
Abstract
Background:
During total knee arthroplasty (TKA) for osteoarthritis, the sagittal gap imbalance (SGI) with a relatively large extension gap is an important surgical challenge. We determined the predictors of SGI with a relatively large extension gap and evaluated the surgical outcomes of knees with SGI.
Methods:
551 consecutive cases of primary TKA for osteoarthritis were retrospectively reviewed. The cohort was divided into two groups according to the SGI and statistically matched according to baseline characteristics via the inverse probability of treatment weighting method. Multiple linear and logistic regression analyses were performed to determine the predictors of sagittal gap difference (SGD) and SGI. Intergroup differences in clinical and radiological outcomes were analyzed.
Results:
Of all the knees included, 8.5% (n = 45) presented with SGI with a relatively large extension gap and required femoral sagittal balancing to manage SGI. The hyperextension angle (HA), preoperative joint line convergence angle (JLCA), and the change in posterior tibial slope (PTS) significantly correlated to SGD and predicted SGI with a relatively large extension gap. SGI group showed significant changes in femoral posterior condylar offset and joint line height compared to those without SGI (1.48 vs −0.45, 1.37 vs −0.51, respectively). Postoperative ROM and knee society knee scores were lower in SGI group.
Conclusion:
Knees requiring sagittal balancing to manage SGI with a relatively large extension gap is not uncommon in TKA for osteoarthritic knees. The change in PTS is an independent and modifiable predictor of SGI.
Keywords
Introduction
As normal knee kinematic patterns change after total knee arthroplasty (TKA), which lead to a new dynamic knee balance, gap balancing is an important issue in TKA. 1 Sagittal gap imbalance (SGI) with a relatively large extension gap, which is associated with knees with hyperextension, is one of the main challenges in creating a rectangular gap during TKA. Interestingly, by computer-navigated technique, recent reports have demonstrated that hyperextension is not uncommon, with an increased incidence of up to 11.8% in knees with degenerative osteoarthritis without neuromuscular disorders. 2,3 Furthermore, failure to perform sagittal gap balancing can lead to postoperative genu recurvatum deformities or flexion limitation due to the use of excessively thicker inserts. These issues significantly impair function and worsen patient quality of life. 4 Therefore, the importance of sagittal gap balancing during TKA has been given considerable attention in recent years.
Femoral sagittal balancing such as under-resection of the distal femur or undersizing of femoral components has been traditionally used to manage SGI with a relatively large extension gap in knees with hyperextension. 5 –9 Strictly speaking, SGI with a relatively large extension gap is not just a problem in knees with hyperextension. Rather, it can also occur in knees with preoperative flexion contracture when the knees present a large posterior tibial slope (PTS) that results in an eccentric proximal tibial osteotomy resecting anterior tibia more.
In addition, femoral sagittal balancing, either under-resection of the distal femur or undersizing of the femoral components, has limitations due to the changes in the joint line height (JLH) or femoral posterior condylar offset (FCO). 3,10,11 Therefore, recognizing predictors, especially modifiable factors beyond femoral sagittal balancing, of SGI with a relatively large extension gap that requires sagittal gap balancing procedures during TKA is important. Furthermore, an adequate strategy for sagittal gap balancing should be proposed for knees with either neutral alignment or flexion contracture.
Therefore, the aims of our study were as follows: (1) to determine the incidence and predictors of SGI with a relatively large extension gap that requires sagittal gap balancing procedures and (2) to analyze the clinical and radiological outcomes of knees with SGI in TKA for knees with degenerative osteoarthritis.
Materials and methods
Patient selection
In the present study, the hyperextension angle was defined as the sagittal alignment of the lower extremity as measured by navigation. We assessed the sagittal alignment after exposure of the joint and excision of the cruciate ligaments and menisci to accurately evaluate the posterior capsular laxity by minimizing the mechanical block effects of the cruciate ligaments and menisci (Figure 1).

Hyperextension angle, defined as the sagittal alignment of the lower extremity as measured by navigation.
After gaining approval from the institutional review board, a retrospective review of 1,055 knees treated with primary TKA between 2014 and 2016 was conducted. The review revealed that navigated TKA was performed in 669 knees. The inclusion criteria were as follows: (1) degenerative osteoarthritis and (2) complete medical records, including navigation data, with at least 2 years of follow-up. The exclusion criteria were TKA for causes other than degenerative osteoarthritis, such as post-traumatic osteoarthritis, including fractures or ligament injuries, sequelae of septic arthritis, inflammatory arthritis, and neuropathic arthropathies.
Of the 669 cases of navigated TKA, 102 were excluded owing to post-traumatic arthritis (n = 40), rheumatoid arthritis (n = 30), sequelae of septic arthritis (n = 21), and lack of navigation data (n = 11). After an additional exclusion of 16 knees with <2 years of follow-up, the remaining 551 knees of 458 patients were included in the final analyses. The mean age and follow-up duration of the cohort were 70.93 ± 5.84 years and 34.32 ± 10.39 months, respectively. For the subgroup analyses, the study cohort was divided into two groups according to SGI with a relatively large extension gap.
Surgical technique
All TKAs were performed by the same surgeon using a computer-navigated technique. The navigation was performed using the OrthoPilot version 4.2 computer-aided surgery system (B. Braun Melsungen AG, Melsungen, Germany). The minimal detectable angular and length changes of the navigation system were 1° and 1 mm, respectively. All the patients underwent TKA using a cemented, posterior cruciate-substituting design (e.motion Total Knee System, B. Braun Melsungen AG) and resurfacing of the patella. A tension device was used to evaluate the sizes of both the medial and lateral gaps and stability, with the knees at extension (0° flexion) and at 90° flexion during the surgery.
The surgical technique for navigation-assisted TKA was described previously. 12,13 After exposure of the joint through a medial parapatellar arthrotomy, registration of the knee, hip, ankle joints, and anatomical landmarks was performed with the navigation system. The alignment of the lower extremity was measured and recorded in the coronal and sagittal planes after exposure of the joint and excision of the cruciate ligaments and menisci, but prior to the preliminary release of soft tissue. Soft tissue release for the acquisition of mediolateral balancing with the knee at extension was carefully performed using real-time feedback from the navigation system. The tibia was resected first, and the target of the resected PTS in the sagittal plane was adjusted according to the strategy for PTS modification with a range of 0–10° (Figure 2). The medial and lateral initial extension and flexion gaps were recorded with the knee at extension and 90° flexion. Bone resections of the distal femur were targeted so that the distal transverse plane cut was 0° relative to the mechanical axis of the femur. The goal set for the difference in the medial and lateral gaps was <2 mm at extension. The rotation of the femoral component was set to achieve a difference in the medial and lateral flexion gaps of <2 mm. 14 Both medial and lateral final gaps were measured using the navigation system after applying tension with the knees at extension and 90° flexion. All the knees included in the present study showed a difference of ≤2 mm in gaps at extension and 90° flexion. After insertion of a trial insert, the insert thickness was determined to be adequate when the sagittal alignment with the knee at extension during navigation remained within 0–3° of the flexion contracture. Implantation was performed if the coronal and sagittal alignments with the trials were satisfactory. Coronal and sagittal alignments were measured again after implantation. The amounts of proximal tibial and distal femoral resections, sizes of the femoral and tibial components, thicknesses of the inserts, and initial and final medial and lateral gaps were recorded with the knees at extension and 90° flexion.

Stepwise strategy for sagittal balancing in total knee arthroplasty for osteoarthritic knees. After categorizing patients according to hyperextension angle (HA) and preoperative posterior tibial slope (PTS), the target of the resected PTS was adjusted. The sagittal gap difference was calculated using the determined medial and lateral gaps in the knees at extension and 90° of flexion. The sagittal gap difference was managed with under-resection of the distal femur, use of thicker inserts, or undersizing of the femoral component.
Definitions of SGD and SGI with a relatively large extension gap than flexion gap
After tibial resection and recording of the initial medial and lateral gaps, the medial and lateral gaps before femoral sagittal balancing were determined on the basis of the assumption that the distal femur was anatomically resected at an amount equal to the distal thickness of the best matched implant, and the selected rotation of the femoral component was applied (Figure 3). By assuming that the implant size was a continuous variable, the best matched implant was determined by rounding off the decimal point of the implant size matched to the anteroposterior [AP] diameter of the knee measured by the navigation system.

Determination of the medial and lateral gaps before femoral sagittal balancing and calculation of the sagittal gap difference (SGD). The medial and lateral gaps before femoral sagittal balancing in the knees at extension and 90° flexion were measured with the assumption that the distal femur was anatomically resected by an amount equal to the distal thickness of the best matched implant, as determined on the basis of the anteroposterior and mediolateral knee diameters. The selected rotation of the femoral component was applied for coronal gap balancing. The SGD was calculated as the difference between the lower medial or lateral gaps in the knees at extension and 90° flexion. In this case, the medial and lateral flexion gaps after the application of adequate rotation of the femoral component were determined as −6 and −4 mm, respectively. The best matched implant size was No. 4, and its distal thickness was 8.5 mm. The medial and lateral extension gaps were 1.5 and 4.5 mm, respectively. The SGD was 7.5 mm.
The sagittal gap difference (SGD) was calculated as the difference between the lower medial or lateral gap before femoral sagittal balancing with the knees at extension and 90° flexion using the following equation: SGD before femoral sagittal balancing = lower medial or lateral extension gap − lower medial or lateral flexion gap (Figure 3). Positive values indicated a larger extension gap, whereas negative values indicated a smaller extension gap. As the mean difference in AP diameter between the femoral implants was approximately 3 mm, not only undersizing of the femoral components but also under-resection of the distal femur was required to manage SGI with a relatively large extension gap when it was defined as a SGD of ≥4 mm. Therefore, SGI with a relatively large extension gap was defined as a SGD of ≥4 mm with a larger extension gap than flexion gap in the present study. For sagittal balancing in cases with a relatively larger extension gap than flexion gap, resection of the distal femur was reduced by up to 3 mm or the femoral component was downsized.
Evaluation of radiological and clinical outcomes
Full-length and erect AP lateral-view radiographs were obtained preoperatively and at the final follow-up visit to assess limb alignment and the position of the components. The parameters were measured using a picture archiving and communications system. The hip-knee-ankle (HKA) angle was used to measure the mechanical axis deviation between the femur and tibia according to the criteria described by Cooke et al., in which a positive value denotes varus and a negative value denotes valgus. 15 JLCA was defined as the angle formed by two articular tangential lines of the distal femur and proximal tibia with similar sign conventions as those used for HKA. The coronal femoral component angle (α), coronal tibial component angle (β), and sagittal femoral component angle (γ) were evaluated according to the American Knee Society’s guidelines (Figure 4). 16 The FCO and PTS were also obtained from the lateral view of the knee joint. PTS was defined as the angle between the lateral tibial plateau line or the cutting surface of the proximal tibia and a line perpendicular to the tibial longitudinal axis and was measured using the circle method (Figure 5). 17 FCO was defined as the distance from the posterior cortical margin to the posterior condyle (Figure 4). 18 JLH was defined as the distance between the line connecting the most distal ends of the medial and lateral femoral condyles and a line parallel to the apex of the fibular head (Figure 5). 19 Postoperative changes in parameters were defined as follow: preoperative–postoperative value in measurements of parameters. The knee range of motion (ROM) was measured using a goniometer. The Western Ontario and McMaster Universities Osteoarthritis (WOMAC) index, Knee Society Knee Score (KSKS), and Knee Society Function Score (KSFS) were assessed preoperatively and at the final follow-up. 20,21

Preoperative limb alignment analysis including hip-knee-ankle angle and joint line convergence angle, the postoperative American Knee Society’s radiographic evaluation and measurement of the posterior tibial slope. The α and β angles were defined as the coronal femoral and tibial component angles, respectively. The γ angle was defined as the sagittal femoral component angle. HKA: Hip-knee-ankle, JLCA: Joint line convergence angle, PTS: Posterior tibial slope.

Measurements of the joint line height and posterior condylar offset.
Statistical analyses
IBM SPSS Statistics version 22.0 software (IBM Corp., Armonk, NY, USA) was used for the statistical analysis. The level of statistical significance was set at p < 0.05 for this study. All data are presented as mean ± standard deviation for continuous variables or as number and percentage for categorical variables. PSs were estimated using multiple logistic regression analyses, with SGI as the dependent variable. Preoperative parameters, including sex, age, BMI, preoperative HKA angle, ROM, and WOMAC index, were used to determine the PSs.
Two groups were statistically matched via the inverse probability of treatment weighting method to minimize the variability of the preoperative characteristics and to reduce the effects of possible confounding factors in the two groups. The Fisher exact test was used to evaluate categorical variables. The independent and paired t tests were used to evaluate continuous variables as appropriate. Correlations between the variables were assessed using the Spearman rank correlation analysis. Correlations between SGD and the other variables were evaluated to determine the factors that affect SGD. Statistically significant correlating factors were analyzed using a multiple linear regression analysis to rule out confounding factors. Multiple linear regression using a stepwise method was performed with statistically significant factors, and the eligibility criterion for the predictive model was p < 0.10.
Multiple logistic regression analysis was used to identify independent predictors of SGI with a relatively large extension gap and was adjusted for possible confounding factors such as age, sex, preoperative ROM, preoperative HKA angle, JLCA, PTS, FCO, JLH, thickness of the resected tibia, and tibial slope change. An intergroup comparison of the intraoperative measurements and radiological and clinical parameters was performed according to SGI.
A post hoc test was performed to determine the sample size using two-tailed correlation, linear regression, logistic regression, and independent t tests, with a significance level (α) of 0.05 and a power of 0.8. Calculations based on a sample size (563 knees in SGI group and 551 knees in control group) indicated adequate power to detect a significant difference and relationship between the parameters in the present study.
Results
The baseline characteristics, navigation data, and radiological parameters of the present study are summarized in Table 1. Of the 551 knees treated with primary navigated TKA for degenerative osteoarthritis, 8.5% (n = 45) presented with SGI with a relatively large extension gap and required femoral sagittal balancing, including under-resection of the distal femur and undersizing of the femoral components. The incidence of SGI with a relatively large extension gap was increased up to 15.0% in the knees (n = 36) with HAs of ≥0°, while 3.5% (n = 11) of the knees with flexion contracture required femoral sagittal balancing for SGI. The SGI group demonstrated a larger HA, preoperative JLCA, PTS, and postoperative PTS changes than the control group (Table 1).
Baseline characteristics, navigation data, and radiological component alignments of the patients according to SGI with a relatively large extension gap.

The variables are presented as mean ± standard deviation or number (%).
IPTW: Inverse Probability of Treatment Weighting, BMI: Body mass index, ROM: Range of motion, HKA: Hip-knee-ankle, JLCA: Joint line convergence angle, PTS: Posterior tibial slope, HA: Hyperextension angle, SGD: Sagittal gap difference, SGI: Sagittal gap imbalance α angle: Coronal femoral component angle, β angle: Coronal tibial component angle, γ angle: Sagittal femoral component angle.
The multiple linear regression analysis revealed that the HA, preoperative JLCA, changes in PTS and resected tibial thickness were significantly related with SGD (Table 2). Furthermore, the multiple logistic regression analysis revealed that increases in HA, preoperative JLCA, and changes in PTS were independent predictors of SGI with a relatively large extension gap (Table 3).
Univariate and multivariate linear regression analyses of sagittal gap differences before femoral sagittal balancing.

CI: Confidence interval, BMI: Body mass index, ROM: Range of motion, HKA: Hip-knee-ankle, JLCA: Joint line convergence angle, HA: Hyperextension angle, PTS: Posterior tibial slope. aFactors used in the Spearman rank correlation analysis, independent-samples t tests, and multivariate analysis. bAnalyzed using independent-samples t tests. R = 0.798, R 2 = 0.636, adjusted R 2 = 0.635, p < 0.001.
Multiple logistic regression analysis of significant sagittal gap imbalance with a relatively large extension gap.

CI: Confidence interval, BMI: Body mass index, ROM: Range of motion, HKA: Hip-knee-ankle, JLCA: Joint line convergence angle, PTS: Posterior tibial slope, HA: Hyperextension angle. Multivariate logistic regression analysis was performed by controlling all the factors in Table 3.
Less of the distal femur and proximal tibia were resected, and thicker inserts were used in the SGI group than in the control group. A significant decrease in FCO and depression of the JLH were demonstrated in the SGI group (Table 4). Furthermore, SGI group showed lower postoperative ROM and KSKS compared to control group. Postoperative WOMAC index were not significantly different between both groups. No complications such as recurrence of recurvatum, osteolysis, and early aseptic loosening were encountered.
Intergroup comparison of the operative findings and radiological and clinical parameters.
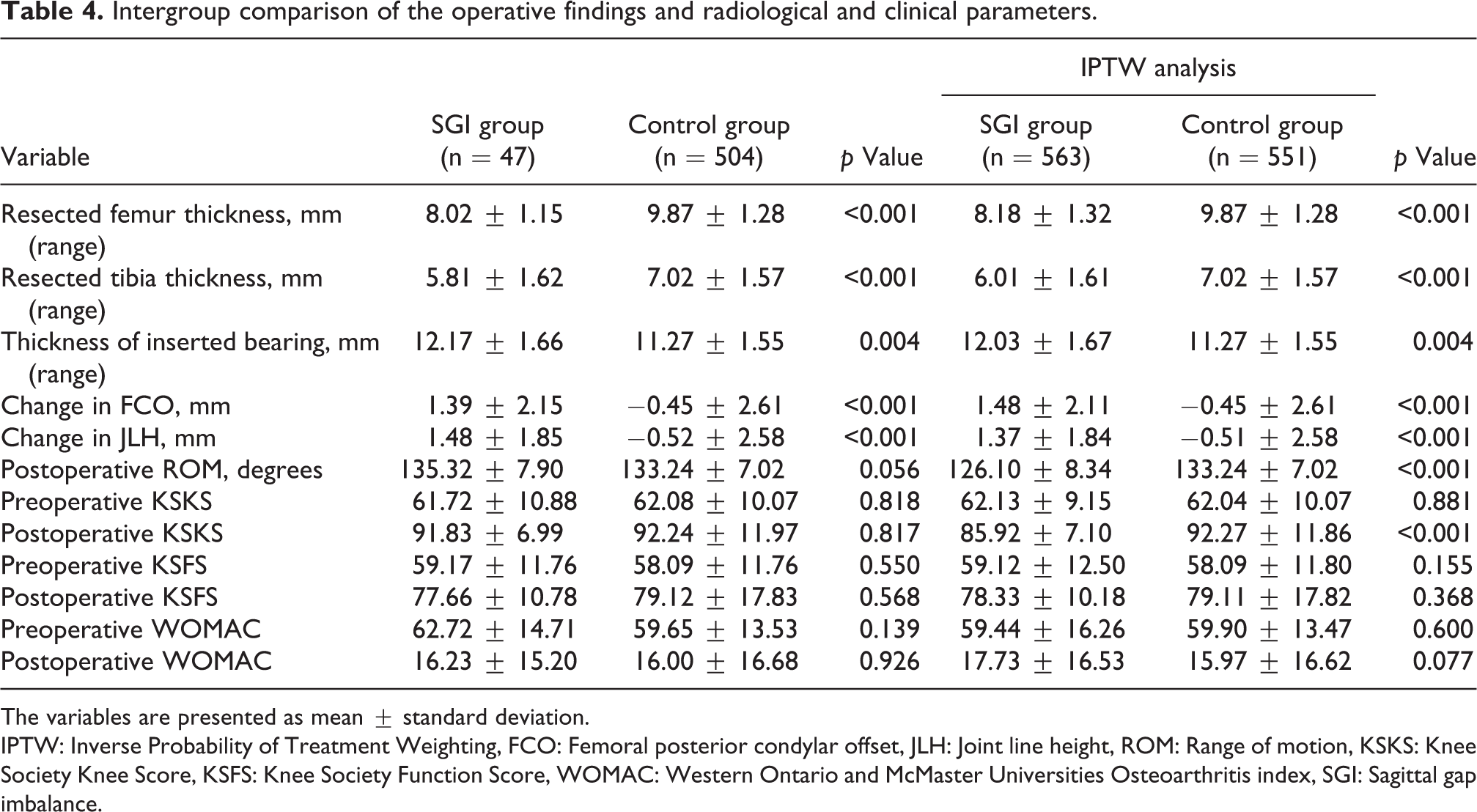
The variables are presented as mean ± standard deviation.
IPTW: Inverse Probability of Treatment Weighting, FCO: Femoral posterior condylar offset, JLH: Joint line height, ROM: Range of motion, KSKS: Knee Society Knee Score, KSFS: Knee Society Function Score, WOMAC: Western Ontario and McMaster Universities Osteoarthritis index, SGI: Sagittal gap imbalance.
Discussion
The most principal findings of the present study are that osteoarthritic knees requiring femoral sagittal balancing for SGI with a relatively large extension gap are not uncommon and SGI was present even in knees with flexion contracture. Furthermore, preoperative HA and JLCA, and postoperative changes in PTS were determined as independent predictors of SGI with a relatively large extension gap.
Genu recurvatum has been believed to be related to neuromuscular disorders, reverse anterior tibial slope after high tibial osteotomy, valgus deformities, or ligamentous laxity in patients with inflammatory arthritis. 5,22 –28 However, against the traditional belief regarding genu recurvatum, recent reports have demonstrated that knees presenting with hyperextension of ≥5° were frequently detected by navigation, with an incidence of 10.2% in knees treated with TKA for degenerative osteoarthritis. 3 The main obstacle to creating a rectangular gap balance is SGI with a relatively large extension gap just after tibial resection in TKA for osteoarthritic knees with hyperextension. However, even in knees with either neutral sagittal alignment or flexion contracture, femoral sagittal balancing procedures are required. Therefore, the present study aimed to determine the incidence of SGI with a relatively large extension gap. SGI is not uncommon, with an incidence of 8.5% of knees with degenerative osteoarthritis and 3.5% of knees even with flexion contracture required femoral sagittal balancing procedures.
Various surgical options for femoral sagittal balancing, such as under-resection of the distal femur, undersizing of the femoral components and use of thicker inserts have been recommended to manage and overcome SGI with a large extension gap during TKA. 5 –9 However, evidences demonstrated that undersizing of the femoral components can reduce the posterior capsular tension, which can independently increase the extension gap. 29 –31 Furthermore, either under-resection of the distal femur or undersizing of the femoral components results in changes in JLH or FCO and can impair the clinical outcomes. 3,10,11 Failure to achieve a rectangular gap owing to an SGI with a relatively large extension gap during TKA can result in postoperative genu recurvatum deformity or compel surgeons to use thicker bearings, which decrease the further flexion; this may lead to impaired patient quality of life and function. 4 These findings may highlight that sagittal balancing strategies with femoral modification alone are not sufficient to manage the SGD and can negatively affect the clinical outcomes. Therefore, the predictors of SGD and SGI with a relatively large extension gap, especially modifiable factors, should be identified and managed to avoid excessive femoral sagittal balancing.
The present study demonstrates that SGD before femoral sagittal balancing was determined on the basis of HA, preoperative JLCA, and postoperative changes in PTS. Moreover, increases in HA, preoperative JLCA, and postoperative changes in PTS were independent predictors of SGI with a relatively large extension gap. Posterolateral capsuloligamentous structures may be subject to chronic excessive tensile forces that can result in recurvatum deformities in varus osteoarthritis. 32,33 Similar to a recent report, our study demonstrates that most of the knees with SGI with a relatively large extension gap presented varus alignment at an incidence of approximately 84%. 3 This could explain the relationships of SGD and SGI with a relatively large extension gap to posterolateral capsuloligamentous laxity, expressed as HA and JLCA.
The relationship between the PTS and the sagittal gap in TKA has been demonstrated. A preoperative PTS of >10.36° (the reported cutoff value) can lead to a relatively large extension gap owing to the removal of greater amounts of the anterior tibia. 34,35 Furthermore, Okazaki et al. reported that the influence of the change in PTS by 5° on the flexion gap was approximately 1 mm with PS-type TKA. 36 Consistently, the present study found that increased postoperative changes in PTS with an insufficient PTS of tibial resection relative to the preoperative PTS, as a sagittal bony structural factor, correlate with SGD and SGI with a relatively large extension gap before femoral sagittal balancing.
Among the predictors of SGI identified in the present study, postoperative changes in PTS may be modifiable intraoperatively by increasing the PTS during tibial resection. However, the longevity of prostheses should be considered a higher priority than modification of PTS because the principal objective of TKA is achievement of a durable joint. Currently, no consensus has been reached on the optimal and safe PTS range for patients who undergo TKA. Although the recommendation for PTS varies for each type of implant, a mean PTS of 0–3° is recommended for PS-type TKA owing to the high stability of tibial implants. 37 –39 In addition, an increase in PTS can result in impingement of the post-cam mechanism in the PS-type TKA, and a PTS of >10° may cause wear or fracture due to excessive tension. 38,40 –42 By contrast, Lee and Kim et al. conducted a finite element study and demonstrated that contact stresses were distributed over a wider area in knees with a PTS of 10° than in those with a PTS of 0°. Moreover, stresses on collateral ligaments were lower in the knees with a PTS of 10° than in those with a PTS of 0°. 43 Therefore, we increased the PTS, but tried not to exceed 10°. A maximum of 10° was indicated only in knees with a HA of >10° or 5–10° and pathological PTS of >10°.
To the best of our knowledge, this is the first matched study to determine the predictors of SGI with a relatively large extension gap and compare the surgical outcomes after TKA in knees with SGI. Orthopedic surgeons should be aware that knees that present with SGI with a relatively large extension gap are not uncommon and SGD and the incidence of SGI can be increased when the resected PTS is systematically targeted in knees with large preoperative JLCA, HA and PTS. The main predictors of SGI with a relatively large extension gap are increases in HA, preoperative JLCA, and PTS changes that represent posterolateral capsuloligamentous laxity and a sagittal structural factor. Therefore, PTS modifications to reduce PTS changes should be considered to overcome SGI with a relatively large extension gap, and to eventually avoid excessive under-resection of the distal femur and undersizing of the femoral components in TKA for osteoarthritic knees.
The present study has some limitations. First, its retrospective study design is inherently disadvantageous. Second, although soft tissue release may affect SGDs, this was not included in the present analysis. Third, the present study was limited by the fact that we categorized the knees according to HA or preoperative PTS on the basis of empirical evidence. However, the focus of this study was to convey the concept of the sagittal gap balancing including PTS modification. Further studies on the development and validation of a concise approach to sagittal balancing and determination of the optimal and safe PTS range are needed. Fourth, PTS modification with a restrictive range might not be suitable for TKA using standard instrumentation without a computer-assisted navigation system because the accuracy of the tibial and femoral cut cannot be assured. Fifth, the long-term results for post-wear, fracture, osteolysis, and aseptic loosening were not assessed.
Conclusion
Sagittal balancing to manage SGI with a relatively large extension gap is frequently required in TKA for osteoarthritic knees. Posterolateral capsuloligamentous laxity, expressed as increased HA and preoperative JLCA, and a sagittal structural factor, expressed as PTS change are independent predictors of SGI.
Footnotes
Author contributions
Conception and design: SB Han, KH Shin. Data collection: SB Kim, CS Lee, KM Jang, KH Shin. Analysis and interpretation: KH Shin, SB Han. Writing the article: KH Shin. Critical revision of the article for intellectual content: SB Han, KH Shin. Final approval of the article: KH Shin, SB Han. Statistical analysis: KH Shin. Obtained funding: Not applicable. Overall responsibility: SB Han.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Approved from the institutional review board of Anam Hospital of Korea University Medical Center.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.