
Abstract
Background
The constrained condylar knee (CCK) implants are becoming more frequently used but the long-term outcomes are inadequately reported. A retrospective review of complex primary and revision total knee arthroplasty (TKA) with use of Legacy Constrained Condylar Knee prosthesis (LCCK; Zimmer) was performed to evaluate the functional and radiological outcomes, identify complications, and ascertain prosthesis survival.
Methods
A cohort of 54 primary TKA and 37 revision TKA cases were performed between December 2002 and March 2021 using the second-generation CCK prosthesis. The cases without using the constrained insert were excluded. Functional outcome comparison includes flexion and extension range of movement (ROM), Knee Society knee score (KSKS), function score (KSFS) and complications. Radiological outcome comparison includes tibiofemoral angle, hip-knee-ankle (HKA) angle and prosthesis components alignment. Survival analysis was performed using revision surgery for any reason as censoring criteria.
Results
The mean follow-up duration was 4.8 years (1.0–9.9 years) in primary TKA group and 6.2 years (1.0–18.6 years) in revision TKA group. The mean KSKS improved from 40.5 to 86.6 in primary TKA group and from 58.8 to 79.6 in revision TKA group. The mean KSFS improved from 41.8 to 58.9 in primary TKA group and from 34.1 to 58.2 in revision TKA group. The overall complication rate was 7.5% in primary TKA group and 35.1% in revision TKA group. Aseptic loosening was found in 6 cases and periprosthetic joint infection was found in 5 cases. Kaplan-Meier survivorship analysis estimated the overall mean survival was 17.9 years and 10-year survival rate was 93%.
Conclusions
Complex primary and revision TKA with use of LCCK prosthesis yielded significant reproducible improvement of clinical outcomes. The failure rate was low in primary TKA but relatively higher in revision cases.
Introduction
The important goals of total knee arthroplasty (TKA) are to achieve pain relief, restore joint stability, alignment, and function. A balanced tension within the knee throughout range of motion is essential to implant stability, which is dependent on articular morphology and surrounding soft tissues. In most cases, where both collateral ligaments are deemed competent, standard posterior-stabilised (PS) prosthesis is sufficient to achieve implant stability. However, in complex primary TKA and revision TKA cases, various soft tissue and bone stock deficiencies could result in ligamentous imbalance, predisposing to post-operative joint instability and prosthesis failure. In the 1970s, a valgus-varus constrained, unlinked condylar knee design was first developed to resist the coronal moments allowed by deficient soft tissue constraints. The implant design features a tall, broad central tibial post fitted tightly against a deep femoral box, with the advantage of limiting movement in coronal, antero-posterior and axial planes, providing increased stability. However, the increased constraint is associated with theoretical risk of premature aseptic loosening due to stress transmission to implant interface, increased polyethylene wear particularly at tibial post, and increased rotational stress.1,3
The first generation CCK implants feature limited modular options, and earlier studies reported conflicting outcomes. The first-generation designs were associated with higher rates of aseptic loosening and patellar complications. Lachiewicz et al. performed 44 primary TKA with either Total Condylar III (Johnson & Johnson) or Insall-Burstein II (Zimmer, Warsaw, IN, USA) prostheses with 10-year survivorship of 96% and 2 cases complicated by patellar osteonecrosis. 10 One study which recruited 57 revision TKA cases using first-generation CCK implants found 8-year survivorship of 75 ± 25% and 3 cases with patellar complications. 7 Another study reported only 50% of 21 cases had good outcome in knee score upon 4-year follow-up, with overall complication rate of 33%. 2
The second generation CCK prostheses improved with implant design and modularity. The NexGen® Legacy® Constrained Condylar Knee prosthesis (LCCK, Zimmer, Warsaw, IN, USA) included a right and left femoral component, and modular stem extensions for both femoral and tibial components. It allowed 2o of internal-external rotation and 1.25o of valgus-varus angulation. The design theoretically allowed soft tissue around the fixation interface to absorb force, reducing risk of aseptic loosening. The re-designed patellofemoral articulation was reported to decrease risk of patellar maltracking and complications. 6 Cholewinski et al. reported on long-term outcome of 43 primary LCCK with 11-year survival rate of 88.5%. Lachiewicz et al. reported no cases among the 27 primary TKA with LCCK required revision for loosening nor patellar problems upon mean follow-up of 5.4 years. 4 Regarding the long-term outcomes of LCCK in revision TKR, Kim et al. reported on 114 knees of revision cases over mean follow-up of 7.2 years and noted 9% complication rate with estimated 10-year survival rate of 96%. 1 Another study by Sanz-Ruiz et al. reported significant improvement of functional and radiological outcomes upon median follow-up of 8.2 years, while the overall complication rate was 23.4% and estimated 9-year survival rate of 80%. 5 The current literature showed diversified long-term outcomes, but most studies were limited by small cohorts, while studies including both primary and revision TKR cases were lacking.
We conducted a retrospective review on the mid- to long-term outcomes in primary and revision LCCK arthroplasty and to evaluate the functional outcomes, radiological results, complications, and survivorship. We hypothesize the LCCK prosthesis will show excellent functional and radiological outcomes with low complication and revision rate for knees undergoing complex primary and revision TKA.
Methods
Patient selection
Ethics approval was obtained from the Research Ethics Committee of our hospital. The data of primary and revision TKA cases performed in our hospital between December 2002 and March 2021 was searched and retrieved in the electronic patient record registry. Inclusion criteria included patients undergoing index arthroplasty with a complete set of NexGen® Legacy® Constrained Condylar Knee prosthesis (LCCK) implanted (including the stemmed CCK femur component stemmed tibia component with or without metal augments, and a CCK insert), with a minimum follow-up of one year, where patients were able to return for follow-up appointment. Exclusion criteria included patients with additional lower extremity joint replacement, cases without full-set LCCK prosthesis, cases using other brands of CCK prostheses, and self-reported neurological diseases.
Surgical technique
All the primary and revision knee arthroplasty cases were performed by the same group of arthroplasty surgeons of our department with standardised surgical technique. Tourniquet was used during the surgery and off for haemostasis after cement has set. Medial parapatellar approach was used for most of the cases except for severe valgus knee cases, in which the lateral parapatellar approach may be used. For revision cases, additional quadriceps snip was performed to improve the surgical exposure. For primary TKA, the use of LCCK prosthesis was decided intraoperatively if there was significant bone loss or satisfactory soft tissue balance could not be achieved with a posterior-stabilised (PS) prosthesis (Figure 1). For revision TKA, after implanting the LCCK femoral and tibial components, the use of a CCK insert was determined depending on the soft tissue balancing (Figure 2
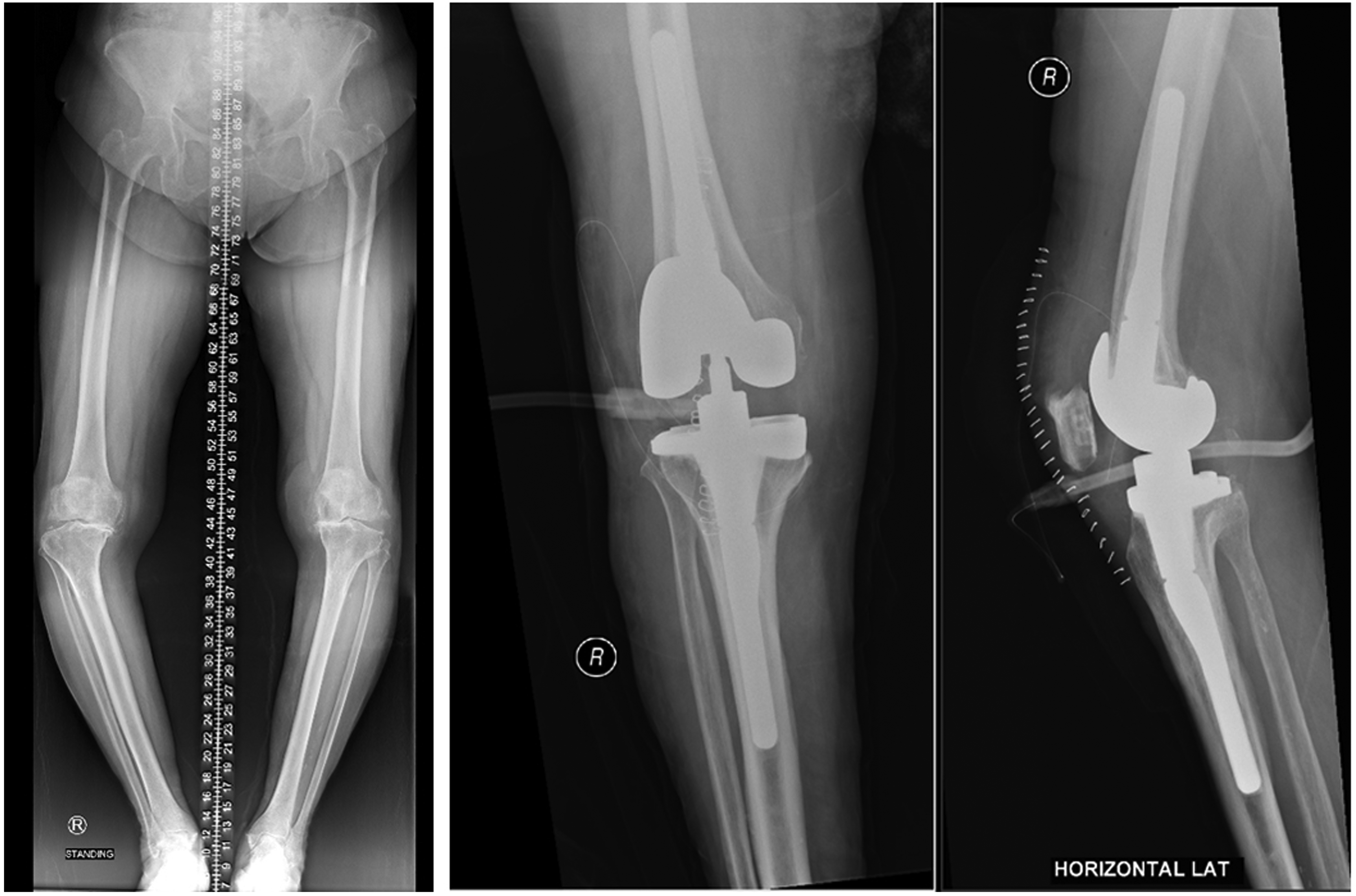
Pre-operative and post-operative radiographs of a primary TKA case. Full-set LCCK prosthesis was used due to severe varus laxity not balanced intra-operatively with standard PS prosthesis.

Radiographs of a revision TKA case. (a) Pre-operative standing anteroposterior radiograph of bilateral knees shows left primary TKA loosening with varus deformity. (b) Post-operative radiograph shows satisfactory left knee alignment with full-set LCCK prosthesis.
Follow-up assessments
Routine follow-up evaluation was performed post-operatively at 1-month, 3-month, 6-month and then yearly. During each follow-up, physical examination and radiographs were taken, and the review data were entered into the computerised record. The Knee Society Score was collected by an arthroplasty specialty nurse as part of routine assessment during follow-up. The patient records were kept at an electronic registry and independently reviewed by an orthopaedic surgeon not involved in the index operations. Clinical outcomes including flexion and extension range of movement (ROM), Knee Society Knee Score (KSS) and Function Score (KSFS). Presence of complications, revision and removal of implants were recorded. Standing anteroposterior whole lower limb radiographs with exposure from femoral head to ankle, also lateral view in 30-degree flexion were obtained for analysis was performed to evaluate limb alignment and implant stability. The latest Knee Society Radiographic Evaluation System and Methodology for Total Knee Arthroplasty was used for radiographic documentation of coronal and sagittal implant alignment, fixation interface integrity with respect to radiolucent lines and osteolysis, and a zonal classification system to document precise deficiency locations.
Statistical analysis
Statistical analyses were performed using SPSS software version 26.0 (IBM Corp, Armonk, NY, USA). Results were presented as point estimate of difference (95% confidence interval [95% CI]) and the associated p-value. A p-value of <0.05 was considered significant. The normality of all numeric data was tested with Shapiro-Wilk test. Patient demographic characteristics were summarised with descriptive statistics. Mean and standard deviation were used for nominal parametric variables. Comparison between pre-operative and post-operative data was performed with repeated-measures analysis of variance (ANOVA) for normally distributed data and repeated-measures Wilcoxon signed-rank test for non-parametric data. Complication rates of the two groups were compared using Chi-square test. Kaplan-Meier estimator was used for survival analysis, and log-rank test was used for between-group comparison of estimated survival.
Results
Between December 2002 and March 2021, 3864 primary TKA and 148 revision TKA procedures were performed at our unit. The initial cohort included 62 primary TKA cases (55 patients) and 52 revision TKA cases (48 patients). Five primary TKA patients and eight revision TKA patients deceased during the course of follow-up. Four cases were excluded as the follow-up period was less than one year. 18 cases were excluded due to incomplete utilisation of the whole LCCK prosthesis. The final cohort included 54 primary TKA cases and 37 revision TKA cases. The basic demographic data are summarised in Table 1. The primary TKA cohort consisted of 15 males (27.8%) and 39 females (72.2%), with mean age of 68 years (range 41–82 years). The revision TKA cohort consisted of 19 males (51.4%) and 18 females (48.6%), with mean age of 71 years at operation (range 56–94 years). The mean body mass index (BMI) was 26.4 kg/m2 in primary group and 27.9 kg/m2 in revision group respectively. Comorbidities include hypertension, diabetes mellitus, obesity, gout, ischaemic heart disease, stroke, spinal stenosis, and polio.
Demographic data in primary and revision TKA groups.
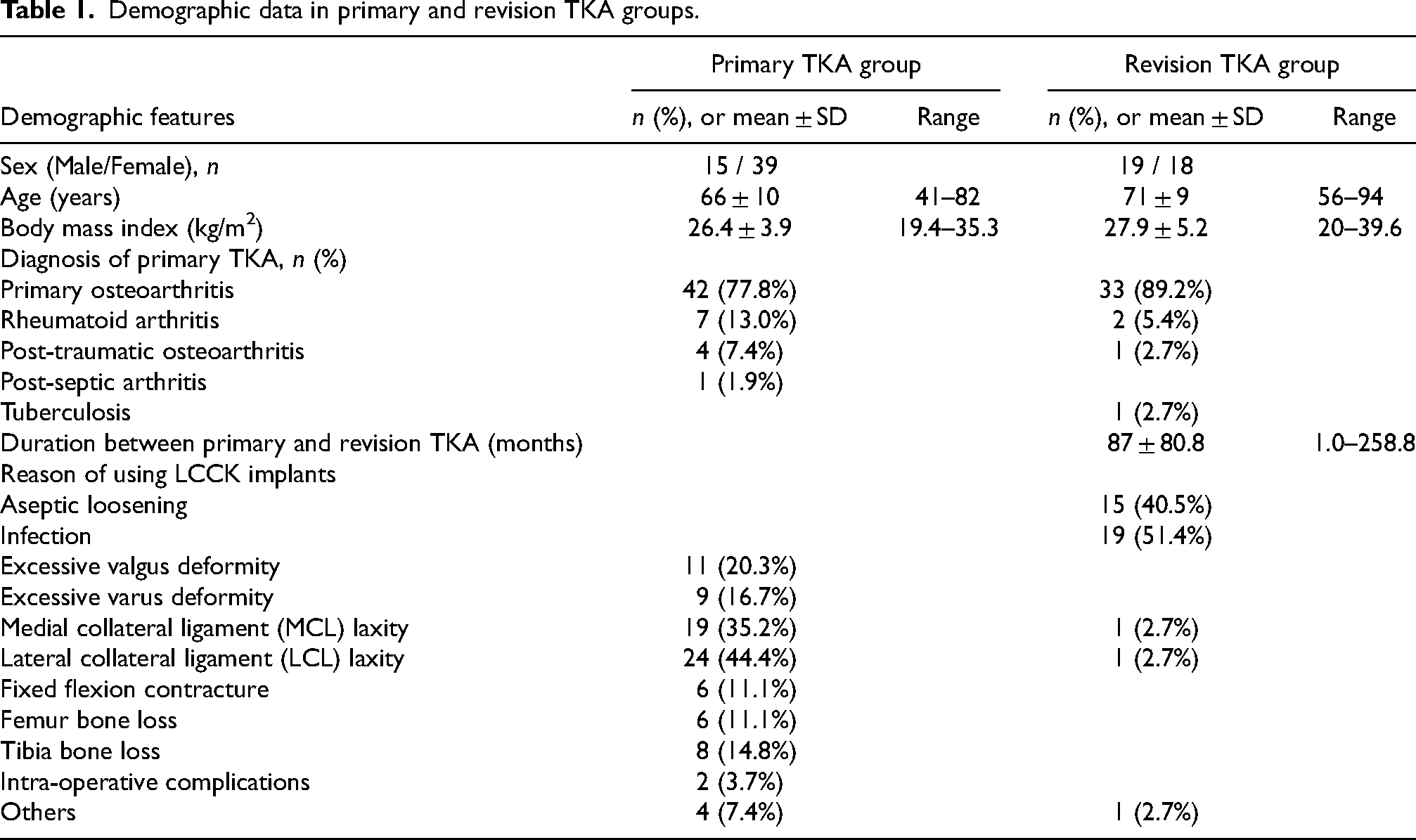
Among the primary TKA cases, the decision of using the LCCK prosthesis was excessive valgus or varus deformity in 20 cases. In 33 cases there were inability to achieve ligament balancing, while the remaining cases were due to knee fixed flexion contracture, excessive bone loss and intra-op complications respectively. The diagnosis was primary osteoarthritis in 42 cases (77.8%), rheumatic arthritis in 7 cases (13%), post-traumatic osteoarthritis in 4 cases (7.4%) and prior septic arthritis in 1 case (1.9%) respectively.
Among the revision TKA cases, the diagnosis of previous knee arthroplasty was primary osteoarthritis in 33 cases (89.2%), rheumatoid arthritis in 2 cases (5.4%), post-traumatic osteoarthritis and tuberculosis in one case, respectively. The mean duration between primary and revision TKR was 87.0 months (range 1.0–258.8 months). The indication for revision TKR was infective loosening in 19 cases (51.4%) and aseptic loosening in 15 cases (40.5%). The indication of remaining cases includes post-operative medial collateral ligament laxity, lateral laxity, and broken implant. Among the cases of infective loosening, the most common microorganisms were methicillin-resistant coagulase-negative staphylococci (MRCNS) in 6 cases (31.6%) and group G streptococcus in 4 cases (21.1%), while 4 cases (21.1%) had negative culture.
Clinical outcomes
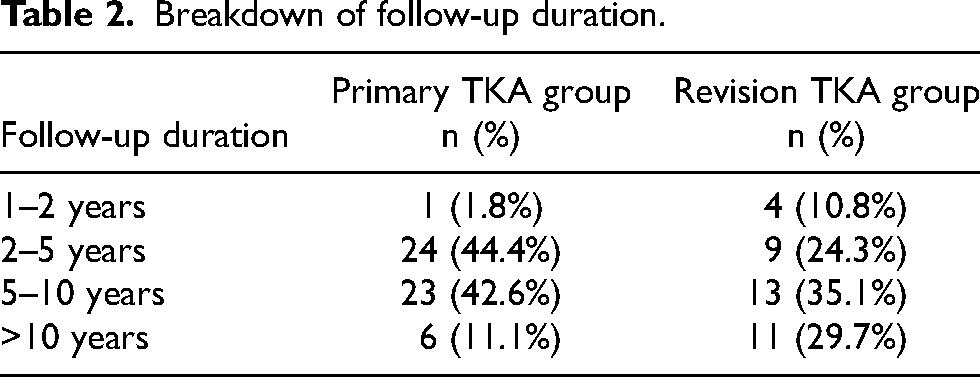
The primary TKA group had mean follow-up 4.8 years (1.0–9.9 years), and the revision TKA group had mean follow-up of 6.2 years (1.0–18.6 years). The breakdown of the follow-up period for both groups was shown in Table 2. The average preoperative and postoperative flexion and extension ROM, knee score, and functional score according to the Knee Society system were shown in Table 3. The use of LCCK prosthesis showed statistically significant improvement in clinical outcomes of the primary TKA cohort. The mean knee flexion ROM improved from 96.5° (95% CI, 89.3° – 103.8°) to 104.9° (101.1° – 108.7°) while mean extension ROM improved from 12.1° (7.6° – 16.5°) to 3.2° (0.1° – 6.3°). The mean Knee Society Knee Score (KSS) improved from 40.5 (95% CI, 34.3–46.7) to 86.6 (82.2–91.0) and mean Knee Society Function Score (KSFS) improved from 41.8 (34.0–49.6) to 58.9 (51.0–66.7). For the revision TKA cohort, the mean knee flexion ROM improved from 92.4° (85.1° – 99.7°) to 99.4° (93.6° – 105.2°). There was no statistical difference of mean pre-operative and post-operative knee extension ROM (p = 0.572). Nonetheless, there were significant improvement of mean KSS from 58.8 (47.6–70.0) to 79.6 (72.2–87.0) and mean KSFS from 34.1 (20.5–47.8) to 58.2 (39.4–77.1) respectively.
Breakdown of follow-up duration.
Clinical outcome comparison at the final follow-up.
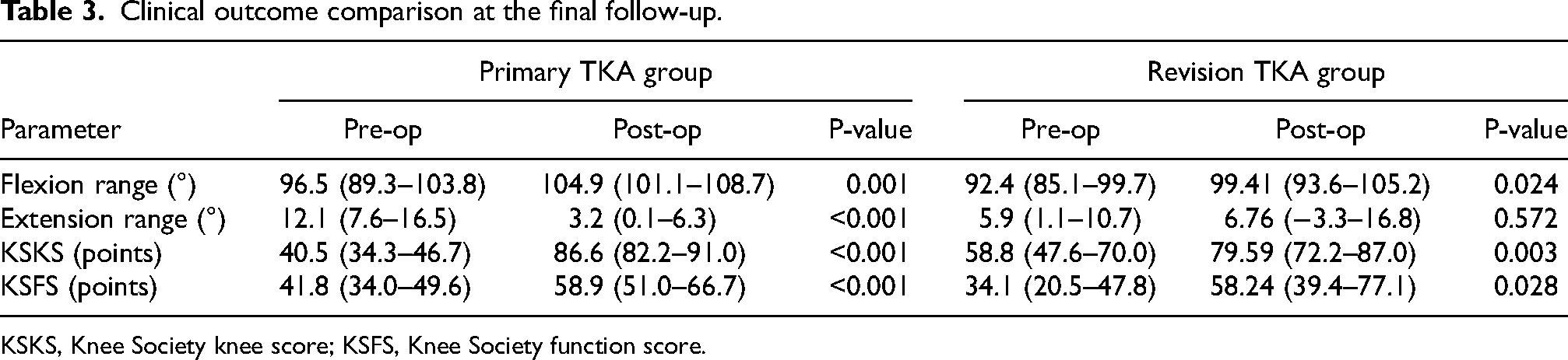
KSKS, Knee Society knee score; KSFS, Knee Society function score.
Radiological outcomes
Radiolucent lines (RLLs) defined as more than 1 mm at the bone-cement interface were seen in 10 primary TKA cases (18.6%) and 5 revision TKA cases (13.5%). At the femoral implant, radiolucent lines were observed at anterior flange and femoral distal fixation region. At the tibial implant, radiolucent lines were seen at medial baseplate, lateral baseplate, and stem extension. None of the RLLs were found progressive upon interval imaging.
For primary TKA cases, the mean preoperative tibiofemoral angle and hip-knee-ankle (HKA) angle were 3.2° varus (range, 38° valgus - 39° varus) and 7.9° varus (range, 34° valgus - 52° varus) respectively. The mean postoperative tibiofemoral angle was improved at 4.7° valgus (range, 10° valgus - 4° varus) and the mean post-operative HKA angle was 0.1° valgus (range, 6° valgus - 20° varus). For revision TKA cases, the mean preoperative tibiofemoral angle and hip-knee-ankle (HKA) angle were 0.2° varus (range, 21° valgus – 32° varus) and 6.7° varus (range, 10° valgus - 34° varus) respectively. The mean postoperative tibiofemoral angle was improved at 5.4° valgus (range, 13° valgus - 1° varus) and the mean postoperative HKA angle was 0.4° valgus (range, 9° valgus - 9° varus). The coronal and sagittal alignment of both femoral and tibial components were evaluated according to the latest Knee Society Radiographic Evaluation System. 13 The coronal alignment of the femoral component is comprised of the distal femoral component surface with respect to the anatomic axis of the femoral shaft. Similarly, the tibial component alignment is determined by the angle between the baseplate and the mechanical axis of the tibia. The sagittal alignment is evaluated on the lateral radiograph. Femoral component alignment is measured as the angle between the most distal femoral fixation surface with respect to the femoral shaft axis. Tibial component alignment is denoted by the posterior slope (Figure 3). The radiological measurements upon the latest follow-up were shown in Table 4 and Table 5.
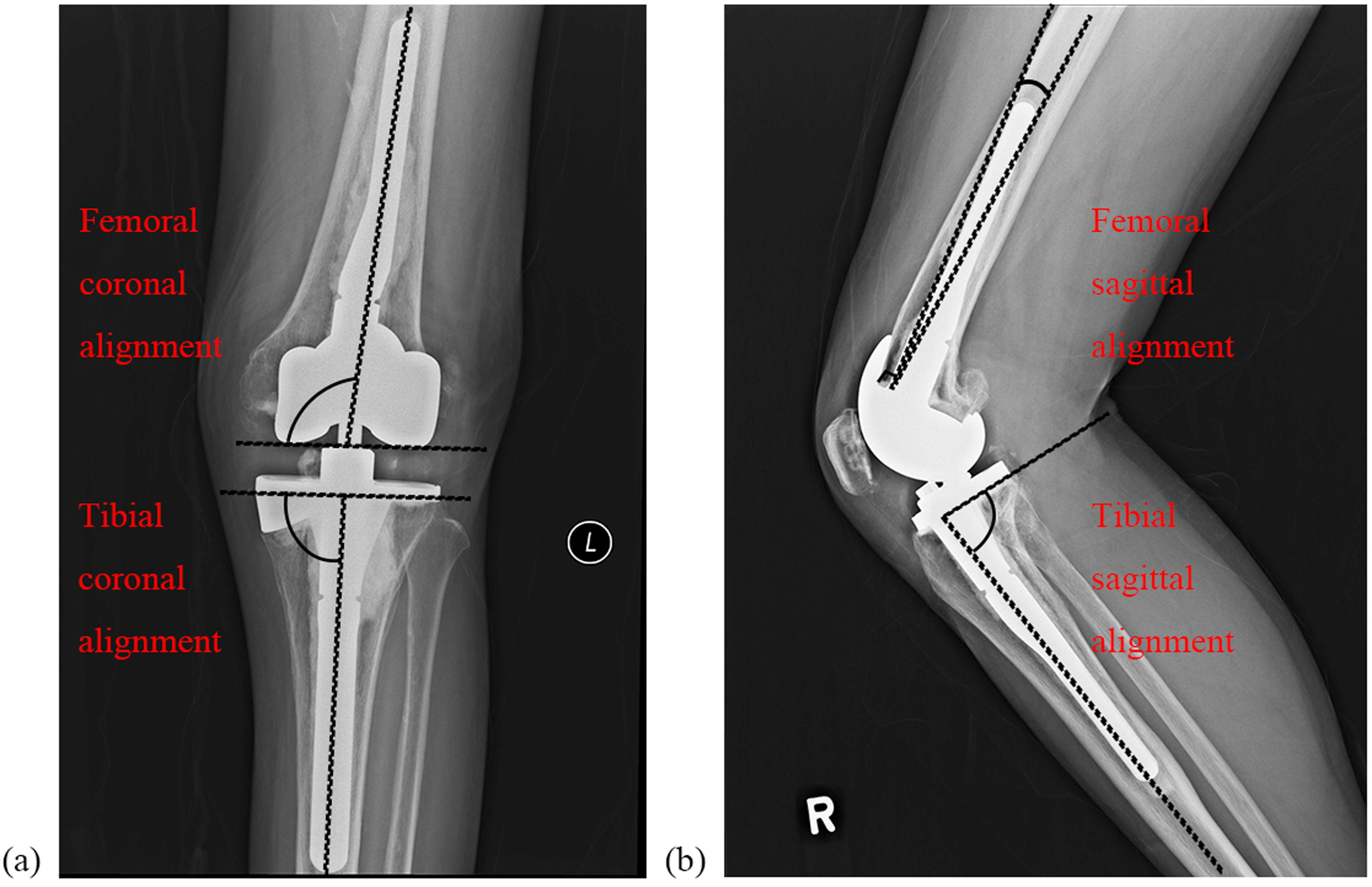
(a) anteroposterior and (b) lateral right knee radiographs denoting measurement of the femoral and tibial component alignment in the coronal plane and sagittal plane respectively.
Primary TKA group radiological outcome comparison at the final follow-up.
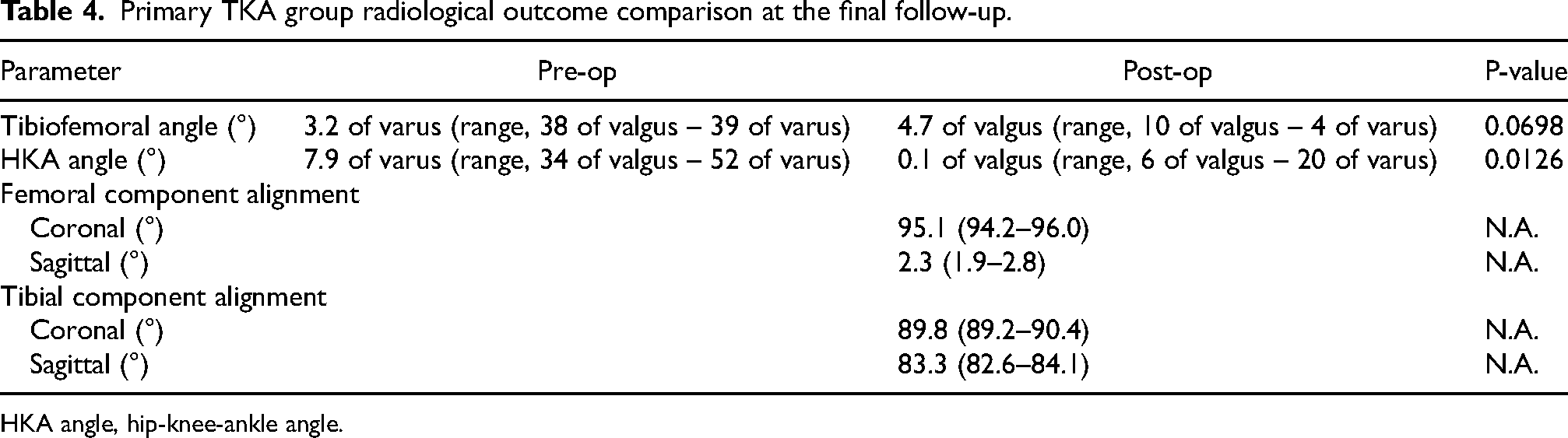
HKA angle, hip-knee-ankle angle.
Revision TKA group radiological outcome comparison at the final follow-up.
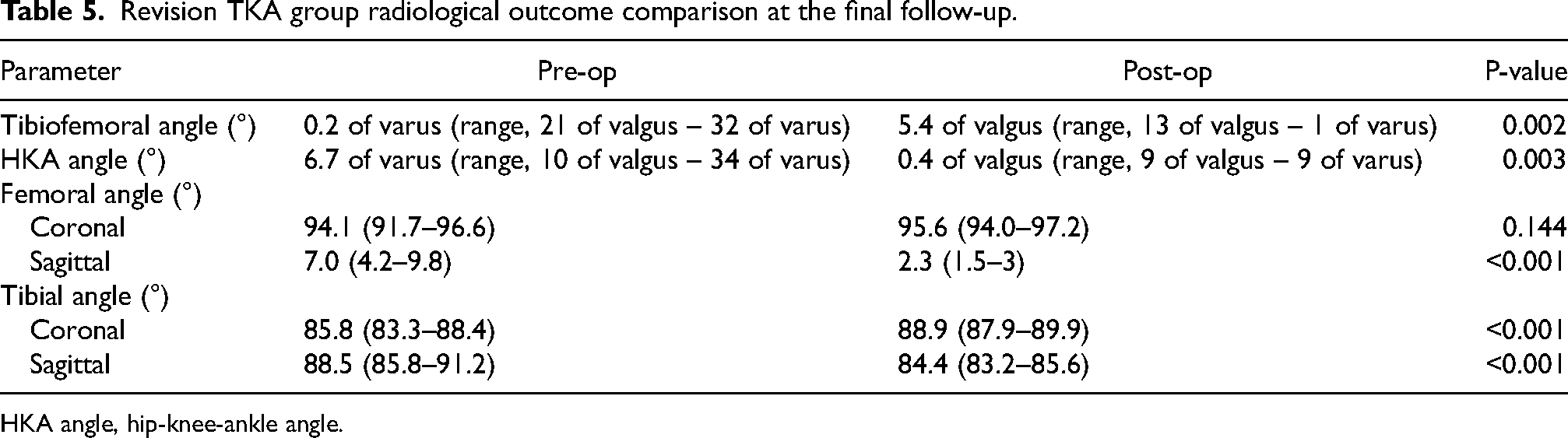
HKA angle, hip-knee-ankle angle.
Complications
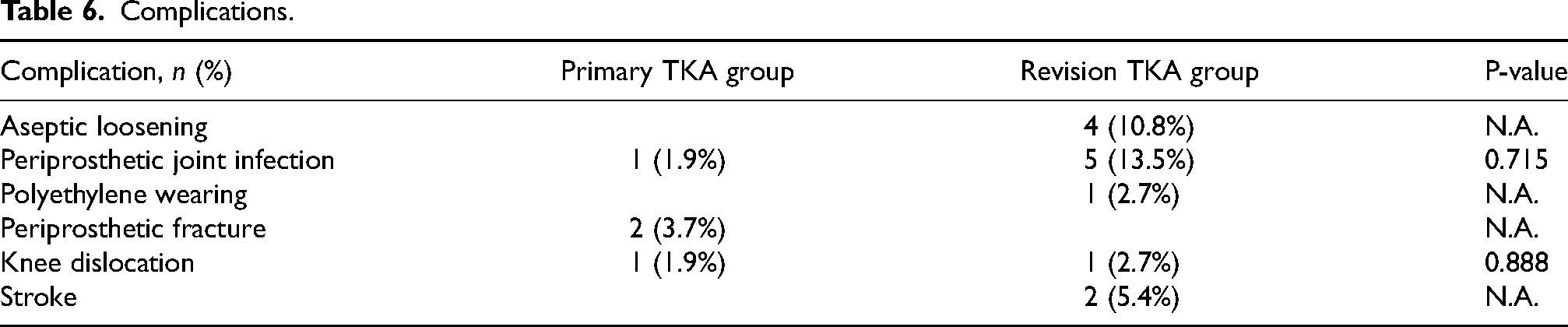
The overall complication rate in primary TKA group was 7.5%. One case was found to have lateral femoral condyle fracture intra-operatively and underwent open reduction internal fixation with plate. One case was found to have medial supracondylar femur stress fracture at 11 months post-operation and was treated conservatively. A case with underlying rheumatoid arthritis and severe pre-operative fixed flexion contracture of 30° was found to have anterior knee dislocation at 2 weeks post-operatively, requiring emergency open reduction. One case was complicated with acute periprosthetic joint infection at 1 month post-operatively with exchange of insert performed, and the patient was given life-long antibiotics suppression.
The overall complication rate in revision TKA group was 35.1%. Aseptic loosening was found in 4 cases (10.8%), with the time of diagnosis ranging from 3.4 to 11.3 years post-operation. Two cases underwent another revision TKR, whereas the other two cases were treated conservatively. Periprosthetic joint infection was found in 5 cases (13.5%), and all cases were initially revised due to previously infected implants. The infection occurred at post-operative intervals ranging from 3 months to 2.2 years.All infection cases were given long-term antibiotics and two-staged revision operation was performed in three of the cases. Among three cases with positive cultures, the isolates were Streptococcus mitis, Streptococcus agalactiae and Group G Streptococcus respectively. The list of complications was summarised in Table 6.
Complications.
Survival analysis
Kaplan-Meier survivorship analysis was performed using revision for any reason as censoring criteria (Figure 4). The mean survival in primary TKA group, revision TKA group and overall group are 12.3 ± 0.21 years, 17.7 ± 0.98 years, and 17.9 ± 0.74 years, respectively. The estimated 10-year survival rate of primary TKA group, revision TKA group and overall survival are 98%, 91%, and 93% respectively. Analysis revealed no statistically significant difference between survivorship of primary and revision TKA groups.
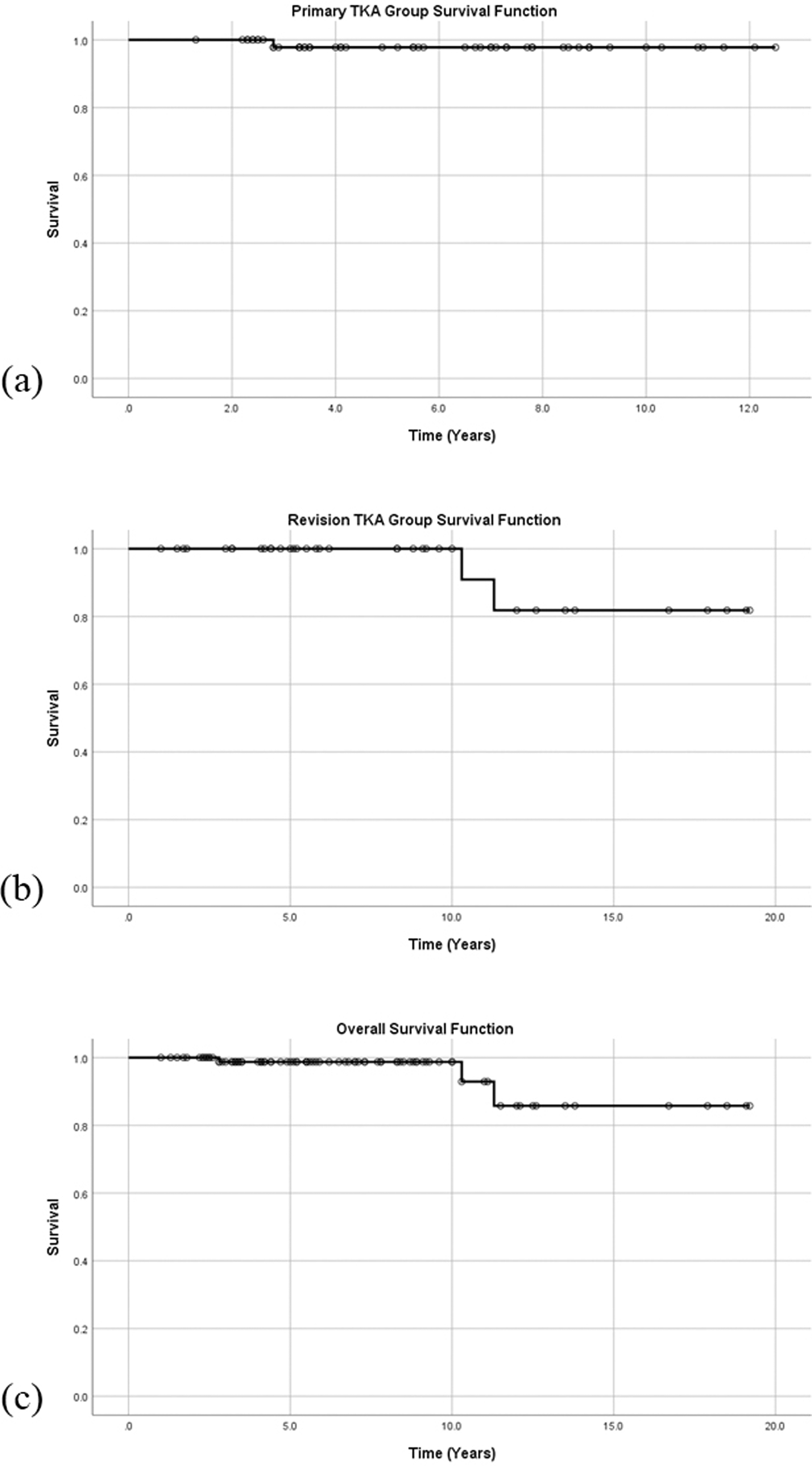
Kaplan-Meier curve of (a) primary, (b) revision and (c) overall survival rate.
Discussion
During the procedure of TKA, surgeons generally prefer using the prosthesis with the least level of constraint, as increased constraint may increase stress to the prosthesis-cement or cement-bone interfaces, causing mechanical loosening and early implant failure. In most scenarios, it is unusual to require the use of prosthesis with more constraint than posterior stabilized (PS) design. However, in certain primary and revision cases, the PS prostheses are inadequate to achieve optimal stability. For primary TKA, the examples include patients with excessive collateral ligament laxity, extreme valgus or varus deformity. In revision TKA, the common instances include excessive bone defect and soft tissue incompetence.7,10 The exact amount of instability necessitating increased constraint is still debatable, where a study suggested a persistent laxity of greater than 7–10 mm despite soft tissue balancing should require a CCK implant. 9
The most significant finding of this study is to confirm the working hypothesis that patients undergoing complex primary and revision TKA with the LCCK implant will show favourable functional and radiological outcomes, with low revision rate and acceptable complication rate. Our study over a mean follow-up of 4.8 years for primary TKA and 6.2 years for revision TKA cases showed the majority of cases had significant improvement of knee ROM, alignment and functional outcome. These results are comparable to those in current literature of complex primary and revision TKA.1,4,6,7,9–11
Radiolucent lines were found in 9.3% of primary TKA and 13.5% of revision TKA cases. Most of them are distributed over medial and lateral baseplates of tibial component on antero-posterior view (Zone 1 and 2), also anterior flange and central box region of femoral component (Zone 1 and 3) according to the Knee Society Radiographic Evaluation System. 13 All of the radiolucent lines are less than 1 mm in height and are non-progressive. The incidence of radiolucent lines is similar to previous literatures, which ranges from 4% to 31%.1,11 Some studies suggest the incidence of radiolucent lines is higher in revision than primary TKA, and more common around the tibial component. Nevertheless, adequate cement fixation was more readily reproducible at the tibial component than the femoral component, as the easier access to the tibial metaphysis allowed better cement interdigitation into the exposed cancellous bone. 1
Kim et al. reported an overall 9% complication rate among a cohort of 114 revision TKA cases over a mean follow-up of 7.2 years, with aseptic loosening being the most common cause of failure. Of the four aseptic loosening cases, three received re-revision surgery with LCCK prosthesis. Pyogenic infection recurred in two cases with subsequent two-stage revision operations performed. 1 Another study on revision TKA by Nakano et al. showed a complication of 7.3%, where all the cases were recurrent pyogenic infection with no cases of aseptic loosening. 6 For primary TKA cases, Maynard et al. reported an overall complication of 19.7% among 127 cases over a minimum follow-up of 7 years, while the results of the 26-case cohort by Lachiewicz et al. showed no cases of aseptic loosening and only one case with pyogenic infection in an immunocompromised patient.4,9 In the current study, there is only a single case of periprosthetic joint infection in the primary TKA group, and the complication rate is similar with those reported in literature. A higher complication rate of revision TKA group than previous studies is observed. We believe the major factor lies in the baseline patient demographics. Compared with similar studies reporting on outcomes of revision TKA using LCCK prosthesis, our case cohort includes patients with more advanced age, higher baseline body mass index, and more medical comorbidities. The most common indication for revision in our cohort is infective loosening, in contrary to most other studies where aseptic loosening is the main reason for revision.1,2,6,8 This observation is in line with the results described by Vince and Long, where a high rate of loosening is observed after revision TKA and most failure cases had a history of infection. 14
Multiple techniques and implant designs have been developed in attempt to optimise implant positioning and restoration of native knee biomechanics. The LCCK prosthesis has the highest level of constraint among the second-generation unhinged constrained condylar implants. Its insert limits the internal-external rotation of ±2o and of valgus-varus angulation of ±1.25o. In contrast, other second-generation CCK implants have different designs in terms of degree of constraint. The Triathlon Revision system (Stryker, Mahwah, NJ, USA) insert gives ±2o of varus/valgus constraint, while allowing for ±7o of internal/external rotation. 12 The Attune Revision system (DePuy, Warsaw, Indiana, USA) is designed to provide ±1.25° varus/valgus constraint while allowing ±4° of internal/external rotational freedom during the full range of motion. 15 However, whether the difference in the level of constraint among the second-generation CCK implants would significantly affect the clinical outcomes remains uncertain. To our best knowledge, there are currently no head-to-head trials comparing the functional outcomes following complex primary and revision TKA with CCK implant of various constraints.
There are several limitations to this study. This is a retrospective study with no suitable control group for outcome comparison. The mean follow-up period is relatively short due to the inclusion of more recent cases into the study. Nevertheless, the inclusion of cases over a long time frame up to 18.6 years of follow-up provided representative data on long-term outcome. In order to standardize the prosthesis for our study, we excluded cases where the full set of LCCK prosthesis was not utilized or another brand of CCK prosthesis was used, thus reducing the number of caseloads. To our best knowledge, the current study includes the largest local case cohort utilising a complete LCCK prosthesis in both complex primary and revision TKA cases, which should provide a contemporary and comprehensive overview of its outcomes in future indicated cases.
Conclusion
The LCCK is a second-generation modular CCK prosthesis which produces promising clinical and radiological outcomes in complex primary and revision TKA. The major complications include periprosthetic joint infection, followed by aseptic loosening. The estimated overall mean survival is 17.9 years, and 10-year survival rate is 93%. Further investigations of longer follow-up intervals and larger cohort may be needed to validate the long-term outcomes.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.