
Abstract
Background:
The treatment of large osteochondral lesions of the talus (OLTs) is challenging due to the poor intrinsic reparative capability of the damaged articular cartilage. Autologous transfer of bone and periosteum has been used successfully in the treatment of large defects in animals, and therefore it was believed that this technique might show similar results in humans. The purpose of this study was to assess the outcome of an innovative technique for autologous transplantation of cancellous tibial graft with periosteal transfer in large OLTs.
Methods:
Forty-one patients (22 females, 19 males), with a mean age of 34.9 years (range, 18-72 years), with a large OLT (>200 mm2) were treated with autologous bone graft and periosteum transfer. OLTs averaging 310 mm2 were identified on a preoperative computed tomography scan. The procedure consisted of malleolar osteotomy, curettage of sclerotic bone, autologous bone graft from the proximal tibia, and transfixion of periosteum over the graft. Outcome measures, including the pain visual analog scale (VAS), ankle range of motion (ROM), American Orthopaedic Foot & Ankle Society (AOFAS) score, and Foot & Ankle Disability Index (FADI), were compared between preoperative and 1 and 2 years following surgery.
Results:
There were significant improvements in VAS pain score from 7.7 before surgery to 1.1 at 1 year after surgery and 0.4 at 2 years or more after surgery. The AOFAS and FADI scores were also significantly improved from 40.3 and 53.3 preoperatively to 95 and 93.2 postoperatively at 1 year and 95 and 93.2 at 2 or more years postoperatively, respectively. Postoperative complications included 2 patients who required removal of medial malleolar osteotomy tension bands due to symptomatic hardware. There were no nonunions or malunions of the osteotomies and no donor site complications.
Conclusion:
Autologous bone graft and periosteum transfer was an effective treatment for large OLTs leading to significant decreases in pain and improvement in functional scores at more than 2 years after surgery.
Level of Evidence:
Level IV, retrospective case series.
While there is general agreement on the treatment of symptomatic small contained osteochondral lesions of the talus (OLTs) with arthroscopic curettage and bone marrow stimulation, there is no consensus on the best treatment for focal and contained large OLTs (>200 mm2). On one hand, the injured articular cartilage shows poor intrinsic reparative ability, and on the other hand, current techniques do not offer high success rates at long-term follow-up. 4,13,14,18,24
We have developed a technique for treating large contained OLTs that takes advantage of the intrinsic chondral regenerative abilities of the periosteum and cancellous autograft. The purpose of this study was to evaluate the radiographic and clinical outcomes of autologous cancellous tibial bone and periosteum transfer for the treatment of large OLTs.
Methods
We retrospectively reviewed the medical records and radiographs of 41 adult patients (mean age, 34.9 years; range, 18-72 years; 22 females and 19 males; Table 1) with a symptomatic OLT measuring >200 mm2 on computed tomography (CT) scan who underwent periosteal and cancellous bone grafting from January 2010 to January 2017. Patients were excluded from the study if they had (a) ankle instability (clinically anteroposterior drawer and radiographically >10 degrees of talar tilt or >10 mm of anterior displacement), (b) active infection, (c) restricted foot and ankle blood supply (>50% lower limb arterial stenosis on ultrasound), and (d) any inclination in ankle axis >5 degrees or (e) contraindications to the procedure, including bipolar lesions (cysts in talus medial and lateral simultaneously or talar and tibia cysts simultaneously) or early osteoarthritic changes (tibial or talus anterior or posterior osteophytes or sclerosis of the joint).
Patients’ Demographics Based on Age and Sex.

The OLTs were located laterally in 3 patients and posteromedially in 38. Bilateral OLT occurred in 7.3% (3/41) of our patients (Figure 1). The defects as measured by CT 7,14 were sized 200 to 220 mm2 in 31 patients and 220 to 240 mm2 in 10 patients (Figure 2).

Radiographs of talar osteochondral lesions of the talus and adjacent subchondral cysts.

(A) Axial ankle magnetic resonance imaging (MRI) of posteromedial talar large cyst. (B) Sagittal ankle MRI of posterior talar cyst. (C) Coronal ankle MRI of posteromedial talar large cyst. (D, E) Sagittal ankle computed tomography (CT) of anterior talar cyst. (F) Coronal ankle CT of posteromedial large talar cyst.
Outcome Measures
Clinical evaluation was performed preoperatively and at 1 and 2 years postoperatively. The outcome measures included the pain visual analog scale (VAS), ankle range of motion (ROM) using a goniometer, American Orthopaedic Foot & Ankle Society (AOFAS) ankle hindfoot score, and a Foot & Ankle Disability Index (FADI) score. An AOFAS score of over 90 was defined as excellent, 84 to 90 as good, 65 to 83 as fair, and less than 65 as poor. The patients were followed up for a mean of 2.4 years (range, 2-3 years). The first 20 cases underwent second-look arthroscopy to evaluate chondral coverage at 9 to 12 months after the initial operation.
Statistical Analysis
Statistical analysis was performed using SPSS 24.0 software (SPSS, Inc, an IBM Company, Chicago, IL) was used for statistical analysis. Friedman’s analysis of variance (ANOVA) and Wilcoxon signed-rank test were conducted for the evaluation of changes in AOFAS, FADI, and VAS score and ROM parameters. A P value of less than .05 was considered statistically significant.
Ethical Approval
The local ethics committee of the Central Clinic of Athens (Orthopaedic Research Institute for Education and Training) approved the study, which was carried out according to the World Medical Association Declaration of Helsinki. Institutional review board approval and written consent from all patients were obtained. 16
Surgical Technique
An 8- to 10-cm curvilinear medial or lateral incision (Figure 3A,B) was made over the medial or lateral malleolus for medial or lateral OLT, respectively. 29,31 For the medial OLTs (38 cases), a medial malleolus chevron osteotomy was performed 2,3,11,43 approximately 5 to 6 cm above the tip of the medial malleolus (Figures 4 and 5). 43 For the lateral OLTs (3 cases), a chevron osteotomy was performed approximately 3 to 5 cm above the tip of the lateral malleolus and the osteotomy was eventually stabilized with anatomic distal fibula plates as well as cortical and cancellous screws.

(A) The 8- to 10-cm standard curvilinear medial incision over the medial malleolus for medial osteochondral lesions of the talus. (B) The periosteum is carefully opened longitudinally and detached from the bone. (C) The posterior tibialis tendon and the adjacent neurovascular bundle are carefully located and protected.

The apex of the chevron cut is identified with fluoroscopy assistance (subchondral plate at the malleolar colliculus).

A medial malleolar chevron osteotomy is performed approximately 5 cm above the tip of medial malleolus. (A) Oscillating saw. (B) Osteotome. (C) The osteotomy is open.
Following the osteotomy, the necrotic or sclerotic bone was curetted and the base of the lesion was then microfractured (Figure 6). A 4- to 5-cm longitudinal incision was then made on the anteromedial tibial tuberosity. The periosteum graft was harvested sharply. We avoided using electrocautery to prevent thermal necrosis. A template of the defect was used to guide the size and shape of the periosteal resection, which was 1 to 2 mm larger than the actual defect. A cortical window was then opened and cancellous bone was transferred into the talar defect and impacted layers (Figures 6D,E, 7, and 8). The periosteal graft was placed over the defect with the cambium side facing the autograft bone. It was then sutured with 6-0 Vicryl sutures. Fibrin glue sealed the periosteal interface (Figures 6F and 8). The procedure was concluded with reduction and internal fixation of the medial malleolus osteotomy fragment with a tension band technique (Figure 9).

(A) The osteochondral plug of the cyst is removed. (B) The sclerotic bone is excised and curetted to the bottom of the lesion until reaching viable bleeding bone. (C) The wall of the cyst and the base of the lesion are abraded and curetted down to viable subchondral bone. (D) A small longitudinal (4 to 5 cm) incision is performed on the proximal tibia metaphysis. With use of a curved osteotome, a cortical window has been opened (2 × 3 cm). (E) Cancellous bone is taken as an autograft and is transferred into the talus curetted defect (impaction graft technique). (F) The periosteum is sutured over the cancellous autografted defect with 6-0 Vicryl sutures and the knots are tied over the graft (usually 6-8 knots).

The incision in the upper anteromedial part of the tibia where cancellous bone and periosteum grafts were taken.

Periosteum transfer in talus large cyst (final view before repairing the osteotomy).

Postoperative radiographs. The osteotomy reduction was performed with a tension band technique in the medial malleolus and plate and screws in the lateral malleolus.
The ankle was bandaged and splinted for 2 weeks. The sutures were removed 15 to 20 days following the operation, and a removable walking boot was applied and passive ankle ROM was permitted. The patient remained nonweightbearing for 1 month followed by partial weightbearing for 4 to 6 weeks. At weeks 6 to 8, full weightbearing began when the ankle X-rays showed sufficient healing of the osteotomy.
Results
The VAS scores displayed a significant statistical improvement from a preoperative mean of 7.7 (95% confidence interval [CI], 7.4-8.0) to 1.1 at 1 year postoperatively (95% CI, 1.0-1.3) and to 0.4 at 2 years postoperatively (95% CI, 0.2-0.6) (P < .001) (Table 2). In addition, improvement in ankle ROM was found with preoperative ankle ROM averaging 24.5 degrees in total to a 1-year postoperative ankle ROM averaging 58.3 degrees (P < .001) (Table 3). The mean AOFAS score increased from 40.3 preoperatively to a 1-year postoperative mean score of 95, with the 2-year postoperative mean score being unchanged at 95 (P < .001). The mean FADI score increased from 53.3 preoperatively to a 1-year postoperative mean score of 93.2 and a 2-year postoperative mean score of 93.3 (P < .001). There was no difference in AOFAS and FADI scores between years 1 and 2 postoperatively (Tables 4 and 5). Based on the patient’s age, the correlation of AOFAS and FADI both pre- and postoperatively was statistically significant, and the pre-AOFAS score was lower in older patients as opposed to younger ones (P < .001).
VAS Score Results and Statistics.

Abbreviation: VAS, visual analog scale.
a Friedman’s analysis of variance.
b Wilcoxon signed-rank test.
ROM Results and Statistics.

Abbreviation: ROM, range of motion.
a Wilcoxon signed-rank test.
AOFAS Score Results and Statistics.

Abbreviation: AOFAS, American Orthopaedic Foot & Ankle Society.
a Friedman’s analysis of variance.
b Wilcoxon signed-rank test.
FADI Score Results and Statistics.
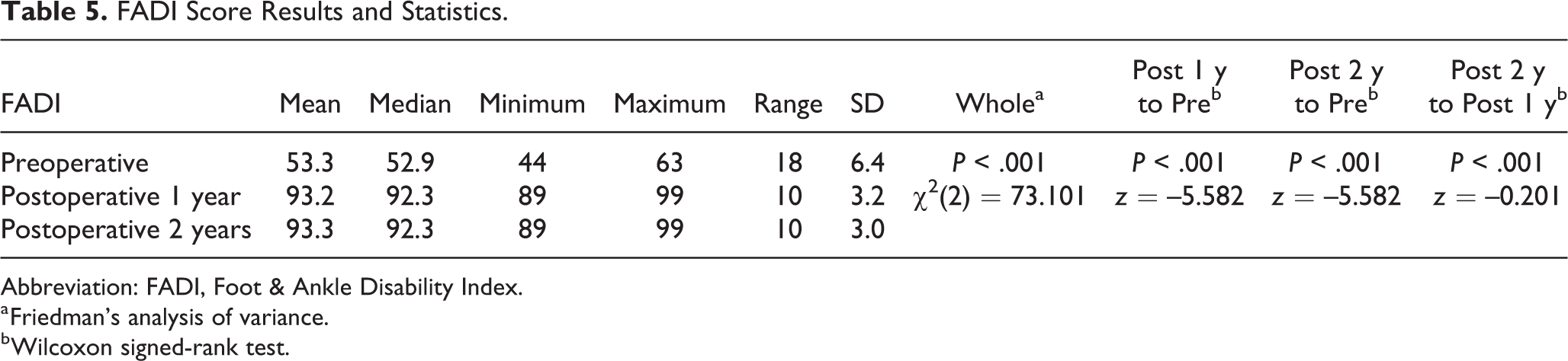
Abbreviation: FADI, Foot & Ankle Disability Index.
a Friedman’s analysis of variance.
b Wilcoxon signed-rank test.
At the time of final follow-up, 33 patients (80.5%) reported excellent results and 8 (19.5%) reported good results based on AOFAS and FADI scores. There were no fair or poor results. Thirty-five patients (85.4%) reported being able to perform physical activities at the same level as prior to the onset of their symptoms, whereas 6 patients (14.6%) reported being able to perform a lower level of physical activity compared to before the onset of their symptoms. In addition, at the final postoperative follow-up, 4 of 41 patients (9.7%) demonstrated an alteration in the normal shape of the talus on ankle radiographs; however, these patients demonstrated minimal clinical symptoms and very good cartilage coverage in the postoperative arthroscopic monitoring.
In the first 22 cases, second-look arthroscopic monitoring was performed between 9 and 12 months following the initial operation to evaluate if a residual cartilage defect existed (Figure 10). The Orthopaedic Research Institute for Education and Training (Institutional Review Board) approved the study, whereas patients’ written consent was also attained prior to the initial operation. In the remaining 19 cases, we did not perform ankle arthroscopy since these patients had very good to excellent results without complications.

Arthroscopic postoperative images of our cases evaluating the formation of fibrocartilage 6 months postsurgery.
In the second-look arthroscopy group, there were no residual cystic or cartilage defects observed. These patients did have limited adhesions that were debrided. There was evidence of alteration of the talar shape seen on anteroposterior and lateral radiographs in 2 patients undergoing second-look arthroscopy; however, these did not appear to show any abnormalities of the cartilage intraoperatively. Of these 22 cases, 18 displayed regenerated cartilage with a uniform thickness and intact surface that appeared similar to normal cartilage and was difficult to distinguish from the adjacent unaffected normal cartilage. In 4 of the 22 cases, we found an intact surface with some softening of the overlying cartilage, but this was devoid of fragmentation or fissuring.
For all patients, postoperative magnetic resonance imaging (MRI) was not performed due to the presence of metallic implants for fixation of the osteotomy. In all 22 cases that were arthroscopically monitored, a layer of nearly fully restored cartilage was detected (Figure 10).
Postoperative complications included 2 patients who required removal of medial malleolar osteotomy tension bands due to symptomatic hardware. There were no nonunions or malunions of the osteotomies and no donor site complications.
Discussion
There has been an increase in large talar OLTs observed in the past decade, with an increased incidence among recreational and professional athletes in the setting of both acute ankle sprains and ankle fractures. 1,13,27,33,43 Surgical treatment options for symptomatic OLTs include surgical excision of the lesion combined with curettage and drilling or microfracturing (bone marrow stimulation), placement of an autogenous (cancellous) bone graft, osteochondral transplantation (osteochondral autograft transfer system [OATS]), 22,30,35,38,40,45,46 and autologous chondrocyte implantation (ACI). 5,13,14,19,23,44 The latter techniques focus on replacement and regeneration of hyaline cartilage. 17,19,21,46 Our proposed surgical technique with cancellous bone grafting with periosteum is also a viable technique performed in large talar cystic defects, offering very good to excellent results. Our technique aimed to restore the articular surface through the use of repair tissue similar to native cartilage, leading to symptomatic relief.
For larger lesions, OATS, ACI, and osteochondral allografts are the main surgical treatment options presently. 5,15,21,22,23,30,45 The reparative procedures, including bone marrow stimulation, are generally best indicated in smaller OLTs with a surface area <150 mm and are less adequate for large defects. 2,3,10,27 We recognize that the benefits of OATS and ACI are that these are arthroscopic surgeries while our proposed technique is an open procedure. However, in our study, there was no evidence of complications related to open procedures, including any evidence of stiffness likely due to the early rehabilitation protocol. 42
Yamashita et al 45 was the initial group to implement the OATS technique, and they showed good clinical outcomes in talus OLT treatment. Subsequent studies have shown excellent results with the OATS procedure; however, in the case of large defects, the need for a larger donor site graft has proven somewhat invasive and can lead to donor site complications in the knee. 12 Matsusue et al 30 reported on mosaicplasty, which involved using multiple graft transplantations for chondral lesions in the knee, which reduced donor site complications. Hangody et al 22 reported on their experience with mosaicplasty in the ankle. They performed the mosaicplasty on 36 patients with an OLT of the talus and had very good clinical outcomes (94%) for most patients. No patients experienced complications arising from the donor sites. Similarly, in our technique, there was no significant donor site morbidity.
Alternatively, allograft transplantation is an option as it allows for a large surface OCL to be replaced with a single unit of viable articular cartilage and subchondral bone from a donor that is matched to surface curvature, shape, and size. 35,38,40,46 However, this technique has limited supportive evidence for treatment of large-volume cystic lesions or salvage procedures. 5,10,26,42 It was first reported in knee surgeries and later applied in the treatment of talus OLTs. 28 Gross et al 20 reported on their experience in which they treated 9 cases of OLTs of the talus with osteochondral allograft transplantation. They reported that satisfactory outcome was observed in only 6 of the cases (67%). Other studies have shown evidence of radiolucencies and edema around allografts. 6,8 The main benefits of using allografts consists of bypassing the need for a donor site and the use of a singular sizable graft, which in turn minimizes the formation of fibrocartilage between graft bones (the main disadvantage of mosaicplasty). 42 One important limitation is that the survival of posttransplantation cells is low compared to autologous graft and periosteum transplantation method. The survival of cells is also lower in frozen allografts compared to fresh allografts. 9 Therefore, in large talus cysts, the possibility of failure with allografts is higher vs our proposed autologous transfers. Another limitation is a possible immunological response, which is greater in fresh allografts compared to frozen allografts. 26,42
It is important to acknowledge that although the former clinical studies have shown good to excellent short- and mid-term results, it is of concern that the methodological quality of previous literature is lacking. 18 In addition, although there is much evidence based on results for ACI in the knee, 32,39,44 literature on the evaluation of efficiency, safety, and usefulness for the ankle is minimal. In a current meta-analysis of ACI in ankle chondral and osteochondral defects, overall clinical outcomes presented a success rate of 89.9%. Further evaluation of 16 subsequent studies demonstrated success rates between 50% and 100% according to the individual scoring system. 37 An important finding of this meta-analysis is the significant lack of evidence concerning the use of ACI on the talus. 34,36 Even though there are encouraging results displaying the efficiency of this treatment, no controlled studies are available. 25,35,38,40,41,46
Furthermore, we believe the proposed procedure in this study is an excellent alternative for large talus cysts (>200 mm2), and although it is an open surgery requiring a malleolar osteotomy, it has many benefits compared to other open techniques. Specifically, (1) it is a single-stage surgery (vs ACI, which is a 2-stage surgery), (2) there were no donor site complications (especially in large lesions) as there was no need to violate additional joints, (3) there was no disease transmission risk as autograft was used vs allografts, and (4) there was limited risk for complications (malunion, nonunion, infection) or failure (0% in 41 cases). Finally, it is important to mention the low cost of this procedure. It is a single-stage surgery with bone autograft and periosteum transfer. Aside from the sutures, the only cost is the osteosynthesis materials (K-W, wire, plate, screws) for malleolar fixation. In our series, there were no failures or poor/fair results. All 41 patients improved significantly and returned to their day-to-day activities. The main limitations of our study are that the number of cases performed until recently is relatively small (41 total) and the short-term follow-up with a mean of 2.4 years (range, 2-3 years).
There are some technical considerations when implementing this technique. This is an open technique requiring a malleolar osteotomy, but for an orthopedic surgeon with experience in ankle fractures, it is feasible to perform an accurate malleolar osteotomy under fluoroscopy without damage to the adjacent articular surfaces. Care should be taken when triangulating the location for malleolar osteotomy as an incorrect position may result in difficulty in access for graft transfer and visualization for periosteal suturing. Furthermore, periosteal suturing will often require microsurgical loupes. In cases of difficulty with periosteal suturing, fibrin glue may be used as an alternative to suturing.
Conclusion
There have been few studies of large OLTs in the talus. We report on treatment of large talar OLTs with transplant of autologous cancellous graft and periosteal transfer with promising short-term outcomes. Future clinical studies on this technique may include long-term outcomes as well as comparative studies to alternative treatment options.
Supplemental Material
Supplemental Material, FAO874039-ICMJE - Large Osteochondral Lesions of the Talus Treated With Autologous Bone Graft and Periosteum Transfer
Supplemental Material, FAO874039-ICMJE for Large Osteochondral Lesions of the Talus Treated With Autologous Bone Graft and Periosteum Transfer by Dimitrios Nikolopoulos, Neoptolemos Sergides, George Safos, Konstantinos Moustakas, Petros Safos and Andreas Moutsios-Rentzos in Foot & Ankle Orthopaedics
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.