
Abstract
Background:
Metaphyseal sleeves have been used as metaphyseal filling implants to address bone loss during revision total knee replacements (TKRs). This study aims to compare the 2-year clinical and radiological outcomes of constraint implant with bone defect and constraint implant without or minimal bone defect in revisions TKR with preoperative coronal plane instability.
Materials and Methods:
Seventeen cases of constraint implants with metaphyseal sleeve matched paired with 34 cases of constrained condylar knee (CCK) prosthesis. Age, gender, body mass index and aetiology for revision surgery were recorded. Clinical outcome measures included Knee Society Knee Score (KSKS), Knee Society Function Score (KSFS), Oxford Knee Score (OKS), physical component summary (PCS) and mental component summary (MCS). Radiological outcome measures included joint line changes, hip–knee–ankle angle (HKA), coronal femoral angle (CFA) and coronal tibial angle (CTA).
Result:
Patients in sleeve group showed significant improvement in KSKS, KSFS and OKS (38 ± 7, 35 ± 6 and 20 ± 2 points, respectively, p < 0.001), while they were 19 ± 3 and 6 ± 2 points for PCS and MCS, respectively (p < 0.001 and p = 0.021). These postoperative scores after surgery were similar between the two groups at 6 months and 2 years. The sleeve provides comparable result in joint line restoration; the postoperative HKA, CFA and CTA were all comparable between the two groups.
Conclusion:
Metaphyseal sleeve with constraint implant is a viable option for revision TKR with preoperative coronal plane instability and significant bone defect. It is able to achieve similar clinical outcomes and joint line restoration compared to CCK prosthesis at 2-year follow-up.
Keywords
Introduction
Primary total knee arthroplasty (TKA) is a commonly performed orthopaedic procedure and usually results in good satisfactory outcomes. 1 As the number of this procedure is increasing, so does the revision rate of this procedure. Kurtz et al. projected that the number of revision total knee arthroplasty (rTKA) procedures performed per year is expected to rise from 38,300 in 2005 to 268,300 by the year 2030, which is approximately 600% increase. 2
One of the major challenges in rTKA is bone loss. The Anderson Orthopaedic Research Institute (AORI) is a widely adopted system to classify the bone loss during revision surgery and to provide guidance to the surgeon regarding the most suitable methods of reconstruction. 3,4 The type 1 defect is minor and usually can be managed with cement or morselized allograft. The type 2A defect involved metaphyseal bone loss in either one femoral or tibia bone loss and usually require metal augments to reconstruct the defect. The type 2B and type 3 are major metaphyseal bone defect, and the conventional strategies involve the use of bulk structural allograft 5 –8 impaction grafting techniques, 9,10 allograft-prosthetic composites 11,12 or tumour prostheses. 13
Metaphyseal cones and porous-coated metaphyseal sleeves are promising alternatives to address the bone loss in the revision surgery. Current literature have demonstrated that metaphyseal cones are a viable option in metaphyseal fixation with good short and midterm outcomes. 14 –20 However, Bohl et al. conducted a retrospective comparative study which showed metaphyseal cones were not associated with superior outcomes when compared to traditional technique at short-term follow-up. 21 Similarly, recent studies also demonstrated metaphyseal sleeve was able to produce promising result in short and midterm follow-up. 22 –29 However, most of the studies were case series and lack a control group. The purpose of our study is to compare the 2-year clinical and radiological outcomes of constraint implant with metaphyseal sleeve with the constrained condylar knee (CCK) prosthesis in revision total knee replacement (TKR) with preoperative knee coronal plane instability. We postulate that the clinical and radiological outcomes between both groups are comparable at 2-year follow-up.
Materials and method
After Institutional Board Review approval was obtained, we reviewed a prospectively collected database in a tertiary hospital knee arthroplasty registry. We identified 51 primary TKR cases with preoperative coronal plane instability which underwent revision surgeries between April 2012 and October 2014. Both groups of patients received constraint implants in view of the preoperative coronal plane instability. All cases have a minimum 2-year follow-up. Seventeen of the 51 cases required porous titanium metaphyseal sleeve in view of the significant bone defect. The bone defect was graded according to the AORI classification. The metaphyseal sleeve was used in cases with AORI 2a, 2b and 3 defects. The remaining 34 cases with minimal bone loss underwent revision surgery with CCK prosthesis. The study group (n = 17) was then matched to the control group (n = 34) in a 2:1 ratio. Both groups of patients were operated by the senior authors over a period from 2003 to 2014, each of whom had at least 3 years’ experience in these surgical procedures.
All patients were assessed by an independent allied health staff preoperatively, at 6 and 24 months postoperatively. The demographics of the patients, including age, sex and body mass index (BMI), were collected preoperatively. Clinical outcomes were measured through Oxford Knee Score (OKS), Knee Society Function Score (KSFS), Knee Society Knee Score (KSKS), physical component summary (PCS) score and mental component summary (MCS) score preoperatively and postoperatively.
The preoperative radiographs were reviewed to decide the femoral and tibial AORI classification. The radiological parameters assessed were the joint line change, hip–knee–ankle angle (HKA), coronal femoral component angle (CFA) and coronal tibia component angle (CTA) (Figure 1). The senior authors performed the radiographic analysis preoperatively and postoperatively.
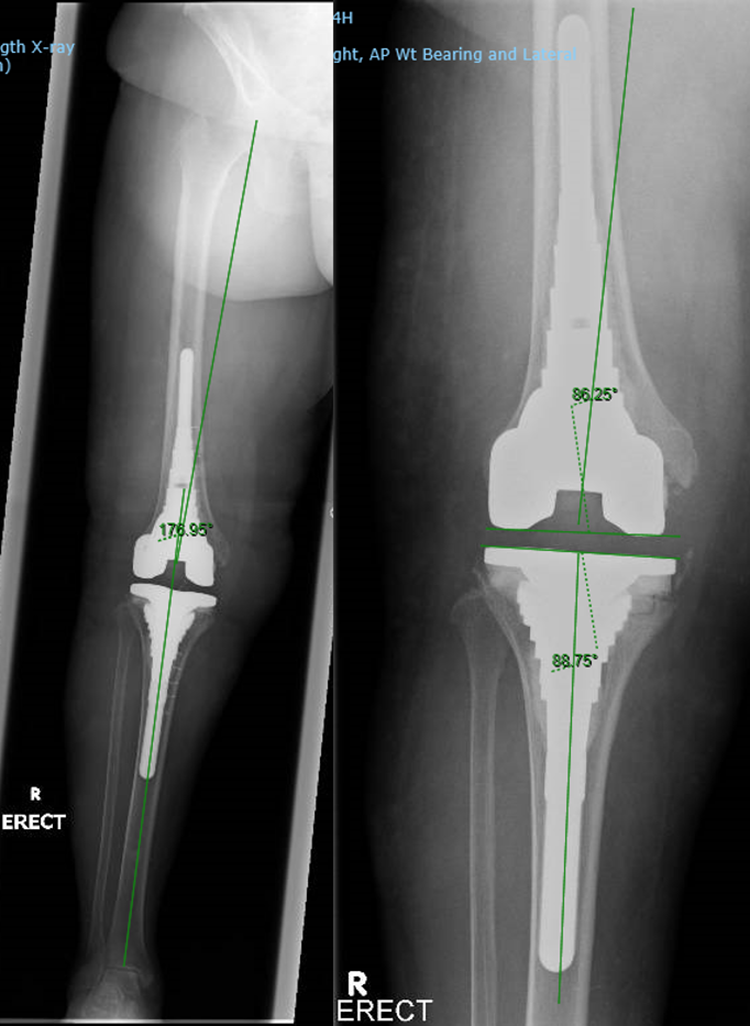
Radiological parameters: (a) HKA and (b) CFA and CTA. HKA: hip–knee–ankle angle; CFA: coronal femoral component angle; CTA: coronal tibia component angle.
Surgical technique for metaphyseal sleeve
All patients were placed under general anaesthesia and in supine position. The surgical approaches used were the standard medial parapatellar arthrotomy or a quadriceps snip depending on the surgeon preference. The bone defects were evaluated after the component removal (Figure 2). A high-speed burr was used to remove any retained cement or sclerotic bone before the sleeve preparation. The initial preparation involved sequential hand reaming of the tibia until adequate endosteal contact was achieved. The trial stem was attached with the metaphyseal broach for sequential broaching until axial and rotational stability was obtained. Subsequently, the broach handle removed, and the final broach used as an intramedullary cutting guide. The trial implants were assembled after the tibial tray sizing was completed. The final implant assembled and inserted into tibia with gentle impaction until the Morse taper is engaged and stable press fit is obtained in the tibia. A similar technique was used for the femoral side when a femoral sleeve was used. The Sigma TC3 Revision Knee Systems (DePuy, Warsaw, Indiana, USA) were implanted in all cases.

Intraoperative images showing metaphyseal defects.
Surgical technique for LCCK
The initial surgical steps are similar to the metaphyseal sleeve techniques. The bone defect was minimal and managed with cement filling. An extension stem was added with a constraint polyethylene insert. For the femoral side, the femoral cut was performed with the intramedullary alignment rod and adding a stem to the femoral component. The Legacy Constrained Condylar Knee (LCCK; Zimmer Inc., Warsaw, Indiana, USA) were implanted in all cases.
Statistical analysis
Power analysis was performed prior to the conduct of this study. The minimal clinically important difference (MCID) in OKS was found to be 5 points. 30 At 2 years after surgery, to detect a difference of 5 points in OKS from a baseline mean score of 23 with standard deviation of 6, a sample size of at least 14 patients in the sleeve group and 28 patients in the control group would be required to achieve a power of 0.80. This calculation was done for a one-sided test with a type I error of 0.05.
Statistical analysis was carried out in consultation with our in-house biostatistician, using SPSS® 21.0 (IBM, Armonk, New York, USA). Statistical significance was defined as a p value of ≤0.05. The Student’s unpaired t-test was used to compare the two groups for continuous variables including age, BMI, pre- and postoperative joint line, HKA, CFA, CTA, knee extension and flexion, KSFS, KSKS, OKS, PCS and MCS, while the Pearson χ 2 test was used for the analysis of categorical variables such as gender, side of operated knee, outliers for change in joint line and incidence of prosthetic joint infection.
Results
There was no significant difference in age, gender, BMI and side of operated knee between the two groups (Table 1). The incidences of postoperative prosthetic joint infection were 1 (5.9%) and 3 (8.8%) in the sleeve and control groups, respectively (p = 0.713).
Patients’ demographics and indications.

BMI = body mass index.
The pre- and postoperative joint line measured, change in joint line, pre- and postoperative HKA, CFA and CTA were all comparable between the two groups (Table 2). The change in the postoperative joint line was similar between both groups (p = 0.657).
Radiological outcomes.

HKA: hip–knee–ankle angle; CFA: coronal femoral component angle; CTA: coronal tibia component angle.
Patients in the sleeve group experienced significant improvement in functional outcome and quality of life scores at 2 years after surgery. These improvements were 38 ± 7, 35 ± 6 and 20 ± 2 points for KSFS, KSKS and OKS, respectively (all three p < 0.001), while they were 19 ± 3 and 6 ± 2 points for PCS and MCS, respectively (p < 0.001 and p = 0.021).
The preoperative OKS and PCS were 6 ± 2 and 7 ± 3 points poorer in the sleeve group compared to the control group. There was no significant difference in the preoperative knee extension and flexion, KSFS, KSKS and MCS between the two groups. Similarly, these functional outcome and quality of life scores at 6 months and 2 years after surgery were also comparable between the two groups (Table 3).
Functional outcome and quality of life scores.
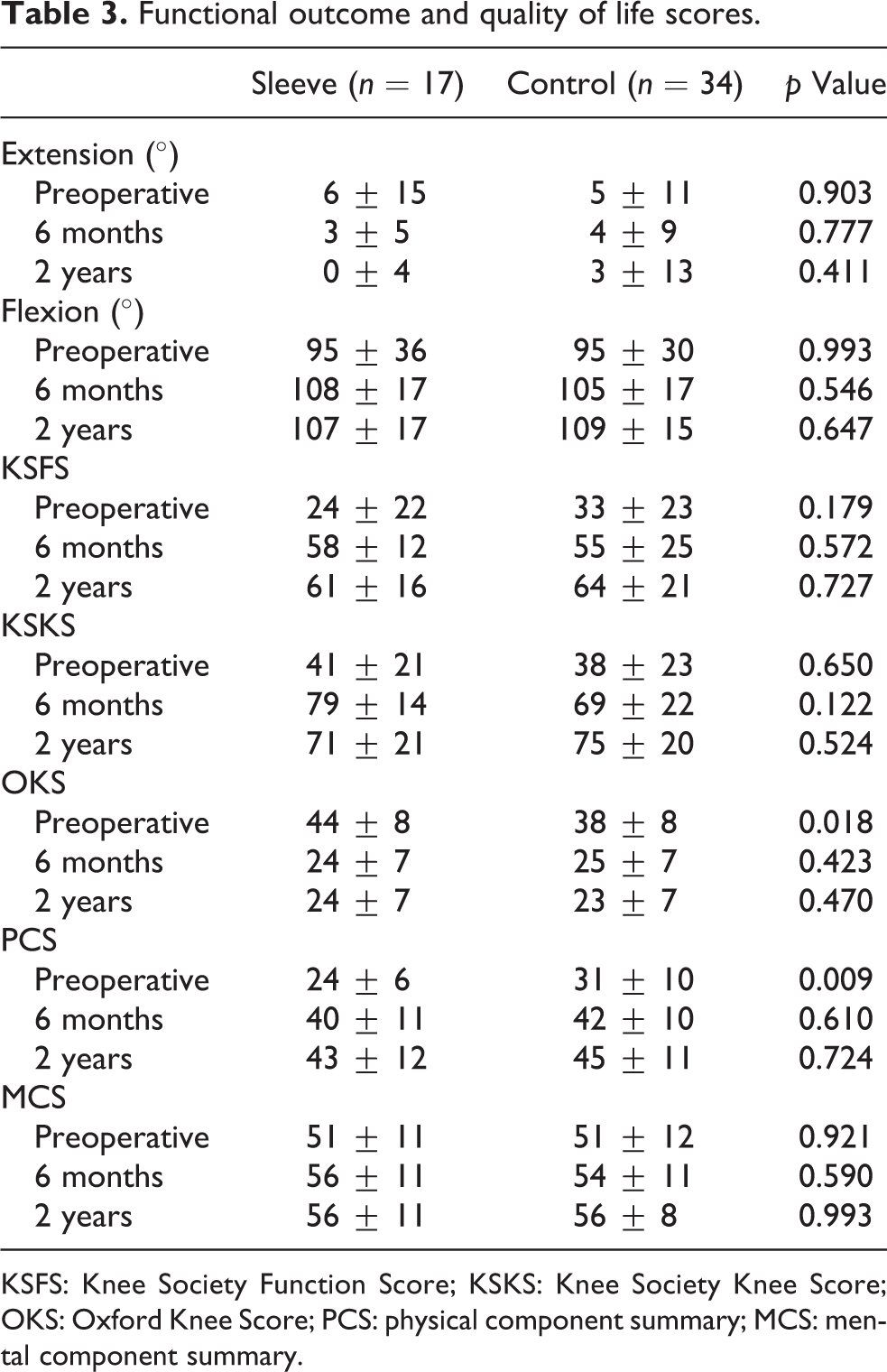
KSFS: Knee Society Function Score; KSKS: Knee Society Knee Score; OKS: Oxford Knee Score; PCS: physical component summary; MCS: mental component summary.
Discussion
This study has demonstrated two main findings. Firstly, the clinical outcomes of both groups were comparable at 2-year follow-up despite the sleeve group having poorer preoperative OKS and PCS scores. Second, the postoperative joint line changes between both groups are similar.
Femoral and tibia bone loss is frequently encountered in rTKA and effective defect management is crucial to obtain a stable fixation of components. The metaphyseal implants which include the metaphyseal sleeve or the metaphyseal cones have emerged as a popular alternative in rTKA with the aim to ensure reliable osseointegration and in turn a good reconstruction to prevent potential complications. There are several studies which evaluated the short and midterm clinical and radiological outcomes of the metaphyseal sleeves. 22 –29 However, most of the studies were mainly case series and lack a comparison group. To our knowledge, we believe this is the first study to compare 2-year clinical and radiological outcomes of constraint implant with metaphyseal sleeve with the CCK prosthesis in revision TKR with preoperative knee coronal plane instability.
Current literature have shown good results in the usage of metaphyseal sleeve in rTKA. 22 –29 Graichen et al. conducted a large prospective study which included 121 patients with 193 sleeves (119 tibial and 74 femoral) with a mean follow-up of 3.6 years. The study demonstrated average AKS was significantly improved from 88 ± 18 preoperatively to 147 ± 23 postoperatively (p < 0.01) and the functional knee score as a subsection of the AKS improved from 52 ± 18.9 preoperatively to 68.8 ± 23.3 points (p < 0.01) postoperatively. 26 Similarly, another large prospective study by Martin-Hernandez et al. which included 134 patients with a mean follow-up of 6 years also demonstrated satisfactory result. The authors reported average of knee KSS increased from 33 preoperatively to 78 postoperatively and functional KSS from 30 preoperatively to 80 postoperatively. All patients demonstrated optimal osseous integration at final follow-up. 29 Our study also demonstrated similar improvement in KSS and KSFS from 41 preoperatively to 71 postoperatively and 24 preoperatively to 61 postoperatively, respectively.
Our study showed both groups achieved improvement in postoperative joint line restoration and comparable results between both groups. A study by Pang et al. showed constrained implants lead to significant higher joint line shift in knee replacement surgery. 31 Joint line restoration in revision surgery is crucial as malposition can lead to patellar instability, patellar impingement, anterior knee pain and reduced range of motion. 32,33 We did not observe any radiolucent lines around the femoral or tibial metaphyseal sleeve or migration of the implants at the final follow-up. A large prospective study by Martin-Hernandez et al. reported optimal osseous integration in all patients and no implants migration, while Graichen et al. reported 96% of cases showed good osseointegration after 3.6-year follow-up. 26,29 Other short-term studies also demonstrated favourable radiological outcomes with stable implants at final follow-up. 22 –25,27,28
The end-of-stem pain is a complication which was described in patients who underwent rTKA with metaphyseal sleeve. A case series by Barrack, which consisted 66 femur and 50 tibia stems, found this complication in 11% of femoral and 14% of tibia stems. 34 Similarly, a study by Alexander et al., which consists of 30 rTKA, reported 23% of the cases complained of this complications and 10% still had chronic ‘end-of-stem pain’ at final follow-up. 24 However, we did not observe this complication in our sleeve group at 2-year follow-up. Intraoperative fracture is also a potential complication in rTKA, since it utilizes the broaching technique to prepare the metaphyseal. The reported incidence ranges from 2.3% to 6.5%. 35 –37 This complication was not observed in our study.
Our study is not without limitations. Firstly, this is a retrospective comparative study without randomization in selection of patients. Secondly, the follow-up of the study is short. Thus, future, larger randomized control trials are required to confirm the result of this study. The study may have been limited with small sample size, but power analysis was performed. Lastly, the power calculation of this study was only based on OKS MCID.
Conclusion
In conclusion, this study has demonstrated that constraint implant with metaphyseal sleeve is a viable option for revision TKR with preoperative coronal plane instability and significant bone defect. It is able to achieve similar clinical outcomes and joint line restoration compared to CCK prosthesis at 2-year follow-up.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by SingHealth NCSS (Nurturing Clinician Scientist Scheme) Award (13/FY2017/P1P/16-A30).