
Abstract
Aim:
This study aimed to assess the relationship between the three-dimensional (3D) alignment of short tapered-wedge cementless stems and bone mineral density (BMD) changes in patients followed up for 5 years after total hip arthroplasty (THA).
Methods:
We retrospectively analysed the hips of 52 patients who underwent THA using short tapered-wedge cementless stems at our institution from 2013 to 2016 with complete 5-year follow-up data. We evaluated the relationship between stem alignment, measured using a 3D-templating software, and BMD changes in the 7 Gruen zones.
Results:
After 1 year, significant negative correlations between varus insertion and a decrease in BMD in zone 7 and between flexed insertion and decreases in BMD in zones 3 and 4 were noted. After 5 years, significant negative correlations between varus insertion and a decrease in BMD in zone 7 and between flexed insertion and decreases in BMD zones 2, 3, and 4 were observed. With increased amounts of varus/flexion stem alignment, the amount of BMD loss decreased. There was no correlation between anteverted stem insertion and changes in BMD levels.
Conclusions:
Our data showed that stem alignment affects BMD based on 5-year follow-up data after surgery. Careful observation is necessary, especially when using short tapered-wedge cementless stems, as stem alignment may affect changes in BMD levels more than 5 years after surgery.
Keywords
Introduction
Primary total hip arthroplasty (THA) is a widely used orthopaedic procedure for reducing pain and restoring joint function in patients with hip dysfunction caused by osteoarthritis, femoral neck fracture, avascular necrosis, dysplasia, and inflammatory arthritis. 1
In recent years, short tapered-wedge stems have been increasingly used worldwide for THA procedures due to their surgeon-friendly and bone stock-preserving features. Short tapered-wedge cementless stems have been associated with favourable short-term clinical outcomes.2–7 In addition, short stems are suitable for minimally invasive procedures, as they can be inserted through a small incision, and mini-incision THA reportedly results in less blood loss and pain and a shorter hospital stay than standard-incision THA.8,9
Nevertheless, some studies have reported that mini-incision THA results in malalignment and poor fixation owing to the narrow surgical field.10,11
If the initial fixation of the femoral component is not ideal, stem subsidence, severe stress shielding, and aseptic loosening may occur in the early postoperative period, requiring revision THA procedures. 12 Furthermore, stress shielding results in low bone mineral density (BMD). 13 Load, normally carried by the proximal femur, is now shared by the implant and the bone that results in a marked decrease in the cortical strain in the proximal femur. Therefore, stress shielding is the consequence of mechanical phenomena. Furthermore, the percentage of load carried by the prosthesis depends on a number of factors such as the prosthesis size, stem design, material composition, stem alignment, stem-stiffness, fixation system, patient activity level, age, the quality and the quantity of the bone structure. These factors can cause differences in the percentage of stress shielding. The decrease in BMD may lead to aseptic loosening, stem subsidence, and periprosthetic fractures.14,15
Stem alignment is commonly analysed by plain radiographs; however, precise alignment cannot always be measured, as the appearance of the stem changes depending on the femoral rotation in 2-dimensional (2D) imaging. Therefore, 3D templating software is frequently used to obtain precise measurements. Several reports have described the relationship between stem alignment and BMD changes using 3D templating software;16,17 however, they had short follow-up periods, and no medium-term outcomes have been described.
This study aimed to assess the relationship between stem alignment as measured using a 3D-templating software and the changes in periprosthetic BMD, as well as the clinical outcomes in patients followed up for 5 years after THA with short tapered-wedge cementless stems.
Patients and methods
Study design
This was a retrospective single-centre cohort study. The study protocol was approved by the institutional review board. The requirement for informed consent was waived because of the retrospective nature of the study.
Study population
Between September 2013 and February 2016, 93 primary cementless THAs with a short tapered-wedge stem (Tri-Lock Bone Preservation Stem [BPS]; DePuy Synthes, Warsaw, IN, USA) were performed in 93 patients at our hospital. In this study, only patients who had been followed up for at least 5 years and had available clinical and radiological data were included.
Consequently, 52 hips from 52 patients (47 women and 5 men) were analysed. Data was retrieved from electronic medical records.
All patients had been diagnosed with osteoarthritis without prior hip surgery (21% primary osteoarthritis and 79% developmental dysplasia of the hip), and THA was performed via the modified Watson-Jones approach in the lateral position by a single experienced surgeon. Cancellous bone removal in zone 7 was not performed, and conventional rasps, instead of compactors, were used during the femur-rasping procedure.
Outcome measurements
We evaluated the clinical results by comparing the preoperative Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) score with the scores recorded at 3 months and at 1, 2, 3, 4, and 5 years after surgery. Occurrences of dislocations, infections, loosening, and all complications requiring revision arthroplasty were documented.
We further evaluated radiological outcomes based on the preoperative taper angle of the proximal femur, intramedullary canal shape, 18 and femoral offset, 19 stem fixation, 20 spot welds, cortical hypertrophy, and radiolucent lines annually after surgery. All patients underwent computed tomography (CT) (from the pelvis to the femur) in the supine position before surgery and 3 months postoperatively. Preoperative taper angle and femoral offset were measured using CT-based 3D templating software (ZedHip, LEXI Co., Ltd., Tokyo, Japan).
All preoperative planning and postoperative evaluations of stem alignment had been completed using CT-based 3D templating software and were built on the surface models according to the following definitions. We defined the femoral axis as the line passing through the centre of the third, fourth, and fifth portions among the 14 equally sized sections of the femur. The femoral axis was reflected in the stem in the coronal and sagittal planes. We defined varus or valgus, as the angle between the femoral axis reflected on the coronal plane of the stem and the stem axis on the coronal plane of the stem; flexion or extension, as the angle between the femoral axis reflected on the sagittal plane of the stem and the stem axis on the sagittal plane of the stem; and varus or flexion, as the varus or flexion angle of the stem axis against the femoral axis in the defined coordinate plane. For anteversion and retroversion, we used the coordinate system recommended by the International Society of Biomechanics (ISB). 21 The ISB coordinate plane included 3 points: the centre of the femoral head and the medial and lateral condyles of the femur. Anteversion was defined as the angle between the stem and the ISB coordinate plane.
BMD around the stem was measured using dual-energy x-ray absorptiometry (DEXA) at 3 weeks (baseline), 3 months, and 1, 2, 3, and 5 years after surgery. The BMD changes in the Gruen zones were calculated by the percentage change from baseline. 22 Further, we analysed the relationship between 3D stem alignment (varus-valgus, flexion-extension, and anteversion-retroversion) and BMD changes in the Gruen zones at 1, 2, 3, and 5 years after surgery. As a sub-analysis, we further analysed the BMD changes in the Gruen zones separately for patients aged ⩽70 years (n = 25) and those aged ⩾71 years (n = 27), as well as for male (n = 5) and female patients (n = 47).
Statistical analysis
Continuous variables are presented as means (range), whereas categorical variables are presented as absolute frequencies and percentages. The Mann-Whitney U-test was used to compare WOMAC scores and BMD changes between patients aged ⩽70 years and those aged ⩾71 years, as well as male and female patients. The Bonferroni correction was used to account for the fact that there were multiple comparisons of BMD changes between patients aged ⩽70 years and those aged ⩾71 years, and male and female patients. Spearman’s coefficient was used to analyse the relationship between post-operative stem alignment (flexion-extension, varus-valgus, and anteversion-retroversion) and the changes in BMD levels in the 7 Gruen zones. Inter-observer and intra-observer variabilities (using 3D computed tomography [CT] template software for stem alignment) were assessed using the interclass correlation coefficient of the last 10 consecutive patients and two blinded observers. Measurements were repeated every 2 months.
Statistical significance was set at p < 0.05. Statistical analysis was performed using IBM SPSS Statistics for Windows, version 26.0 (IBM Corp., Armonk, NY, USA).
Results
Patients’ mean age at surgery, body mass index, and follow-up period were 70.4 (56–84) years, 24.5 (17.2–34.3) kg/m2, and 69.7 (60–85) months, respectively.
The mean WOMAC score improved significantly from 44.1 (20–74) points, pre-operatively, to 7.1 (0–29) points, 1 year after surgery (p < 0.001); however, there were no significant differences between the scores at 1 and 5 years post-surgery (p = 0.817). Neither dislocation, infection, aseptic loosening, nor any other complications requiring revision arthroplasty were noted.
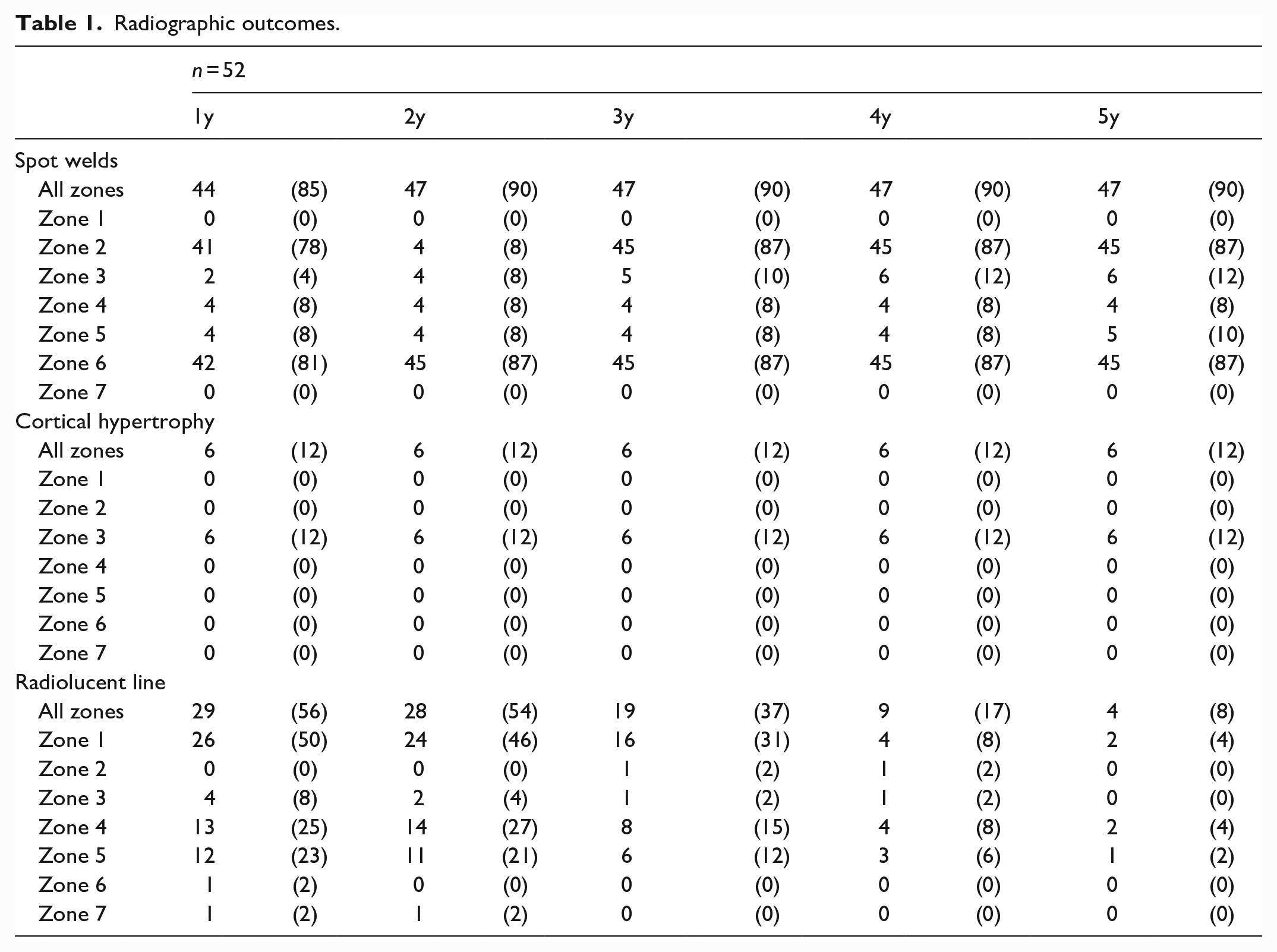
The mean taper angle of the proximal femur was 129° (121–137). The intramedullary canals were stovepipe-shaped in 5 hips and champagne flute-shaped in 2 hips. The mean femoral offset was 36.7 mm (27.2–53.2). None of the stem fixations were unstable, and biological fixation of the stem was achieved in all cases. Spot welds frequently appeared in Gruen zones 2 and 6, whereas cortical hypertrophy appeared only in zone 3 (Table 1). Radiolucent lines appeared in 50% of the hips in zone 1, 1 year postoperatively. Regardless, their occurrence markedly decreased to 3.8% after 5 years.
Radiographic outcomes.
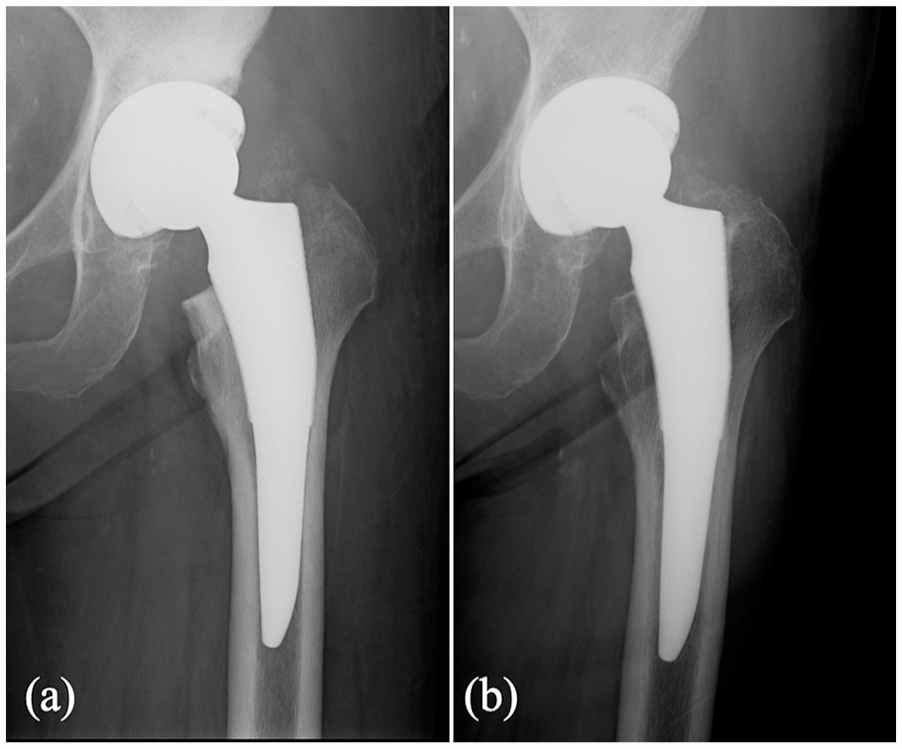
The BMD in zone 7 showed the largest decrease from baseline over 5 years (3 months, 11%; 1 year, 19%; 2 years, 20%; 3 years, 20%; and 5 years, 26%). The BMDs in zones 1 and 7 continued to decrease every year after surgery (Figure 1; Table 2). Plain radiography of the typical case with 20% BMD decrease in Gruen zone 7 is shown in Figure 2, and that of the case with more than 50% BMD decrease in Gruen zone 7 is shown in Figure 3.
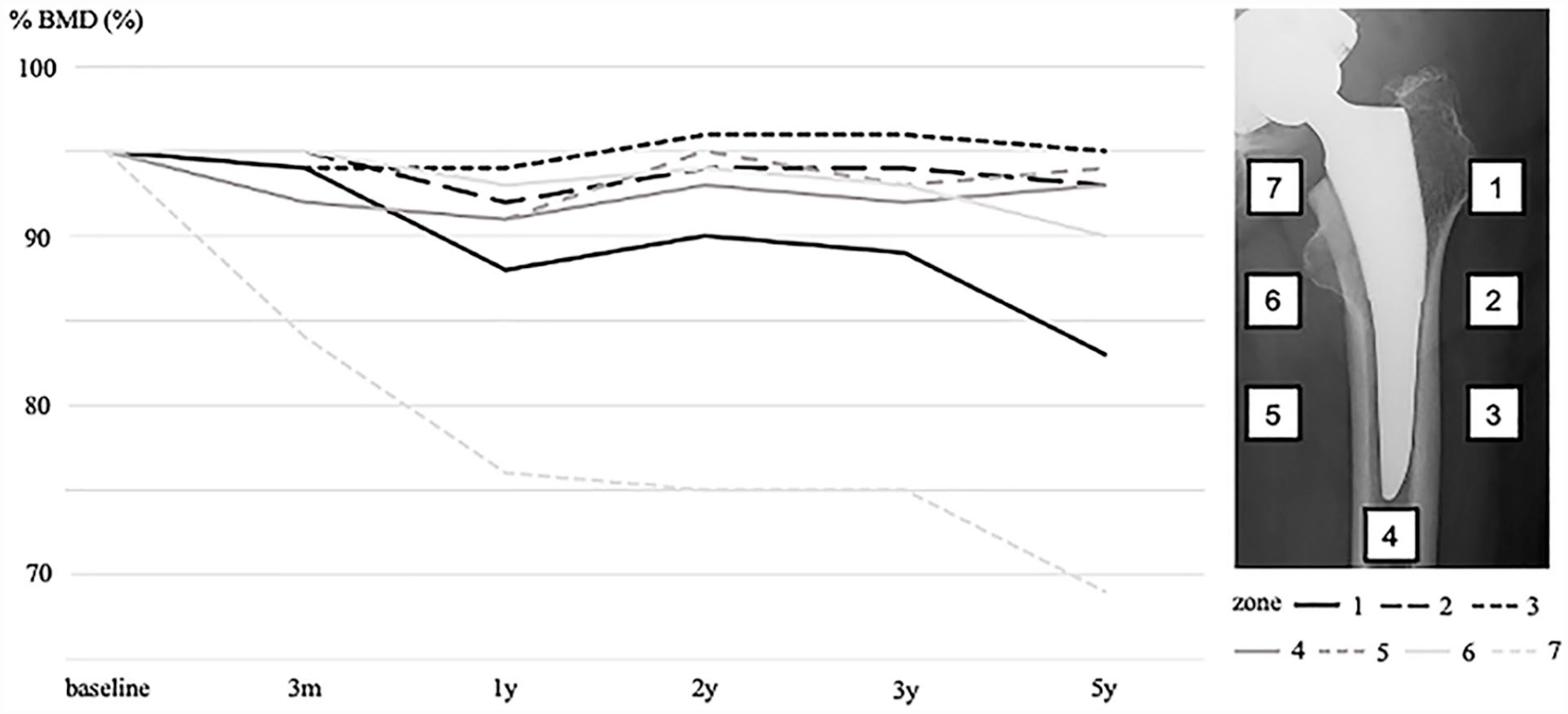
Changes in bone mineral density (BMD) in each Gruen zone.
The BMD changes in Gruen zone.
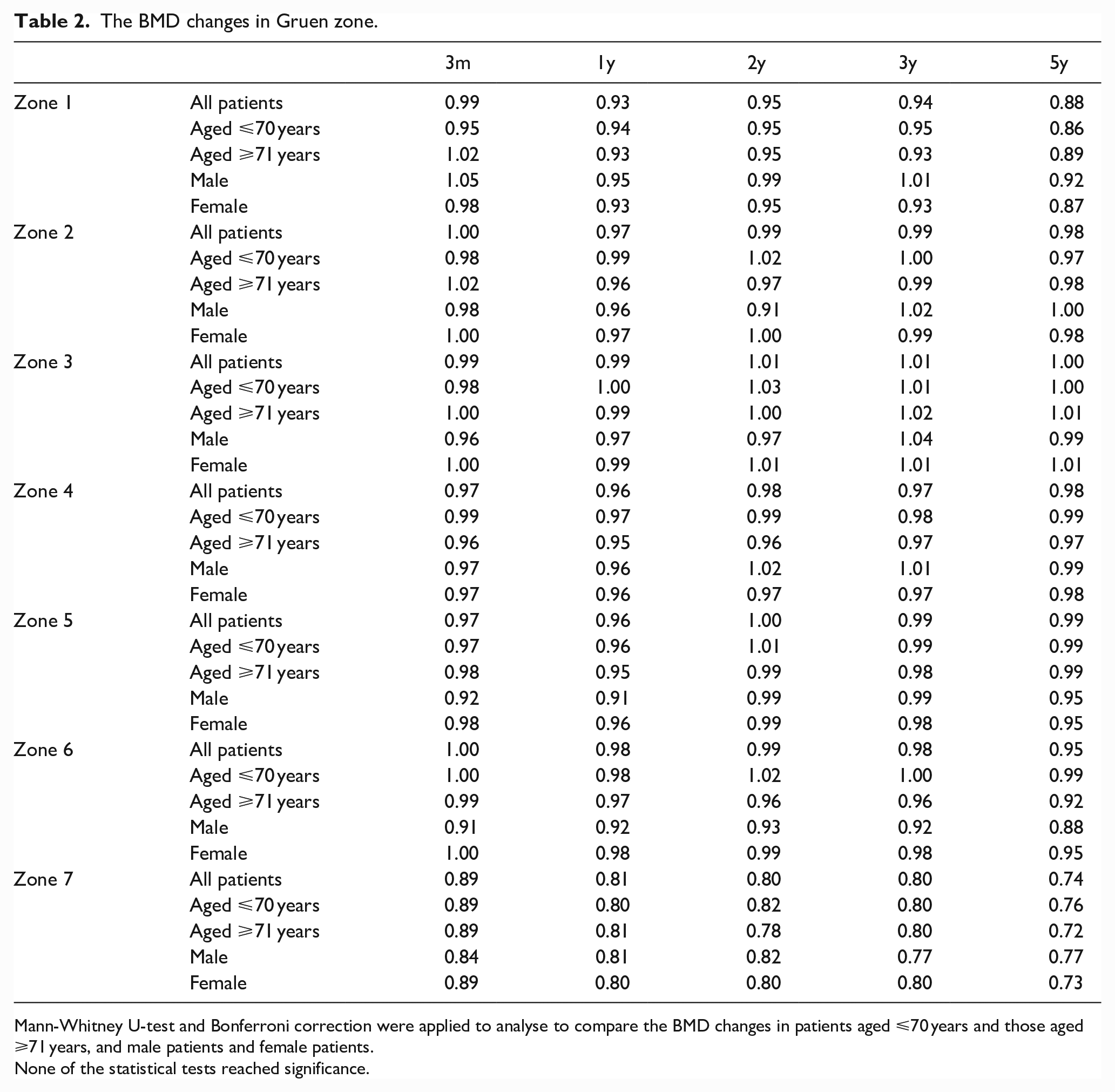
Mann-Whitney U-test and Bonferroni correction were applied to analyse to compare the BMD changes in patients aged ⩽70 years and those aged ⩾71 years, and male patients and female patients.
None of the statistical tests reached significance.
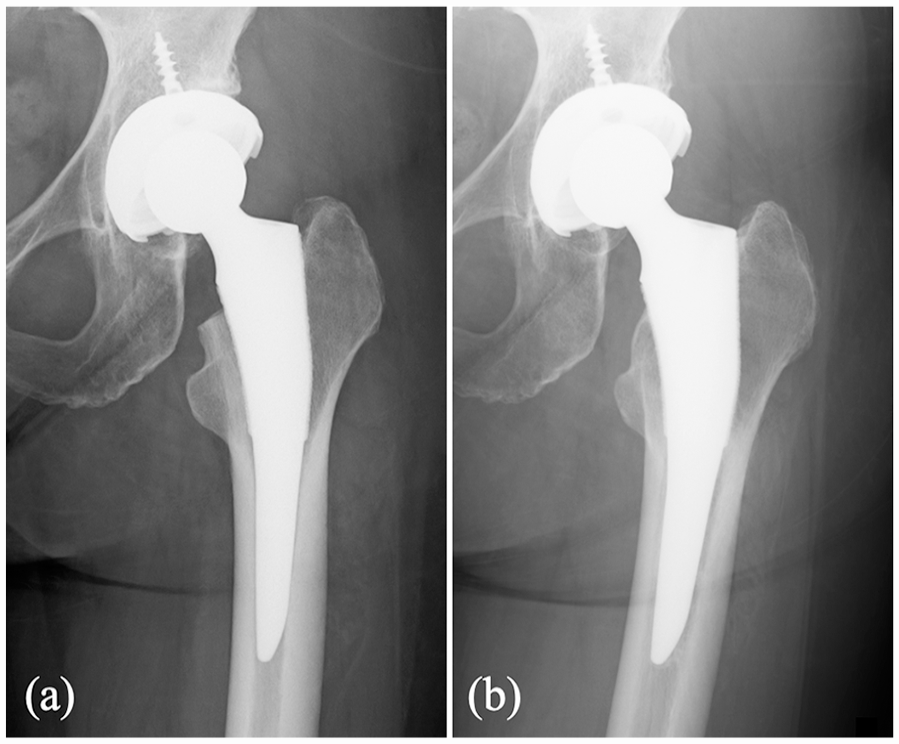
Plain radiography of a typical case with 20% BMD decrease in Gruen zone 7: (a) 3 weeks postoperatively and (b) 5 years postoperatively.
Plain radiography of a case with >50% BMD decrease in Gruen zone 7: (a) 3 weeks postoperatively and (b) 5 years postoperatively.
The interclass correlation coefficients between the two blinded observers for measurements of the varus, flexion, and anteversion angles were 0.99 (95% confidence interval [CI], 0.97–1.00; p < 0.001), 0.98 (95% CI, 0.92–1.00; p < 0.001), and 0.99 (95% CI, 0.94–1.00; p < 0.001), respectively. The interclass correlation coefficients between the first and second measurements by 1 observer for measurements of the varus, flexion, and anteversion angles were 0.99 (95% CI, 0.99–1.00; p < 0.001), 0.98 (95% CI, 0.94–1.00; p < 0.001) and 0.99 (95% CI, 0.96–1.00; p < 0.001), respectively. The mean alignment of the femoral stem was 2.1° varus (−3.0 to 7.0°), 3.6° flexion (−4.9 to 7.4°), and 25.4° anteversion (−2.5 to 50.9°).
After 1 year, significant negative correlations between varus stem insertion and a decrease in BMD in zone 7 and between the flexed insertion and decreases in BMD levels in zones 3 and 4 were noted. After 5 years, there were significant negative correlations between varus stem insertion and a decrease in BMD in zone 7 and between flexed insertion and decreases in BMD in zones 2, 3, and 4 (Table 3). There was no correlation between an anteverted stem insertion and changes in BMD levels. A more varus stem alignment was associated with a lower decrease in BMD in zone 7 throughout the 5 years. All significant correlations between stem alignment and BMD were weak to moderate; no strong correlations were observed.
Correlations between 3D stem alignment and BMD changes in Gruen zone.
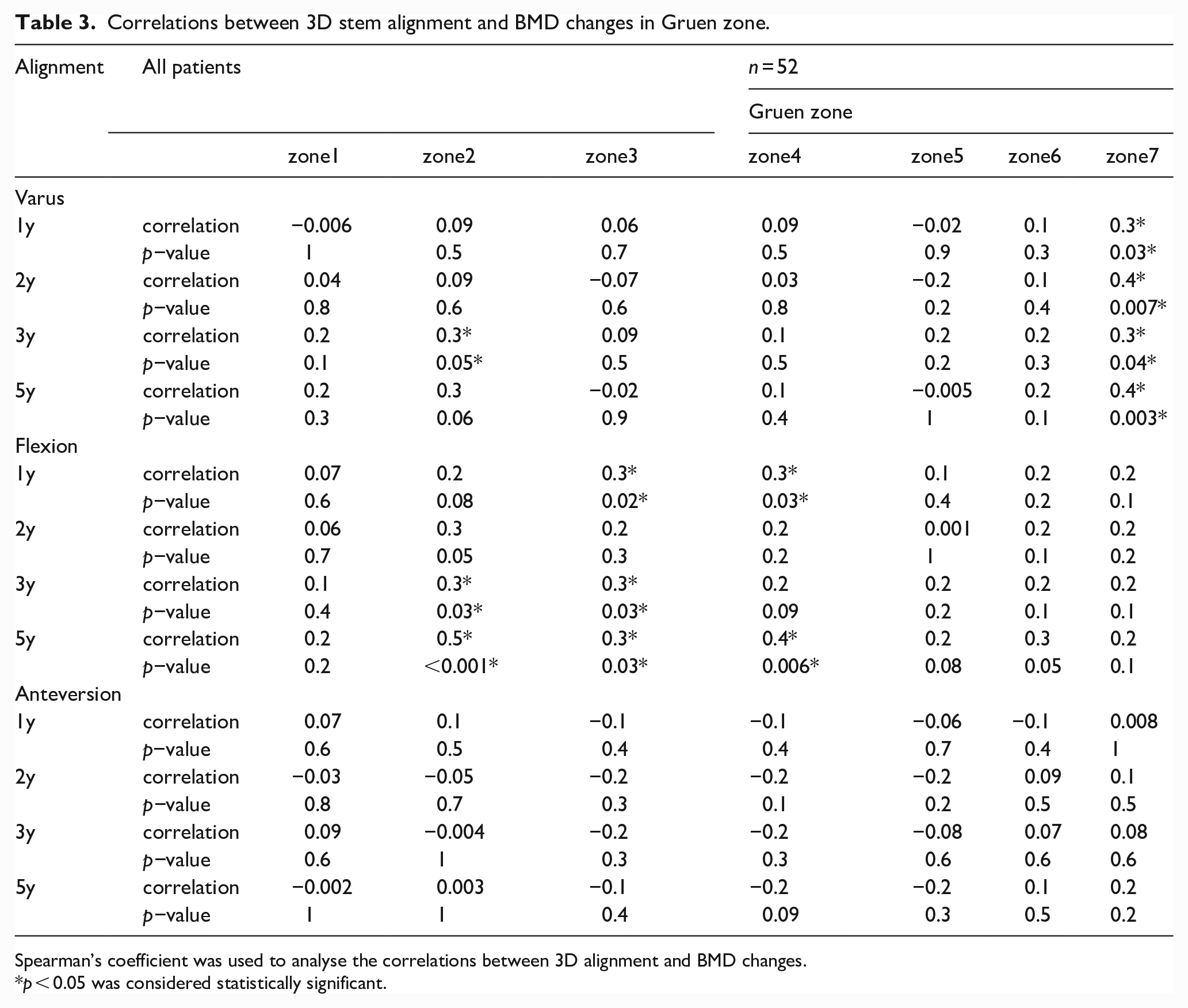
Spearman’s coefficient was used to analyse the correlations between 3D alignment and BMD changes.
p < 0.05 was considered statistically significant.
Based on the sub-analysis results, there were no significant difference in the BMD changes in each Gruen zone between patients aged ⩽70 years and those aged ⩾71 years, or between male and female patients (Table 2).
Discussion
The short- and medium-term clinical outcomes of tapered-wedge stems have been reported to be excellent.2–7 It is important to note that some studies have found that tapered-wedge stems increase the risk of failure of osteointegration and progressive stem subsidence owing to the distal fixation of the tapered-wedge stem and the mismatch between the implant and femur.12,23,24 In this study, WOMAC scores significantly improved after THA, and no cases of subsidence or complications were noted.
Previous reports have similarly used the Tri-Lock BPS that we implanted in our patients. Ulivi et al. 6 reported that the Harris hip score (HHS) of 159 patients significantly improved after a mean follow-up of 5.7 years, with a survival rate of 99%. Albers et al. 7 found that the HHS of 126 patients significantly improved after a mean follow-up of 5 years, with a survival rate of 99.2%. Based on these results, the medium-term clinical outcomes using Tri-Lock BPS are excellent.
In this study, we observed radiolucent lines in 55.8% of all hips 1 year after surgery, half of which (50%) occurred in zone 1. A previous study using the Tri-Lock BPS noted the occurrence of radiolucent lines in zone 1 in 42.1% of the operated hips at 2.9 years after surgery, 25 which is similar to our results. We also found a marked decrease in the frequency of radiolucent lines in 9.5% of patients, 5 years postoperatively. We speculate that the radiolucent lines, particularly those in zone 1, are related to the characteristics of the Tri-Lock BPS stem rather than to loosening.
BMD decreased most significantly in the Gruen zone 7 at all follow-up assessments in our patients. Inaba et al. 26 investigated the periprosthetic BMD changes in 3 types of stems (i.e., fit-and-fill type stems, Zweymüller type stems, and short tapered-wedge type stems), and similarly found the largest BMD decrease in zone 7 in all stem types, 3 years postoperatively. They reported that short tapered-wedge stems showed a BMD loss of approximately 20%, compared with 30% in fit-and-fill and Zweymüller stems. We also used short tapered-wedge stems and found a BMD loss in zone 7 of 20%, 3 years after surgery, suggesting that these stems result in lower BMD loss than fit-and-fill and Zweymüller stems. Nonetheless, BMD levels in zones 1 and, especially, 7 continued to decrease up to 5 years postoperatively. Although short tapered-wedge stems were originally designed for proximal fixation, they are often fixed more distally from the proximal femur in actual practice, thereby increasing the likelihood of occurrence of BMD decreases in zones 1 and 7. Tapaninen et al. 27 investigated periprosthetic BMD after THA using a proximally fixed cementless stem and reported that BMD continued to decrease for up to 10 years postoperatively in zones 1 and 7. Thus, periprosthetic BMD levels may continue to decrease in the long term, and careful follow-up is necessary for patients who undergo cementless THA. Another new finding of this study was that there was no significant difference in BMD between patients aged ⩽70 years and those aged ⩾71 years. Although it is generally believed that BMD decreases with age, these results suggest that periprosthetic BMD decreases regardless of age.
Throughout the 5-year follow-up, we found a significant negative correlation between varus insertion and a decrease in BMD levels in zone 7. The varus alignment of the stem may have led to contact with the femur medioproximally, thus resulting in BMD changes. Although the varus alignment of the stem may be advantageous for BMD decrease, monitoring is important as poor outcomes following varus insertion of cementless stems have been reported. 28 In this study, we revealed that stem alignment continued to affect changes in BMD levels for 5 years after surgery. Consequently, we believe that further investigation of long-term outcomes is necessary.
The main strength of this study was the evaluation of stem alignment using a 3D-templating software with CT scans. Some studies have reported a relationship between stem alignment and BMD changes using plain radiographs; 29 however, radiography does not allow precise stem-alignment measurements. Thus, to our knowledge, this is the first study to assess the relationship between 3D-measured stem alignment and BMD changes in the medium term.
This study has some limitations. First, technical errors may have occurred during the matching of the preoperative and post-operative CT data to analyse implant alignment. We assume that our matching system error was relatively small because the reference points were not influenced by post-operative metallic halation. Second, BMD measurements are not perfectly reproducible, although they were consistently performed in accordance with the manufacturer’s recommendations. 30 In addition, there was a high degree of variability in the skills of the technicians who performed the tests and the clinicians who interpreted the results of BMD measurements. 31 Third, all surgeries in this study were performed by a single surgeon at one institution. Therefore, our results might be influenced by the surgeon’s individual surgical skills and cannot be generalized. Fourth, BMD was only evaluated in the anteroposterior plane. If the sagittal plane was also evaluated, clearer relationships between stem alignments, especially between flexed insertion and BMD changes, might have been revealed. Furthermore, we did not evaluate the BMD of the spine, so we were unable to determine overall bone loss. Fifth, the baseline BMD was defined as the BMD at 3 weeks postoperatively, not the pre-operative BMD. However, periprosthetic BMD studies are often compared postoperative BMD to that of the immediate postoperative period, not that of the preoperative period, because post-operative conditions are different from pre-operative conditions due to implant insertion.16,17 Sixth, this study had a retrospective study design, and nearly half of otherwise eligible patients were excluded because the complete data were not available, which introduced significant selection bias. Seventh, we used Tri-Lock BPS, which is made of Ti-6AI-4V, but other materials may give different results. Finally, the number of hips analysed was small in this study; therefore, we were unable to analyse the relationship between stem size and periprosthetic BMD. Thus, further research in larger cohorts is required. Despite these limitations, we believe that our results demonstrate the potential of a 3D-templating software to define the relationship between stem alignment and changes in BMD around the stem, which can be helpful after THA.
Conclusion
To our knowledge, this is the first study to demonstrate that stem alignment affects periprosthetic BMD beyond 5 years after THA. The clinical results of short tapered-wedge cementless stems, 5 years postoperatively, were excellent; however, careful observation is necessary, as the stem alignment may affect BMD changes more than 5 years after surgery. Long-term studies on the relationship between BMD changes and 3D-stem alignment in larger cohorts are needed to validate our findings.
Footnotes
Acknowledgements
We thank Shingo Maeda, Hitomi takuma, and Shogo Shibata for their assistance in the orthopaedic surgeries in Shiraniwa Hospital Joint Arthroplasty Centre.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.