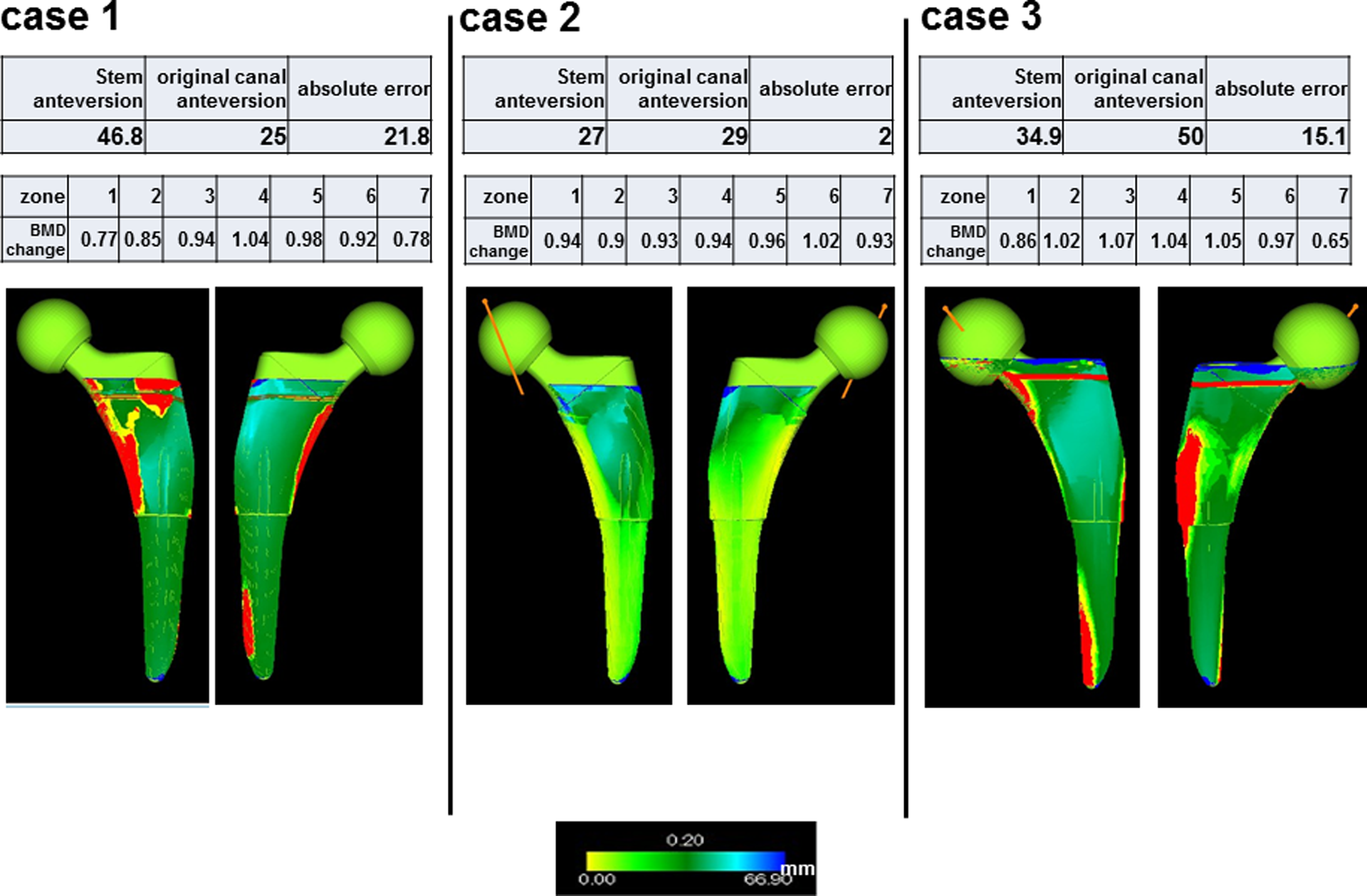
Three representative cases of contact between stem and cortical bone: (a) excessive anteversion, (b) neutral anteversion, and (c) retroversion. (Top) Degree of alignments. (Middle) Periprosthetic bone mineral density changes in the seven Gruen zones at 24 months postoperatively. (Bottom) Contact situation between stem and cortical bone surface.
The BMD in Gruen zones 1 and 7 at 24 months post-surgery showed a substantial loss in cases 1 and 3, but it was maintained in case 2 (Figure 3, cases 1 and 2). These findings indicate that excessive changing stem anteversion caused abnormal strain distribution on the cortical bone surface, leading to proximal BMD loss.
Stem contact with femoral bone in distal portion causes proximal periprosthetic BMD loss
To analyze the relationship between stem point contact and BMD loss, we analyzed the relationship between the situations of stem point contact with the femoral bone, periprosthetic BMD changes, and stem anteversion error. The mean absolute anteversion error was significantly lower in the group with cases of stem point contact with femoral bone in Gruen zone 3, but not in the other Gruen zones. We also showed that the mean BMD change was significantly lower in the group with cases of stem point contact with femoral bone in Gruen zone 3, but not in the other Gruen zones. These results indicate that excessive anteversion error causes stem point contact with the femoral bone in the distal portion, leading to proximal periprosthetic BMD loss.
Discussion
Previous works demonstrated that contact force was dependent on subject-specific geometry and that specificity influenced stress distribution in the periprosthetic bone. 18,19 In other words, stress distribution in the periprosthetic bone was influenced not only by subject-specific geometry but also by stem alignment. Bah et al., 20 in a finite element method study, reported that stress distribution in periprosthetic bone was dependent on stem alignment, especially anterior–posterior and varus–valgus alignments. Vresilovic et al., 21 in a radiographic study, reported that varus alignment caused early stem loosening because of poor seating of the femoral prosthesis with decreased bone ingrowth. The relationship between varus–valgus alignment and stress distribution in the periprosthetic bone has been established well in biomechanical studies. 21 –25 However, the relationship between anteversion mismatch and stress distribution in the periprosthetic bone remains unclear.
The results of the present study indicate that excessive mismatch in stem anteversion is correlated with postoperative periprosthetic proximal BMD loss. Further, excessive anteversion error causes stem point contact with the femoral bone in the distal portion, leading to proximal periprosthetic BMD loss. We recently reported significant negative correlations between stem anteversion and BMD changes in Gruen zones 2, 3, 4, and 6, 26 and the result was consistent with that of other reports. 27 However, we have learned that excessive decreased anteversion also caused periprosthetic BMD loss in the current study. The results may be explained by stem contact force with cortical bone. Umeda et al. 27 reported that in vitro strains decreased in implanted femurs relative to intact femurs and that increasing anteversion increased strains anteriorly and posteriorly near the distal tip of the implant. We have demonstrated that not only excessive increased stem anteversion but also stem retroversion increased contact area with the distal part of stem, leading to loss of proximal bone density. Therefore, the abnormal stress distribution may be the reason for proximal periprosthetic bone loss in cases of excessive mismatch in stem anteversion.
The limitation of this study is the lack of presentation of direct evidence of periprosthetic bone stress distribution after THA. We must therefore analyze the simulation of stress distribution in the periprosthetic bone.
In conclusion, excessive mismatch in stem anteversion affects proximal periprosthetic BMD loss after THA. The native anatomical anteversion angle should be used as a reference for inserting the tapered-wedge stems.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.