
Abstract
Objective:
Insall advocated that a successful clinical outcome of total knee arthroplasty (TKA) depends on soft tissue balance procedure. Spacer blocks, balancer, and instrumented tibial sensor (VERESENSE, OrthoSensor, Dania, Florida, USA) are the current methods of soft tissue balancing during TKA. The purpose of the study is to assess intraoperative medial and lateral tibiofemoral compressive force (TFCF) using novel insert sensor and investigate the relationship between TFCF and patient-reported outcome measurements (PROMs).
Methods:
Twenty-five patients who underwent bicruciate stabilized (BCS) TKA were evaluated retrospectively. We measured intraoperative medial and lateral TFCF in neutral position as well as the force ratio (FR %:medial TFCF/medial + lateral TFCF) in varus and valgus position using the novel insert sensor throughout the range of motion (ROM) and assessed the relationship between intraoperative medial and lateral TFCF and PROM at 6 months after TKA.
Results:
Medial TFCF increased and lateral TFCF decreased throughout ROM. The mean FR was 0.44% ± 0.22 throughout ROM. Medial and lateral TFCF differences at 60° of ROM in neutral position showed a positive correlation with physical function in Western Ontario and McMaster Universities scores (r = 0.60, p < 0.05). Medial and lateral TFCF differences at 30° and 140° of ROM in valgus stress test showed a positive correlation with symptoms in 2011 Knee Society Scores (r = 0.49, p < 0.05; r = 0.51, p < 0.05).
Conclusion:
The present study revealed that BCS TKA reproduces the coronal laxity, which is similar to healthy knee. These results suggest that intraoperative medial stability is important for function and symptoms, therefore, surgeons should not release medial soft tissue for achieving better clinical outcomes after BCS TKA.
Level of Evidence:
II
Keywords
Introduction
Total knee arthroplasty (TKA) is a common and cost-effective surgical treatment for osteoarthritis in the knee, with a proven effect for pain reduction and better quality of life. 1 –3 However, 10–20% of primary TKA patients are not satisfied according to the patient-reported outcome measurements (PROMs). 4 –7 Surgical technique of TKA to improve patient satisfaction includes (1) accurate osteotomy, (2) component alignment, and (3) acquisition of good soft tissue balance. Today’s rapid orthopedic technological developments, such as preoperative 3D planning software, patent-specific instruments, and navigation systems, reinforced the accuracy of osteotomy as well as component alignment. Meanwhile, knee revision cases due to instability have been estimated to cause 18.7% of total TKA reoperations each year, which in part may be because of improper balancing. 8,9 In general, acquisition of soft tissue balance is dependent on the surgeon’s technique. W. Norman Scott 10 advocated “TKA is a soft tissue procedure” in the 1980s. Ligamentous balancing is compared to be an important variable for improving postoperative patient satisfaction and implant survivorship. 11 Soft tissue balance has been traditionally achieved with the aid of rudimentary tools like blocks, laminar spreaders, and balancer. The perception of balance is subjective and varies between surgeons. 12 Few cases of soft tissue imbalance are detectable during TKA and distraction force is applied for subjective visual evaluation of the surgeon 13 ; therefore, measured imbalances have often been corrected by soft tissue releases, such as multiple-puncture needle techniques, 14 or by modifications to bone resections. 15 There is no consensus on whether the goals of balancing should be based on tibiofemoral gaps, distraction forces, and varus and valgus moments to cause condylar liftoff.
The VERASENSE (OrthoSensor, Dania, Florida, USA) tibial trial insert is a microelectoric device that provides intraoperative peak loads and contact points (CPs) in the medial and lateral TKA compartments throughout the ranges of motion (ROMs) 15,16 ; therefore, real-time feedback enables confirmation of kinematics and acquisition of good soft tissue balance during TKA.
In the current study, we measured tibiofemoral compressive force (TFCF) during TKA using an insert sensor developed independently. There were three purposes for conducting this study: (1) to evaluate the intraoperative medial and lateral TFCF in bicruciate stabilized (BCS) TKA, both the anterior and posterior cruciate ligaments are substituted with a dual cam/postmechanism, which has resulted in more normal tibiofemoral kinematics; (2) to investigate the correlation between the intraoperative medial and lateral TFCF and the PROM; and (3) to determine a novel surgical technique.
Patients and methods
Between December 2017 and October 2018, 72 consecutive primary TKAs due to varus osteoarthritis of the knee (Kellegren–Lawrence: grade 4) were performed using BCS prosthesis (JourneyⅡBCS, Smith& Nephew, Inc., Memphis, Tennessee, USA; Figure 1). The study excluded left knees intraoperatively, which accounted for 32 knees. Patients’ resected tibial sizes were measured, and those that matched with sizes 2, 5, and 6 of tibial tray were not included as subjects. Cases that required 10 mm or thicker insert were also a part of our exclusion criteria. These exclusions derived from the limited availability of insert sensor sizes, thicknesses, and right knee only used during this study (Figure 1). Cases in which the difference in the prosthetic alignment between the preoperative three-dimensional computed tomography (3DCT) plan and postoperative 3DCT image was greater than 3° were considered outliers (15 knees; Figure 1).

Flow diagram including number of patients. TKA: total knee arthroplasty; TFCF: tibiofemoral compressive force; 3DCT: three-dimensional computed tomography.
All TKAs were performed by the same surgeon (TK) and exposed with medial parapatellar approach. At first, the distal femoral cutting guide block was aligned using an intramedullary guide, followed by the alignment of proximal tibia cutting block using an extramedullary guide. For femur and tibia, a standard 6° valgus angle guide and 5° posterior inclination guide were used for all patients. The rotational alignment was adjusted to the surgical epicondylar axis for the femoral component and medial one-third of tibial tuberosity at the level of patellar-tendon attachment for the tibia component. All femoral components were inserted with cement and the tibial components were inserted without cement on the porous tantalum modular tibial component. On the first day after TKA, patients were allowed to walk with or without assistive devices after the drainage tube had been removed. The postoperative mean hospital stay for rehabilitation was 23.2 days (14–34 days). The hospital ethics committee approved the study protocol, and the patients provided informed consent for participation.
We retrospectively evaluated a pilot series of 25 patients with the use of the novel insert sensor used in conjunction with BCS (Figure 1). A unique insert sensor (Marusan Name Co. Ltd., Yokohama, Japan) was developed for this study to make it compatible with BCS knee. Seven thin pressure sensors were embedded in the insert to divide measurement regions (Figure 2). TFCF was measured medially and laterally using a thin insert sensor (Marusan Name, Co. Ltd, Yokohama, Japan; Figure 3). The pressure sensor is capable of measuring pressure up to 2000 kgf (1 kgf = 0.0098 N). A transducer was made using an open-source electronics platform (Marusan Name Co. Ltd) to convert pressure to electronics voltage. The complex of the insert sensor and transducer was connected to a personal computer to record the TFCF data (Figure 3). The measurement area of the insert sensor was divided into seven regions of interest (ROI) (Figure 4): the anterior medial region (ROI 1), the central medial region (ROI 2), the posterior medial region (ROI 3), anterior post region (ROI 4), the anterior lateral region (ROI 5), the central lateral region (ROI 6), and the posterior lateral region (ROI 7). With the tibial component (size: 3.4) for the tibia, femoral component, and patellar component in place, the standard polyethylene trial was inserted and the knee was reduced. The knee was assessed manually to confirm that the joint was not excessively tight or loose in the coronal or sagittal planes in extension and flexion. At that time, the size of the standard polyethylene trial of 10 mm or more was excluded. With the insert sensor inserted, the knee was taken into extension. After medial parapatellar arthrotomy was repaired by suturing more than three stitches to ensure appropriate soft tissue tension during evaluation of the knee joint, we assessed medial and lateral TFCF, compressive force of anterior post and CP in six positions: 10°, 30°, 60°, 90°, 120°, and 140° of flexion. Visible varus–valgus (V-V) stress testing was performed in six positions to assess any laxity present in the collateral ligaments. For V-V laxity, the surgeon applied maximum manual varus and valgus stress to the knee at six positions.

A novel insert sensor is equipped with seven thin pressure sensors that measure pressure up to 2000 kgf (Marusan Name Co. Ltd, Yokohama, Japan).

In intraoperative measurement, tibiofemoral compressive force was measured medially and laterally using a novel insert sensor. A transducer was developed using an open-source electronics platform (Marusan Name Co. Ltd) to convert pressure to electronics voltage.
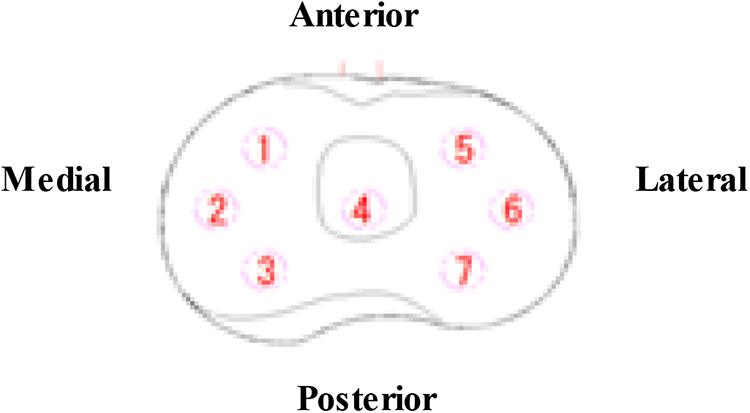
The measurement range of the insert sensor was divided into seven regions of interest (ROI): the anterior medial region (ROI 1), the central medial region (ROI 2), the posterior medial region (ROI 3), anterior post region (ROI 4), the anterior lateral region (ROI 5), the central lateral region (ROI 6), and the posterior lateral region (ROI 7).
Soft tissue balancing was thereby quantitatively retrospectively defined using the force ratio (FR %), defined as the ratio of the medial TFCF over the total forces measured on the tibial plateau (medial TFCF/medial + lateral TFCF). A ratio of 0.5% indicates equal lateral and medial forces. This target has traditionally been the target for standard total knee designs. 15 –17
However, BCS design TKA considered in the current study more closely represents the native anatomy (e.g. including a 3° oblique joint line). Consequently, the target was modified to allow for higher forces on the medial side compared to the lateral, particularly in high flexion. The target loads thereby more closely match the condition of the intact knee, associated with rollback of the lateral femoral condyle in flexion and relaxation of the lateral collateral ligament. 18 Relatively minor surgical corrections were needed, attributed to the normal nonarthritic status of the specimen.
The preoperative plan was developed using 3DCT data of the entire extremities in all cases. A postoperative CT scan was obtained 4 weeks after TKA. The 3D data of femoral and tibial components were fit to postoperative 3DCT image (Figure 5). The femur and tibial of the postoperative 3DCT images were superimposed onto those of the preoperative 3DCT plan using computer software (ZedView, ZedKnee; LEXI Co., Ltd, Tokyo, Japan). The absolute differences in the prosthetic alignment between the preoperative 3DCT plan and postoperative 3DCT image were measured using six parameters: coronal, sagittal, and axial alignment of the femoral and tibial prostheses. Prosthetic alignment differences greater than 3° between preoperative 3DCT plan and postoperative 3DCT image were considered as outliers (Figure 5 and Table 1). 19,20

Preoperative plan 3DCT was shown. 3D computer-aided design (CAD) data of femoral and tibial components were fit to 3DCT image. The blue components indicate the preoperative plan image; the yellow components indicate the postoperative component.
Absolute differences in the prosthetic alignment between the preoperative 3DCT plan and postoperative image in each plane.

3DCT: three-dimensional computed tomography; TEA: transepicondylar axis; AP: anteroposterior; PCA: posterior condylar axis.
The 2011 Knee Society Scores (KSS) 21 was developed as a new patient-derived outcome measure to better characterize symptoms, patient satisfaction, expectation, and physical activities after TKA. The Western Ontario and McMaster Universities (WOMAC) scores have been extensively tested for validity, reliability, feasibility, and responsiveness for measuring changes after different osteoarthritis of the knee intervention. 22 The 2011 KSS and WOMAC scores were surveyed and evaluated at 6 months postoperatively.
Statistical analyses
Means and standard deviations were used to describe the data. All statistical analyses were performed with SPSS version 24.0 software (SPSS Inc., Chicago, Illinois, USA). Statistical significance was set at a p value of <0.05. The Shapiro–Wilk test for normal distribution was applied to the variables to verify normality for all data presented in the current study. The differences between medial and lateral TFCF were subsequently assessed using a two-sided paired t-test. We performed Spearman’s rank correlation analysis to assess the correlations of intraoperative TFCF difference between the medial and lateral compartments throughout ROM and postoperative 2011 KSS and WOMAC scores. A statistical power analysis was performed before the present study. Sample size was calculated using the computer software G* Power 3.1.9.2 (Heinrich Heine Universität Düsseldorf, Düsseldorf, Germany), showing that 25 knees were necessary for the six predictors (power = 0.80; α = 0.05; effect size = 0.20).
Results
Medial TFCF increased and lateral TFCF decreased throughout ROM (Figure 6). It suggests that BCS prosthesis guided medial pivot movement after flexion angle of 30° and screw home movement at flexion angle of 10°. The FR started with a mean of 0.35 at full extension and then slowly increased until reaching 0.66 at 140° of flexion. The mean FR was 0.44% ± 0.22 throughout ROM. Only two knees were engaged between anterior cam and post in posterior inclination of tibia with 6° and 8°. Patients with postoperative ROM of less than 120° flexion often exhibited medial CP between 90° and 140° flexion to be at ROI 1 rather than ROI 3 and lateral CP to be at ROI 5 rather than ROI 7.

Mediolateral compressive force (N) throughout range of motion.
The FRs in varus stress test increased and were 0.5 or higher throughout ROM. The FRs were constant after 90° of ROM (Figure 6). The FRs in valgus stress test increased and were 0.4 or less throughout ROM. The FRs were constant after 90° of ROM. Unlike varus stress test, medial TFCF increased at ROM of 30–60° (Figure 7).

We assessed medial and lateral TFCF in neutral position, varus and valgus stress test throughout range of motion (10°, 30°, 60°, 90°, 120°, and 140° of flexion). Soft tissue balancing was thereby quantitatively defined using the force ratio (FR %), defined as the ratio of the medial TFCF over the total forces measured on the tibial plateau (medial TFCF/medial + lateral TFCF).
Correlations of intraoperative TFCF difference between the medial and lateral compartments throughout ROM and postoperative 2011 KSS and WOMAC scores at 6 months after TKA are presented in Table 1. Medial and lateral TFCF differences at 60° of ROM in neutral position showed a positive correlation with physical function in WOMAC scores (r = 0.60, p < 0.05). Medial and lateral TFCF differences at 120° of ROM in varus stress test showed a positive correlation with stiffness in WOMAC scores (r = 0.59, p < 0.05). Medial and lateral TFCF differences at 140° of ROM in valgus stress test showed a negative correlation with physical function in WOMAC scores (r = −0.58, p < 0.05). Medial and lateral TFCF differences at 30° and 140° of ROM in valgus stress test showed a positive correlation with symptoms in 2011 KSS (r = 0.49, p < 0.05, r = 0.51, p < 0.05).
Discussion
The principal findings of this study were that BCS TKA (substituting anterior cruciate ligament [ACL]) reproduces the coronal laxity of the intact knee, demonstrating the increased medial TFCF and decreased lateral TFCF throughout ROM.
The FRs in varus and valgus stress test increased and were 0.5 or higher in varus stress test and were 0.4 or less in valgus stress test throughout ROM. They stayed constant after 90° of ROM. This could be due to the different stiffness of the medial and lateral collateral ligament, which are stressed during varus–valgus stress test. During both tests, the laxity increased progressively with flexion angle. Evidently, the geometry knee reproduces more lateral laxity at higher flexion as in the anatomic situation. We revealed that using a unique insert sensor, the soft tissue balancing should aim for anatomical contact forces, which will result in a laxity close to normal in BCS TKA. While, in varus stress test, medial TFCF rose sharply between 30° and 60°. Therefore, it is suggested that BCS TKA potentially reduces the external rotation of the femur between 30° and 60° flexion.
In the current study, we found the correlation between intraoperative medial TFCF increase at 60° flexion in neutral position and physical function (Table 2). In addition, there was correlation between medial TFCF increase at 30° and 140° flexion in valgus stress test and symptoms in 2011 KSS (Table 4). These results suggest that intraoperative medial stability in mid and deep flexion position is important for function and symptoms, therefore, surgeons should not release medial soft tissue to achieve better clinical outcomes after BCR TKA.
Correlation coefficients between medial and lateral TFCF differences throughout range of motion in neutral position and patient reports outcome measure at 6 months after TKA.

med-lat TFCF: medial and lateral tibiofemoral compressive force difference; KSS: Knee Society Scores; WOMAC: Western Ontario and McMaster Universities scores.
a Correlations are statistically significant (p < 0.05).
Other interesting findings of the present study are that medial TFCF increase at 120° flexion in varus stress test was correlated with reducing stiffness (Table 3). The results suggest that greater lateral laxity at 120° flexion guides a rollback and translation of femoral component and reduces stiffness.
Correlation coefficients between medial and lateral TFCF differences throughout range of motion in varus stress test and patient-reported outcome measure at 6 months after TKA.

med-lat TFCF: medial and lateral tibiofemoral compressive force difference; KSS: Knee Society Scores; WOMAC: Western Ontario and McMaster Universities scores.
a Correlations are statistically significant (p < 0.05).
Correlation coefficients between medial and lateral TFCF differences throughout range of motion in valgus stress test and patient-reported outcome measure at 6 months after TKA.

med-lat TFCF: medial and lateral tibiofemoral compressive force difference; KSS: Knee Society Scores; WOMAC: Western Ontario and McMaster Universities scores.
a Correlations are statistically significant (p < 0.05).
Medial TFCF decrease at 140° flexion in varus stress test was correlated with improving physical function (Table 3). These results suggest that lateral TFCF increase at deep flexion guides bicondylar rollback, as a result, it improved daily physical activity.
Only two knees were engaged between anterior cam and post in posterior inclination of tibia with 6° and 8°. We should make the posterior inclination of tibia more than 6°, depending on the patient’s physiological posterior inclination of tibia. A small number of cases were assessed, therefore, further studies should be directed at assessing posterior inclination of tibia.
Conversely, previous work has defined adequate knee balance using Triathlon knee (posteriorcruciate ligament [PCL] retaining or sacrificing TKA (Stryker, Mahwah, New Jersey, USA)) with VERASENSE system as load difference of 15 pounds between the medial and lateral compartments. A good balance in flexion was obtained, where the femoral component meets at one-third posterior to the center of tibial component. 15 Postoperatively, balanced patients (mediolateral intercompartmental loading difference <15 pounds at 10°, 45°, and 90° of flexion) showed greater improvement in mean values than unbalanced patients in both 2011 KSS and WOMAC scores. 15 The unbalanced group reported medial TFCF of 100 pounds or higher due to the malrotation position of femoral and tibial components, while cases of malrotation alignment were excluded in this study. 15 While Elmallah et al. 23 reported that the sensor group using Triathlon knee (cruciate-retaining TKA (Stryker)) with VERASENSE system had lower mean differences in intercompartment loading at 10°, 45°, and 90° compared to manually balanced patients.
Salvadore et al., 24 similar to this study, revealed that using fresh-frozen lower extremity specimens, the soft tissue balancing should aim for anatomical contact forces, which will result in a laxity close to normal in BCS TKA. The computer simulation study has shown that anterior contact between the anterior aspect of the tibial post- and femoral component was observed if the posterior tibial slope was 6° or more. 25 Unlike VERASENSE system, compressive force of anterior cam and post can be measured in the current study and cases with less than 6° of the posterior inclination of tibia did not engage with anterior cam and post, therefore, we should aim for the patient’s physiological posterior inclination of tibia to substitute for ACL.
Meneghini et al. 26 showed that medial and lateral TFCF related to the PROMs obtained at 4 months from TKA and confirmed that mean medial TFCF (70.7 pounds) was higher than mean lateral TFCF (44.0 pounds) during trial sensor testing at 0°, 45°, and 90° of flexion. In conclusion, the authors revealed that PROMs were unrelated to mediolateral balance of the knee, as determined by medial and lateral TFCF. Meere et al. 27 reported that the FR was 0.52% ± 0.14 throughout ROM using Triathlon knee (PCL retaining or sacrificing TKA (Stryker)) with VERASENSE system, while the FR was 0.44% ± 0.22 in the current study. This is because the lateral TFCF was higher than medial TFCF from 10° to 60° of flexion.
In the current study, the lateral load decreased as the knee flexed, while the opposite was the case for the medial site. The FR (medial TFCF/ medial + lateral TFCF) started with a mean of 0.35 at full extension and then slowly increased until reaching 0.66 at 140° of flexion. These load levels resemble the distribution observed for intact knees, as demonstrated by Verstraete et al. 18 This resemblance is not surprising, given the anatomical design features with joint line obliquity of the considered implant system. Conversely, Gustke 16 described that a ratio of 0.5% indicates equal lateral and medial forces and this target has traditionally been the target for nonanatomical total knee designs.
BCS prosthesis guided screw home movement at flexion angle of 10° and has an asymmetrical insert thickness to recreate joint obliquity like a healthy knee and induces medial pivot pattern during early flexion or bicondylar rollback beyond mid-flexion. 28
The present study has some limitations. The first limitation of this study is that only varus knees were included, so the results of this study cannot be directly applied to valgus knees.
The second limitation is that only a small number of cases were assessed, but there were strong correlations on multiple regression analyses. The third limitation is that the data were obtained for BCS TKA by novel insert sensor; therefore, the results may differ from data obtained for other TKA design. The fourth limitation is that KSS and WOMAC scores were obtained only 6 months after TKA.
Long-term investigations of the change in PROMs are necessary. The fifth limitation of this study is that intraoperative measurement of medial and lateral TFCF was not true physiological loads, as reported by D’ Lima et al. 29 and Mizu-Uchi et al. 30 The sixth limitation of this study is that the current study is a pilot series, and the stresses across the joint are not applied intraoperatively. In the future, if a normal value of TFCF to improve PROM is known, a new surgical technique will be developed. The seventh limitation of this study is that a unique insert sensor (size 3.4 and thickness 9 mm) in right knee was developed for this study. The last limitation of this study is that one observer performed all the measurements, and therefore, this study has no interobserver variability of measurements.
Novel insert sensor in the present study may have an advantage of providing objective and quantifiable feedback when performing appropriate soft tissue releases and further studies should be directed at assessing whether this new technology really improves soft tissue balance.
Conclusions
BCS TKA (substituting ACL) reproduces the coronal laxity of the intact knee, demonstrating the increased medial TFCF and the decreased lateral TFCF throughout ROM using an insert sensor developed independently. But BCS TKA reduces the external rotation of the femur from 30° to 60° flexion. To achieve the intraoperative medial stability and substitute for ACL, surgeons should not release medial soft tissue to accomplish better clinical outcomes and are suggested to aim for the patient’s physiological posterior inclination of tibia.
Footnotes
Acknowledgments
The authors thank Hiroaki Suzuki for their assistance in this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.