
Abstract
Rapid prototyping (RP), also known as three-dimensional printing (3DP), allows the rapid conversion of anatomical images into physical components by the use of special printers. This novel technology has also become a promising innovation for spine surgery. As a result of the developments in 3DP technology, production speeds have increased, and costs have decreased. This technological development can be used extensively in different parts of spine surgery such as preoperative planning, surgical simulations, patient–clinician communication, education, intraoperative guidance, and even implantable devices. However, similar to other emerging technologies, the usage of RP in spine surgery has various drawbacks that are needed to be addressed through further studies.
Keywords
Introduction
Spine surgeons deal with a wide range of complex pathologies of spinal column including deformities, tumors, infections, trauma, and degeneration. All of these problems have different complicated aspects that need to be investigated in detail using various sophisticated techniques. Sound knowledge of anatomy and identification of landmarks, which involve a long and steep learning curve, are some of those crucial requirements for a proper surgical intervention. Intraoperative techniques for visualization of the deformed spine including preoperative computerized tomography (CT)-based, fluoroscopy-based, and three-dimensional (3D) fluoroscopy have been used as navigating techniques that contribute to the analysis. However, all these techniques involve prolonged surgery duration, high radiation exposure to patients as well as operating staff, and high cost. 1 Rapid prototyping (RP) is a developing approach that sheds light on most of these issues.
RP, also known as three-dimensional printing (3DP), is the “third industrial revolution” as pointed out by futurist Jeremy Rifkin. It has been developed as a promising innovation for many disciplines including medicine. Recently, 3DP has started to be used as a groundbreaking modality in training and planning of surgical procedures by the late 1990s. 2 In the industry, widespread computer-aided design and computer-aided manufacturing produced momentum and desire to extract 3D images into physical models. The transfer of the data obtained from 2D imaging to a 3D haptic mannequin constructs this revolution’s basis. This conversion includes miscellaneous available techniques such as stereolithography, selective laser sintering, direct laser metal sintering, two-photon polymerization, laminated object manufacturing, 3D printing, 3D plotting, polyjet inkjet technology, fused deposition modeling, vacuum casting, and milling. 3 The 3DP’s principle for building up models layer-by-layer with material deposition has led to the impeccable construction of detailed anatomical models or complex, which cannot be reproduced even by sophisticated milling machines. 4 The layering technique includes a liquid that is sprayed through the inkjet printer nozzles, thus forming a solid thin slice over and over again until the intended object is completed. As a result, not only the external details but also the details of its internal contour geometry can be transferred to the model created from CT images by the 3DP machine. 4 The 3D printing methods include selective laser melting, laser sintering, fused deposition modeling, stereolithography, laminated object manufacturing, and fused filament fabrication. 5,6 Materials to be used in 3DRP techniques also vary according to the need such as thermoplastics, which are used commonly in fused filament fabrication, whereas titanium and cobalt chrome alloys in selective laser melting. 5,7,8
One of the major advantages of producing impeccable constructions of complex structures with such an easy way by even nonprofessions is that it can be done in a center that has one of these smart printers. There is no need for a specific type of workshop or a long-term training for basic access. This encouraged the utilization of these devices and the production of 3D spine mannequins in the daily practice of several institutes. Assessing the complex deformities with haptic sensation rather than 2D images on computers has provided the spinal surgeons with realistic anatomical demonstration of the deformities either preoperatively or intraoperatively. Implementation of 3DRP technology in complex spinal deformity surgery ensured enhanced communication between the surgical team by improved envisioning of the deformity by each team member. These features of 3DRP has been reported to have several clinical benefits, such as improved diagnosis and decreased surgical duration, blood loss, and fluoroscopy time as well as costs by eliminating intraoperative navigation usage in complex spinal procedures. 9,10 These procedures are mostly complex reconstruction deformity cases requiring anterior column reconstruction with anterior supports performed with ready-to-use implants which bring the risk of implant dislodgement following the inaccurate fit. Promisingly, patient-specific implant production has been started to be used in very rare extensive reconstruction procedures to take advantage of even load distribution and superior osseointegration. 11 –15
There are many ways to use 3DP in spine surgery. Education of patient and health-care professionals, preoperative applications like surgical planning, and intraoperative applications such as patient-specific guides and implants are just some of its implications in this field of medicine. The current review article aims to discuss the pros and cons of this emerging technology based on current literature.
3DP models, training, and preoperative planning
3DP models have been appeared to improve health understudy instruction. Contrasted with cadaveric examples, 3DP models accompany negligible well-being and security, medicolegal, and accessibility concerns. 16,17 While it is far-fetched, 3DP models can replace cadavers as learning instruments, which are likely to enhance corpses to lessen costs and show uncommon anatomical structures.
Wu et al. 18 created the 3D models of spinal, pelvic, and upper and lower extremity fractures using CT images taken from four patients. Ninety medical students randomly divided into two groups, one of which had only radiological images and the other group had 3D models, were asked questions about fracture types. As a result, it was shown that students with 3D models had significantly higher scores in questions about spinal and pelvic fractures. The authors reported that 3D models improve understanding in student education, especially in complex anatomical regions.
Training residents of the pedicle screw instrumentation procedure in the surgery room is restricted by virtue of the well-being and careful proficiency. Park et al. 19 assessed the instructive impact of utilizing a genuine size 3D-printed spine model for training residents of the freehand pedicle screw instrumentation strategy. In their study, residents who had no experience of pedicle screw insertion were told by a senior specialist, and every resident inserted pedicle screws for each model. CT images of the spine models were acquired to assess screw accuracy. As a result, 3D spine models can be a successful device for training residents of the freehand pedicle screw instrumentation. Despite all their positive features, they have stated in their studies that the “osseous feeling” in 3D-printed models is different. Some studies remarked that 3D models cannot mimic the texture of human tissues (e.g. the discs, ligaments, and neurovascular structures) and blood which makes 3D-printed spine models nonideal training devices. 20,21
On the other hand, 3D models can be a perfect instrument for improving patient–doctor communication. 3D models give more material and instinctive representation of anatomy than standard imaging methods. All things considered, they may give patients as well as their families with a superior comprehension of the pathoanatomy, surgery, and treatment process. The utilization of 3D models has been related to better doctor–patient relations and educated assent in adult and pediatric patients. In some cases, 3D models can be a success for expanding patient compliance and decreasing patient anxiety. 22,23
The use of 3DP models leads to enhancement in the surgical team’s envisioning of the patient’s bony anatomy before surgery. Therefore, it has been shown that surgical times and anesthesia times are shortened, and blood loss is reduced. Even surgical strategies have been shown to improve with the use of these models. 24
Intraoperative pedicle screw templates
Complex and severe spinal deformities having more than 90° of Cobb angle may become tight for understanding the deformity, preoperative planning, and intraoperative success. This may also hold true for average deformities when placing pedicle screws. Pedicle screw insertion is one of the mainstays of spinal surgery fraught with devastating and life-threatening complicated injuries of inferior vena cava, descending aorta, spinal cord, lung, and so on. Nevertheless, it is the state-of-the-art technique at the moment because of its three-column bony purchase that provides enhanced stability. 10 However, insertion of these implants can sometimes become troublesome, particularly in the revision of complex deformity cases. 3DRP technology is an excellent facility to avert the risks of complications by helping surgeons in determining the pedicle entry points and accurate trajectories for pedicle screw insertion by manufacturing 3D-printed guides according to the preoperative CT images. Its effectiveness and safety are shown with a pilot study conducted on 11 adolescent idiopathic scoliosis patients. 3D-printed patient-specific guides enable preoperative planning and facilitate pedicle screw insertion intraoperatively. Likewise, it is found to be economical and accessible, since it does not need significant investment. 25 Especially deformities like congenital spinal malformations, infantile idiopathic scoliosis, neurofibromatosis, or neuromuscular scoliosis guarantee requisite to treat on time for averting the progress and even marked cosmetic disturbance, vital capacity, and potential neurological damage. 26,27 Luo et al. assessed the accuracy of pedicle screw insertion with 3DP guides on a series of 15 severe congenital scoliosis patients. They concluded that the pedicle screw insertion was more accurate by using 3DP guides when it was compared with freehand technique which led to their recommendation of this technique to the centers where intraoperative CT scan or O-arm navigation is not accessible. 28 In another study, Garg et al. also compared pedicle screw placement with jigs and freehand technique in complex deformities. Higher accuracy was found in the group, in which the pedicle screws were inserted with a 3DP jig. They deduced that an easier pedicle screw insertion to a deformed spine may prevent neglected deformity by the widespread application of surgical intervention on an earlier phase of the disease. 29
Moreover, the placement of pedicle screws with conventional methods may become very challenging and have some shortcomings even in the hands of most experienced surgeons or in straightforward cases. The vast majority of studies have reported rates of screw misplacement for the freehand technique usually as between 28% and 43% while only a few reported under 5%. 30,31 Therefore, improved accuracy and consistency in pedicle screws have led to investigations on the computer-navigated spine surgery. The computer-assisted pedicle screw installation has shown to be more accurate which decreases the risk of disturbing a nerve root, the spinal cord, or a vascular structure. 5 –8,16,10 Techniques described to facilitate a safer thoracic pedicle screw placement can be classified into four types: (1) freehand technique that relies on anatomical landmarks and averaged angular dimensions, (2) techniques with direct exposure of the pedicle such as through laminotomy, (3) CT-based computer-assisted surgery (CAS), and (4) fluoroscopy-based CAS technique. 32
As a tremendous invention, 3DP has been used for intraoperative guidance to accurate pedicle screw placement in miscellaneous ways, and investigations are ever increasing. Most of these techniques succeeded in some degree of accuracy. Mostly, the authors benefitted from the preoperatively printed models of the whole spinal column. To develop patient-specific pedicle screw templates, a 3DP model of the patient’s bone structures of the spinal column is first created from CT imaging or MRI information (Figure 1). The guide layout generally contains a segment that matches the posterior vertebral bone structures, such as spinous processes, lamina, facet joints, or transverse processes, and a part that outlines a drilling trajectory for screw instrumentation. When the guide is printed, the screw entry point and perfect screw direction are affirmed preoperatively (Figure 2), and then, the guide is sterilized. During the operation, the 3DP guide is put on the surface of target vertebra to successfully correct the pedicle screw direction (Figures 3 and 4).

A demonstrative case example. Anteroposterior standing plain radiograph of a 15-year-old adolescent idiopathic scoliosis.

Pedicle screw trajectory of the left pedicle of T3 is visible on three planes.
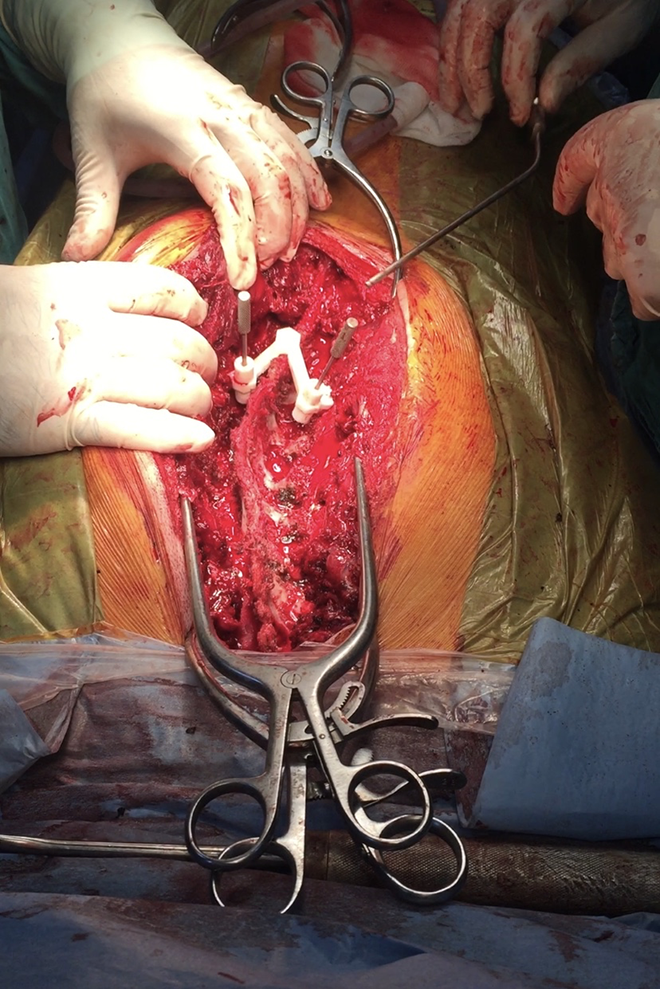
Intraoperative picture demonstrates the 3D printed guide usage.

(a) Postoperative anteroposterior standing plain radiograph of the same patient shown in Figure 1. (b) Computerized tomography evaluation of the T3 level demonstrates an accurate pedicle screw fixation.
The 3DP templates have been used at all vertebral levels, even for the S2AI screws. 33 At the cervical level, the pedicle screw instrumentation is of a highly delicate methodology because of the neural and vascular structures extremely susceptible to injury and their anatomical variations. In the study of Lu et al. 34 on cervical vertebrae, a total of 84 pedicle screws were inserted, and the accuracy of the screw position was affirmed by postoperative X-rays and CT examines, and no screw misplacement was observed. Therefore, a safer screw positioning was achieved with the cervical pedicle template technique. They concluded that the cervical pedicle template technique is easy to use and can simplify surgical action as well as producing a highly sensitive cervical pedicle screw insertion. Moreover, in their study, five abnormal or variant pedicles were encountered. The utilization of guide templates helped them pick the correct screws and choose the most ideal screw trajectory for every pedicle, effectively dealing with variations.
Sugawara et al. 35 showed that the operation time and radiation exposure was reduced, and high accuracy of the screw placement was achieved by using three steps of screw templates (the screw entry point location guide, drilling guides, and screw insertion guide) for C1–C2 posterior fixation. At the thoracic and lumbar levels, similar results of high exactness, insignificant cortical penetrations, optimized intraoperative time, reduced radiation and intraoperative bleeding, and usability have been accounted for.
The common shortcomings of these studies were being susceptible to the movement of every single vertebra on each superior and inferior adjacent segment. Some of the other printed models were designed to accommodate on a smooth surface like the lamina or body of a vertebra. Unfortunately, these guides were devoid of reference landmarks to fit properly on the vertebra to assign the pedicle screw trajectory and initial hole. Besides, the pedicle screw guide templates require a complete soft tissue resection of the posterior spinal bone landmarks such as the lamina, spinous process, facet joints, and sometimes, an excessive paraspinal muscle retraction can be required. 36,17 On the off chance that the soft tissue is not evacuated appropriately, it can increase the risk of screw misplacement. 37 There are some concerns that polymer-based templates produce debris during intraoperative use. Takemoto et al. 38 kept away from this issue by developing titanium patient-specific templates with a reduced contact area, but the expense of production was fivefold higher.
Although lateral mass and laminar screws are infrequently used, these templates have also been associated with higher screw insertion accuracy and the other better results (operation time, usability, cost, etc.). 39,40
Implantable devices (fusion cages and total disc replacement)
Many researchers are trying to imitate the stability and porosity of natural bone based on the question risen from the properties of an ideal fusion cage. The main problem here is that as the porosity increases, the osteoconductive effect of the implant decreases significantly. Existing metal anterior interbody cages and the other implantable devices may prompt subsidence and migration on account of the bungle in the biomechanical properties between the implant and the encompassing tissue. At this point, 3DP technology can produce implant devices that are both mechanically robust and structurally porous without impairing the osteoconductive effect of the implant. Young’s modulus of implants produced with 3DP technology is similar to Young’s modulus of the natural bone. Thus, the risk of collapse and stress shielding effect seen in traditional implants can be reduced. Appropriate porosity of the 3DP cage can increase the transmission of osteoinductive factors and facilitate osteoconduction, thereby potentially improving bone growth in the fusion site.
The most commonly used material to create 3D fusion cages is titanium; poly-ε-caprolactone, polyether ketone ketone (PEKK), and tantalum are the other products that can also be used. 41,42 When the structure of the cages formed using titanium was examined, it was observed that the Young’s modulus of the created structure falls between the normal cortical and the spongy bone. In a titanium cage optimization study published by Lin et al., 43 Young’s modulus values close to normal human bone values were achieved. It was determined that this situation has an architecture that allows 75% of the implant to be filled with osteoinductive graft material. In an ovine lumbar fusion study comparing three different fusion cages by McGilvray et al., 44 the 3DP interbody cages utilizing porous titanium material can provide more consistent bone ingrowth and biological fixation. Chung et al. presented an infection case who salvaged with 3DP patient-specific titanium implant that allowed two lumbar-level reconstruction. They found a good fusion and no implant-related complication at the end of a 3-year follow-up. 45 Numerous innovative 3DP cage forms for PLIF, TLIF, LIF, and ALIF procedures have been produced via powder-based printing and have become commercialized. 46
Besides its various advantages, RP has some drawbacks. First, it needs a high radiation exposure for 3D modeling of anatomical part of the patient, which is an issue that can be overcome using imaging techniques alternative to CT. However, this innovation is still less harmful than using intraoperative imaging techniques, since the operating staff are not exposed to the radiation. Second, the application of this newer technology is time-consuming and not suitable for urgent cases. The production process should be shortened for more extensive usage. 47 Third, RP needs equipped software and technical staff who knows how to use it. Emerging technologies such as machine learning and artificial intelligence may help to reduce technical assistance as well as provide a faster production process. 48
Conclusion
3DP is a promising improvement for a routine application in different stages of spine surgery such as preoperative planning, surgical simulations, patient–clinician communication, intraoperative guidance, and even implantable devices. Being an integral part of medicine, it increases patient safety, helps surgeons perform more complicated operations, and customizes implants for bone defects. While this efficient technological improvement is being adopted, implementing further studies is crucial to reach its highest potential and to find different aspects of spinal surgery to use it safely.
Footnotes
Acknowledgements
Authors would like to extend their gratitude to Karya Senkoylu for editing the article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical statement
The authors are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.