
Abstract
Background:
We evaluated the accuracy of a sagittal alignment of tibial component in total knee arthroplasty (TKA) with the sagittal reference line using the preoperative radiograph.
Methods:
We evaluated 151 patients who underwent primary TKA with posterior cruciate substituting type implant. For 75 patients, the sagittal reference line using preoperative radiograph (group A) was used, while for 76 patients the sagittal reference using intraoperative fibular shaft line (group B) was used. The parallel line (line S) to the anatomical axis of the tibia in the lateral plain radiograph was used as the sagittal reference. The distance from line S to proximal tibia cutting area and to skin surface 20 cm distal to the cutting area was measured in preoperative radiographs. Next, the distance to the extramedullary guide rod was applied intraoperatively, reflecting the results. The intraoperative fibular shaft line was determined using the connecting line between the tip of fibular head and the lateral malleolus. The postoperative tibial component slope angle and the difference to the target slope angle were compared.
Results:
The difference to the target angle was 1.8 ± 1.3° in group A, whereas the difference was 2.5 ± 1.4° in group B (p = 0.04). The patients with difference within 3° to the target angle were 78.7% in group A and 61.8% in group B (p = 0.024).
Conclusion:
The sagittal reference line using the preoperative lateral radiograph was helpful as a reference guide for the tibial slope in TKA.
Introduction
Sagittal tibial alignment is one of the important factors for successful total knee arthroplasty (TKA), including stability and survival rate. 1 –3 However, no definite landmarks for sagittal slope exist and it has not been studied thoroughly.
Several anatomical landmarks of the tibia in TKA were introduced and used in operations, including anatomical axis of the proximal and central tibia, anterior and posterior cortical line, and fibular shaft axis. 4 –8 These references had differences between each other and should be considered for the sagittal alignment for the results of TKA. Among these, the fibular shaft axis could be used easily due to the palpable fibula in the proximal and distal areas intraoperatively. Although this reference is well-known and widely applied, its accuracy is not high. 9
The line connecting the most anterior point of the predicted tibial cut surface and the skin surface 20 cm distal to the predicted cut surface using computed tomography (CT) scan was studied and reported as a useful guide for the tibial slope for TKA. 9
We applied this reference in lateral plain radiographs and hypothesized that this reference would be a simple and accurate method. The purpose of this study is to evaluate the accuracy of a sagittal reference of tibial component in TKA using proximal tibial cutting surface and anterior skin surface in lateral plain radiograph.
Materials and methods
Patients
A total of 151 patients who underwent primary TKA from September 2017 to August 2018 were evaluated. Patients were divided into two groups: 75 patients who underwent TKA from April 2018 to August 2018 using the reference with tibial cut surface and anterior tibial skin were designated as group A, and 76 patients from 91 patients who underwent TKA from September 2017 to March 2018 using the fibular shaft axis were selected (case matched in age and sex) and designated as group B.
The demographics, including age, sex, the direction of the leg, height, body weight, and body mass index (BMI), did not show statistically significant differences between the two groups (Table 1).
Demographic characteristics of the two groups.
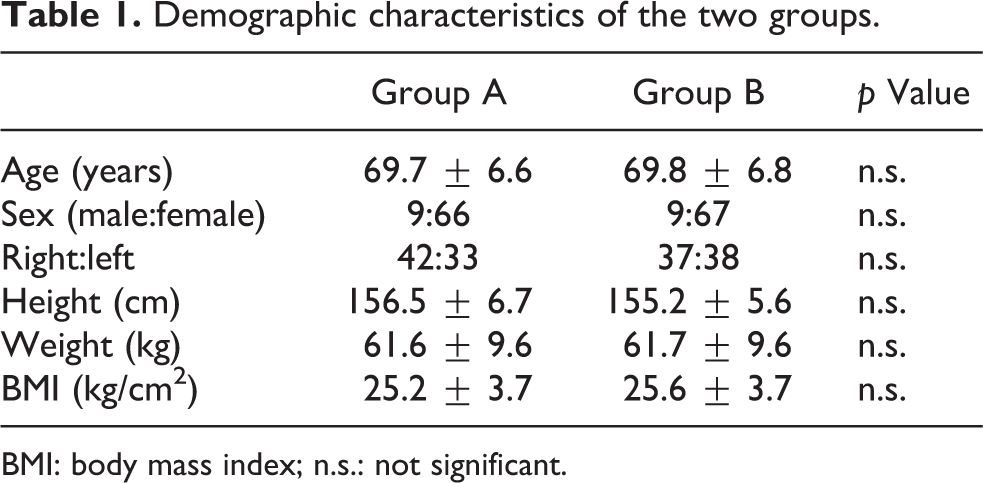
BMI: body mass index; n.s.: not significant.
Surgical procedure
In group A, the preoperative planning was first performed using the lateral radiograph of the tibia. First, the anatomical axis line, which is a line bisecting the medullary canal at 7 cm distal from the plateau and at 7 cm proximal from the plafond, was drawn. This axis was used as the reference because it is the closest axis to the mechanical axis in coronal and sagittal planes. 10 Next, the anatomical axis line was moved parallel to the anterior area of the tibia (line S). Each distance from the tibial cut surface and anterior skin surface 20 cm distal to the tibial cut surface to the line S was measured. The difference in distance between the proximal area and the distal area was measured (Figure 1).

(a) In the lateral radiograph of tibia, the anatomical axis line, which is a line bisecting the medullary canal at 7 cm distal from plateau and at 7 cm proximal from the plafond, was drawn. (b) The anatomical axis line was moved parallel to the anterior area of the tibia (line S). (c) The distance from line S to the tibial cut surface (a) and anterior skin surface 20 cm distal to the tibial cut surface (b) were measured.
During TKA operation, this distance in difference was applied. Using the extramedullary tibial cutting guide, the distance from the tibial cutting surface and anterior skin surface 20 cm under the tibial cutting surface was measured (Figure 2). The cutting slope followed the reference of each implant.
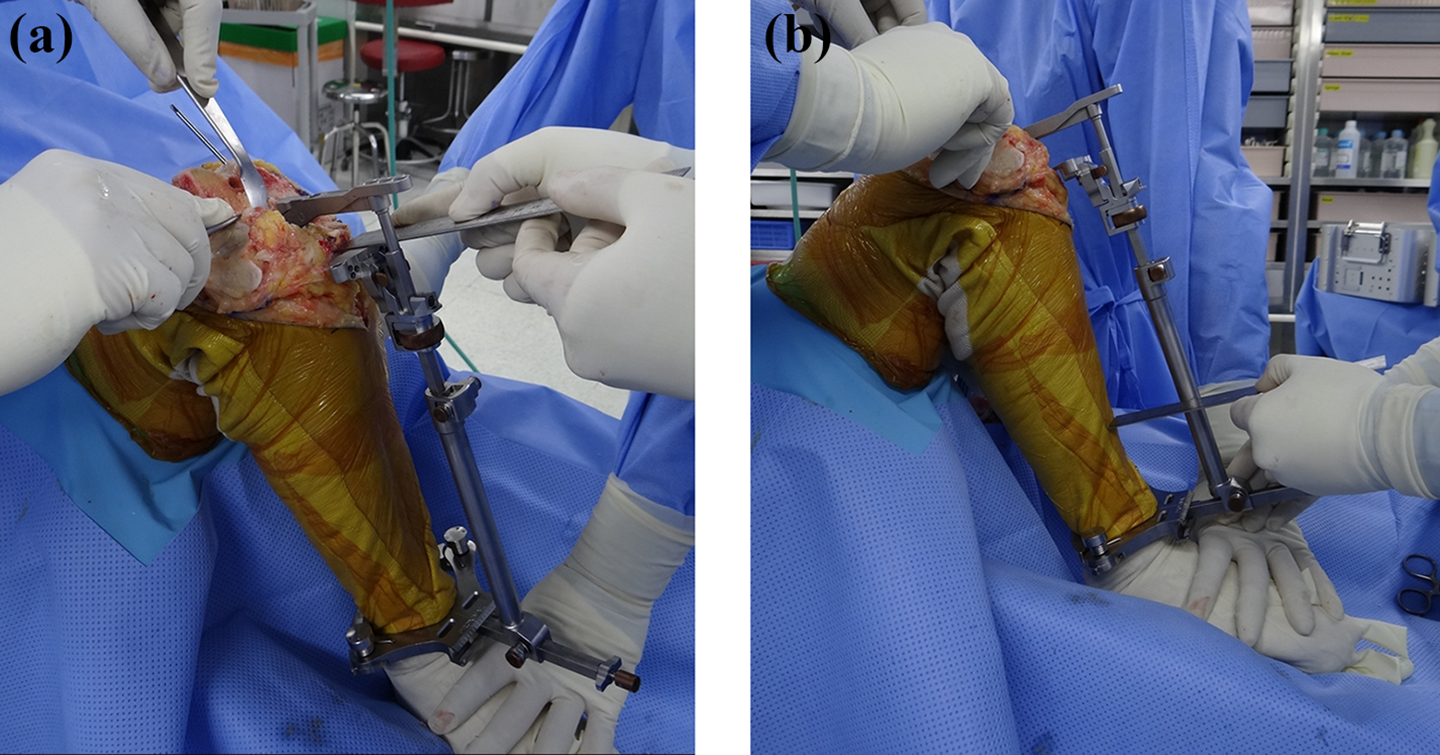
During TKA operation, using extramedullary tibial cutting guide, the measured difference was applied to the distance from the cutting surface (a) and anterior skin surface 20 cm under the tibial cutting surface (b). TKA: total knee arthroplasty.
In group B, the fibula axis line was drawn during the operation. The proximal fibular neck and lateral malleolus were palpated, and a line between the two areas was drawn and determined as the fibular shaft axis. The extramedullary tibial cutting guide was set parallel to the fibular shaft axis line drawn and the cutting slope also followed the reference of each implant.
The cutting slope was decided upon as the reference angle of the implant. A total of four implants were used. The target slope angle was 0° in Scorpio NRG (Stryker, Mahwah, New Jersey, USA; 32 cases in group A and 31 cases in group B), 3° in Zimmer Persona (Zimmer, Warsaw, Indianna, USA; 18 cases in group A and 6 cases in group B), 5° in ACS (Implantcast GmbH, Buxtehude, Germany; 24 cases in group A and 26 cases in group B), and 7° in Nexgen LPS-flex (Zimmer; 1 case in group A and 13 cases in group B).
Evaluation methods
Postoperatively, the posterior slope angle was measured using the lateral tibial radiograph. The angle was measured as the line between the inferior surface of the tibial component and the anatomical axis of the tibia (Figure 3).

Postoperative radiographs of the tibia. The posterior slope angle, which is the angle between the tibial component and the line perpendicular to the anatomical axis, was measured.
The difference to the target angle between the two groups was compared, and the acceptable range was determined within 3° to the target angle. The ratio of acceptable range between the two groups was compared.
The measurements were evaluated twice independently by two raters with an interval of 1 week.
Statistical analyses
The mean values of the measurements were used as the basis for assessment of the intra- and interobserver reliabilities by calculation of the intraclass correlation coefficients (ICCs). Values greater than 0.75 were considered significant. The ICC values for intra-observer reliability were 0.996 and 0.998, respectively. The ICC value for intra-observer reliability was 0.995. The ICC values for intra-observer and interobserver reliability in our study were found to be above 0.75 in both groups, which represented good reliability and accuracy.
The paired t-test was used to compare the difference to the target angle, and the χ 2 test was used to compare the ratio in acceptable range.
Statistical significance was assumed at p values of <0.05. All statistical analyses were performed with SPSS Statistics version 21.0 (IBM Co., Armonk, New York, USA).
This study was approved by the institutional review board (IRB) of our institution (No. 2018-10-022-001).
Results
The difference to the target angle was 1.8 ± 1.3° (range 0 to 4.4°) in group A and 2.5 ± 1.4° (range 0 to 5.7°) in group B. In group A, the difference was smaller significantly (p = 0.04).
The ratio within the acceptable range was 78.7% (59 of 75) in group A, whereas it was 61.8% (47 of 76) in group B (p = 0.024).
Discussion
The method using tibial cut surface and anterior skin line in lateral radiograph was more accurate and had less difference with the target angle in postoperative tibial component slope angle rather than the method using fibular shaft axis line.
The sagittal malalignment of the components has been related to a higher failure rate, and numerous studies have stressed the importance of accurate component orientation and position. 11,12 The effect of posterior tibial slope angle after TKA was reported by several authors and has been emphasized to obtain acceptable results with TKA. Posterior tibial slope after TKA affects anteroposterior stability, range of motion, and contact pressure within the tibiofemoral joint. 13,14 Excessive posterior slope angle could cause several problems, including posterior tibiofemoral subluxation, polyethylene wear, and loosening of component. 15 –17 Anterior impingement of the post/cam mechanism could also occur with excessive tibial posterior slope. 18
Therefore, studies for successful tibial posterior slope were reported. Okamoto et al. 18 reported a tibial posterior slope at 5° or less for better results of TKA. Kim et al. 11 reported that tibial sagittal alignment within 0–7° could improve the survival rate after TKA.
Consideration for various sagittal references during TKA was reported by several authors. Han et al. 7 reported that the posterior tibial slope changed according to the reference axis. Yoo et al. 4 reported that the anatomical reference used to measure the posterior slope should be identified in studies where the posterior slope is used to evaluate the sagittal alignment of TKA.
Several anatomical landmarks of the tibia in TKA were introduced and used in operations, 4,19 including anatomical axis of proximal and central tibia, anterior and posterior cortical line, and fibular shaft axis. Among these, the fibular shaft axis can be used during operations easily because of the palpable fibula in the proximal and distal areas. Although this reference is well-known and widely applied, its accuracy is not high. 9 The mechanical axis, which is the line from the center of the tibial proximal plateau to the center of the tibial distal plafond, was considered the ideal reference according to some reports. 7 However, the mechanical axis was not consistent due to the osteophytes and bone defects on radiographs, especially in osteoarthritis. The anatomical axis that is not affected by osteophytes or defects in osteoarthritic knees could be consistent.
Moreover, anterior tibial crest was also reported as a reliable reference for posterior slope of TKA because it is easily palpable during the operation and has less soft tissue. 8,20,21 However, the soft tissue thickness should be considered, although there is less soft tissue in that area. Tsukeoka and Tsuneizumi 9 reported that the accuracy of the sagittal reference using the line tibial cut surface and anterior skin under 20 cm using CT images to reflect the thickness of soft tissue in the anterior tibial crest and the reference was almost similar to that of the mechanical axis in the sagittal plane. The distance was measured using the angle between the mechanical axis and the line joining the cutting surface to anterior skin surface under 20 cm multiplied by 3.5 (200 × tan 1°). In this study, the distance obtained from the preoperative radiograph could also consider the soft tissue thickness. Moreover, the sagittal alignment was determined during the operation by just reflecting the distance to the extramedullary tibial guide in preoperative radiograph.
Yoo et el. 4 measured the differences between several anatomical references and reported that the difference between the central anatomical axis and the fibula shaft axis was 3.3°. In the present study, the difference between the anatomical axis and the fibula shaft axis was 3.5°. The posterior slope angle could be affected by these differences, which had an effect on the survival rate of TKA or clinical results. Therefore, a consistent method for the slope is needed to obtain the targeted posterior slope angle.
This study applied this reference to the actual TKA surgery using lateral radiograph obtained preoperatively. The distance to the extramedullary guide between the cutting surface and the anterior skin surface simulated the preoperative planning with lateral radiograph. It was applicable easily, reproducible, and could be confirmed during the TKA operation. The results were more accurate than the method using fibular shaft axis line, which is the widely and easily used method in TKA. However, the thickness of the anterior tissue could be changed during the draping prior to surgery or wrapping the elastic bandage for tourniquet.
Several references to sagittal alignment have been reported. However, a gold standard reference has not been proved. Moreover, the clinical association between each reference was also not proved; therefore, further studies evaluating the association between clinical results and references to prove the standard of TKA slope should be undertaken.
The limitations of this study were the retrospective study design and the small number of patients. Use of the various products and not a single product could also be a limitation. Finally, only radiographic results were evaluated. Large-scale studies with clinical results should be performed.
Conclusion
This study demonstrated that the sagittal reference line using the preoperative lateral radiograph was helpful as a reference guide for the tibial slope in TKA.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.