
Abstract
Background:
Congenital kyphosis results from the failed formation of the vertebrae during the embryonic period and may be associated with cardiac, urogenital, or spinal cord anomalies. Surgical treatment is the best choice through anterior, posterior, or both approaches.
Objectives:
This study aims to evaluate the effect of posterior gradual correction using the “in situ” bender to correct severe thoracolumbar congenital kyphosis with or without osteotomy or excision of the vertebra.
Methods:
Twenty-five patients with an age range of 2–23 (mean ± SD = 12.58 ± 6.03) years with severe thoracolumbar kyphosis were treated surgically at our institution between 2004 and 2013. Pedicle screwing, osteotomy, and gradual “in situ” bending through the single posterior approach were the choices of treatment. Cobb’s angle, patient’s height, and SRS-22r were used to evaluate the patients preoperatively and postoperatively. Follow-up periods were 35–136 months.
Result:
Cobb’s angle pre-surgery range was 35–180 (81.48 ± 39.1) degrees improved post-surgery to 0–45 (21.72 ± 13.47) degrees (p-value <0.0001). The range of patients’ standing height pre-surgery was 79–170 (142.42 ± 24.85) centimeters increased after surgery to 81–175 (147.76 ± 26.33) centimeters (p-value <0.0001). SRS-22r pre-surgery range was between 2.12 and 3.904 (3.2 ± 0.77) and improved post-surgery to 4.16 and 4.96 (4.59 ± 0.29) (p-value = 0.046).
Conclusion:
Gradual correction with the “in situ” bender with or without osteotomy through the single posterior approach can give satisfying clinical (patients’ standing height and SRS-22r scores) and radiological (Cobb’s angle) results to treat severe congenital thoracolumbar kyphosis.
Keywords
Introduction
Congenital kyphosis is a spinal deformity, which results from failed anterior formation or segmentation of the vertebrae in the sagittal plane during the early embryonic period. 1 –3 The cause of these defects is not clear and believed to be a vascularization disorder as studies on animals suggested. 3,4 Renal and cardiac congenital anomalies may be associated with spinal deformities as they form in the same period. 3 McMaster classified these defects into three types: type 1 (anterior spinal column defect, which results in posterior hemivertebra, rapid progressive kyphosis, and associated with neurological deficit and paraplegia), type II (anterior failure of segmentation, which leads to progressive kyphosis without neurological deficit), and type III (a combination of formation and segmentation failures, which is usually seen at the level of T10–L1 vertebrae and may progress faster than type II). 4,5 The cardiopulmonary function may be affected in progressive and severe cases. 5
Pure congenital thoracolumbar kyphosis (not associated with scoliosis) is a rare condition. The number of patients in most previous studies ranged between 9 and 24. 1,3,6 –9
No rule exists for conservative treatment with cast or braces. 3,5,10,11 Surgical treatment is the best choice for these cases considering the patients’ age range, types, sizes of the deformity, and their neurological statuses. 12 Many surgical procedures were applied through anterior, posterior, or combined approaches with no clear indication which one is the best to correct the deformity. 13 –18
Recently, with the development of surgical techniques and instrumentations, the posterior approach became the preferred technique to perform pedicle subtraction osteotomy (PSO), posterior vertebral column resection (PVCR), or vertebral column decancellation. 19 –22
This retrospective study aims to evaluate the effect of posterior gradual correction of severe congenital thoracolumbar kyphosis using pedicle screws and “in situ” bender with or without osteotomy or excision of the vertebra (PVCR or hemivertebra) at our institution in the interval between January 2004 and December 2013.
Methods
Twenty-five patients with an age range from 2 to 23 (mean ± SD = 12.58 ± 6.03) were operated between January 2004 and December 2013 at our institution for thoracolumbar congenital kyphosis. Institutional Review Board approval was obtained.
Other causes, that is, infections, syndromes, neurological causes, post-surgery, tumors, or fractures of kyphosis and kyphoscoliosis, were excluded. Clinical data (including history and physical examination) were gathered by a multidisciplinary team of orthopedic surgeons, pediatricians, dysmorphologists, and neurosurgeons. Radiological evaluation, including standing long X-ray film showing the whole spine in anteroposterior and lateral projections, spine magnetic resonance image, and computed tomography (CT) scan was performed.
Genitourinary and cardiac congenital malformations were investigated. Results of the pulmonary function test were collected among the results of other laboratory tests. We also recorded the standing height in centimeters, kyphosis magnitude using Cobb’s angle, apical level, and kyphosis subtype using the CT scan (Table 1). All kyphotic curves were rigid, especially in older patients and patients with high-degree curves.
Demography of patients and pathology and treatment.
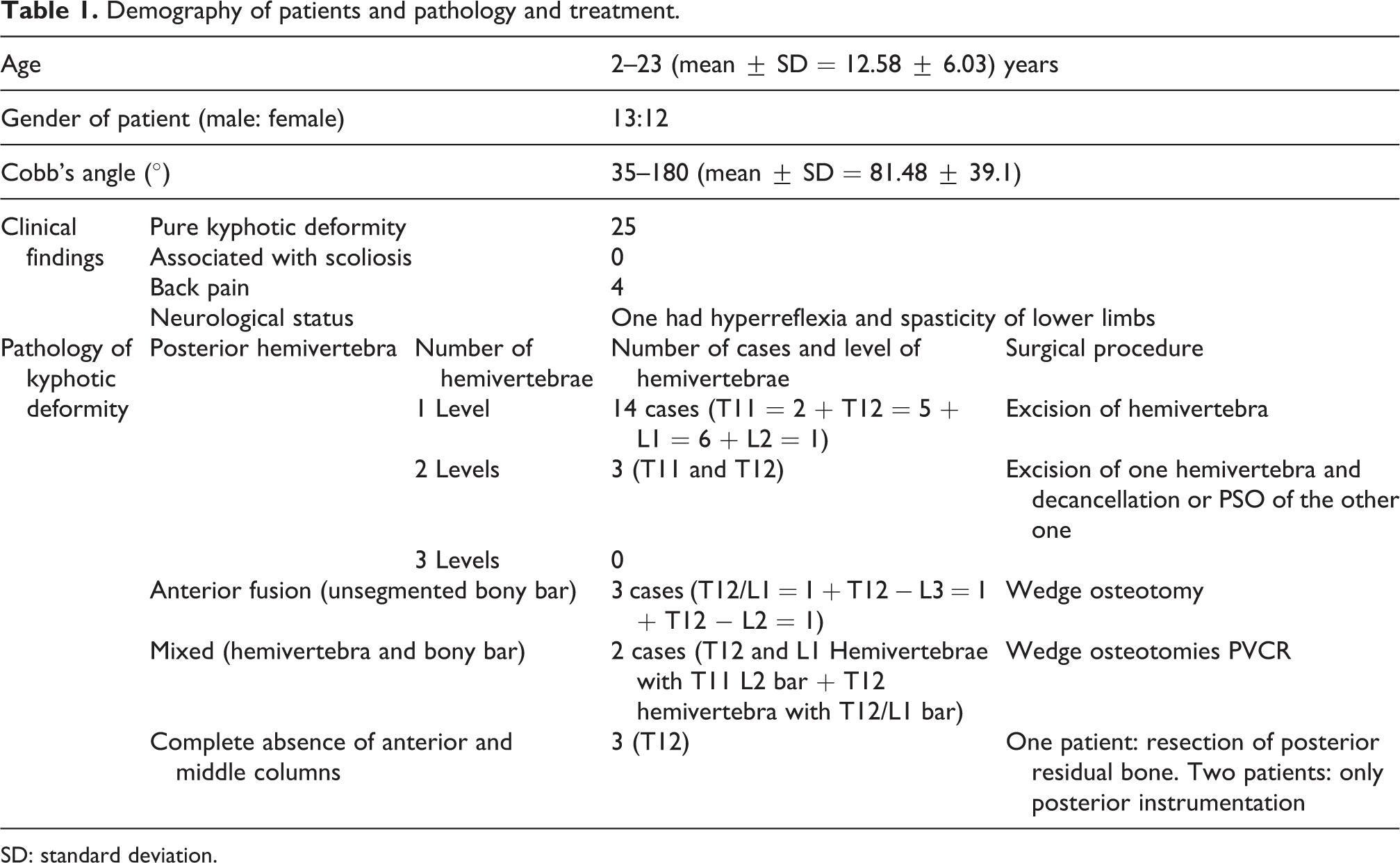
SD: standard deviation.
The SRS-22r questionnaire from the Scoliosis Research Society was completed by each patient twice: before surgery and at the final follow-up. The SRS-22r questionnaire consists of 22 questions: 5 for pain, 5 for function, 5 for self-image, 5 for mental health, and 22 for satisfaction/dissatisfaction with treatment. The first 20 questions were used pre-surgery and post-surgery, whereas the last 2 questions were used only at the last follow-up.
All the patients were operated through the single posterior approach, pedicle screw fixation with or without osteotomy [osteotomy was not indicated in three patients (one was an adult and the other two were less than 5-year-old)]. Short fixation segment (mainly two vertebrae above and two below the apex) with or without; hemivertebra excision, PSO, or decancellation were used for the younger patients before puberty. Decancellation (egg-shell osteotomy) was done through the posterior approach by excising the posterior neural arch, facet joints, and pedicles. After that, the vertebral body cancellous bone was excised using the curette and pituitary forceps, while the posterior cortex was pushed anteriorly to prevent spinal canal encroachment and spinal cord or cauda equina compression. Long fixation and osteotomy (excision of hemivertebra, PSO, wedge osteotomy, or excision of residual posterior bone) were performed for the adolescents and adult patients. In one case (Cobb’s angle = 155°), we needed to insert a body cage after PVCR. In three cases, we did excision of hemivertebra and decancellation (Table 1). After that, two rods were bent to give them the corrective sagittal shape of the spine and they were applied to the heads of the screws. The shape of the bent rod provided partial correction for the deformity, while the residual kyphosis was corrected gradually using the “in situ” bender.
Gradual correction technique was done over 2–3 h by applying the “in situ” bender on the rods near the apex of kyphosis. Small amount of corrective force was applied on the rods in 1-min intervals with 5–10 min breaks. That allowed relaxation of the anterior abdominal wall muscles and soft tissues and prevented the pull-out of the screws that can be caused by the excessive stress on them. This manoeuvre was repeated several times until satisfactory correction was achieved. Forty percent of patients who were operated before 2008 were monitored during the surgery by the wake-up test because neuromonitoring technology was not available at our hospital. Since 2008, we monitored all the patients during surgery, in addition to the wake-up test.
Postoperatively, the patients were transferred to the general medical floor. On the next day, they were ambulated as tolerated. They were X-rayed on the third postoperative day and discharged on the fifth day. Only four of the early age (less than 5-year-old) patients were worn the Boston brace. The SRS-22r questionnaires were completed by all the patients twice (except patients who were less than 5-year-old, their parents did that): before surgery and at the final follow-up. Photographs for each patient were taken in the preoperative period and the last follow-up after signing informed consent.
Statistical analysis
In this study, we analyzed the results using SPSS version 21. Paired sample t-test was used to compare the means of pre- and post-treatment values (SRS-22r) for the same group of patients to compare the significant differences in the average heights before and after surgery also to calculate the SD for both groups’ means. The results considered to be significant if the p-value is <0.05. Using SPSS again (frequencies), the descriptive statistics of the study (such as self-image, pain, function pre- and post-treatment, etc.) were determined.
Results
Twenty-five patients met our inclusion criteria between January 2004 and December 2013; 13 males and 12 females, the age range was from 2 to 23 (12.58 ± 6.03) years. The follow-up period ranged between 35 and 136 (75.32 ± 31.15) months. Seventeen patients had (≥1) posterior hemivertebra and three patients had a complete absence of anterior and middle columns (Table 1). Pre-surgery Cobb’s angle ranged between 35° and 180° (81.48° ± 39.1°) improved to 0–45°(21.72° ± 13.47°) at the final post-surgical evaluation. The improvement range was 5–135° (59.2° ± 32.69°); p-value <0.0001 (Figures 1 and 2).

Lateral X-ray of whole spine showed severe kyphosis of the thoracolumbar (180°) area with compensatory thoracic and lumbar lordosis.

Lateral X-ray of the whole spine of the same patient showed post-surgical improvement of the curves and restoration of the sagittal balance.
The range of patients’ pre-surgery heights was 79–170 (142.42 ± 24.85) centimeters, which improved to 81–175 (147.76 ± 26.33) cm post-surgery. The improvement range was 0–17 (5.28 ± 4.208) cm; p-value <0.0001 (Table 2).
Cobb’s angle and patients’ height pre and post-surgery.

SD: standard deviation.
All patients were operated with a single-stage except three of them, who needed staged procedure over 2–3 stages because they had very tight anterior soft tissues. Operative time range was 4 and 9.5 (4.98 ± 1.46) hours and the mean blood loss range was 450–1800 (1057.2 ± 344.5) ml. The wake-up test during the surgery was normal for all patients who were operated before 2008. After a full recovery, two patients developed complete paraplegia: one improved completely and directly after emergency revision surgery and evacuation of a small hematoma, while the other improved gradually over 2 years. Two patients developed junctional kyphosis so that the instrumentation was extended one level above. Three patients had a metal breakdown after 6 months of surgery and another one needed changing of the screws as they became small for pedicles with the growth of the patient (Figure 3). None of them had wound infection. One had a mild pulmonary embolism (proved with the spiral CT scan).

Lateral view X-ray of the whole spine shows broken rode.
The SRS-22r score range was better after the surgery than before it, especially self-image, which improved from 1–3.4 (2.12 ± 0.603) to 3.8–5 (4.608 ± 0.449). A mean value of each item in the score was calculated for each patient, then the mean value of all patients was calculated. The mean values of the score were taken at the final follow-up and compared with that of pre-surgery (Figure 4). SRS-22r pre-surgery range was 2.12 and 3.904 (3.2 ± 0.77166) with the least value was that for self-image [the range was 1 and 3.2 (2.12 ± 0.603)], and the best value was that for pain [the range was 2 and 4.8 (3.904 ± 0.788)].
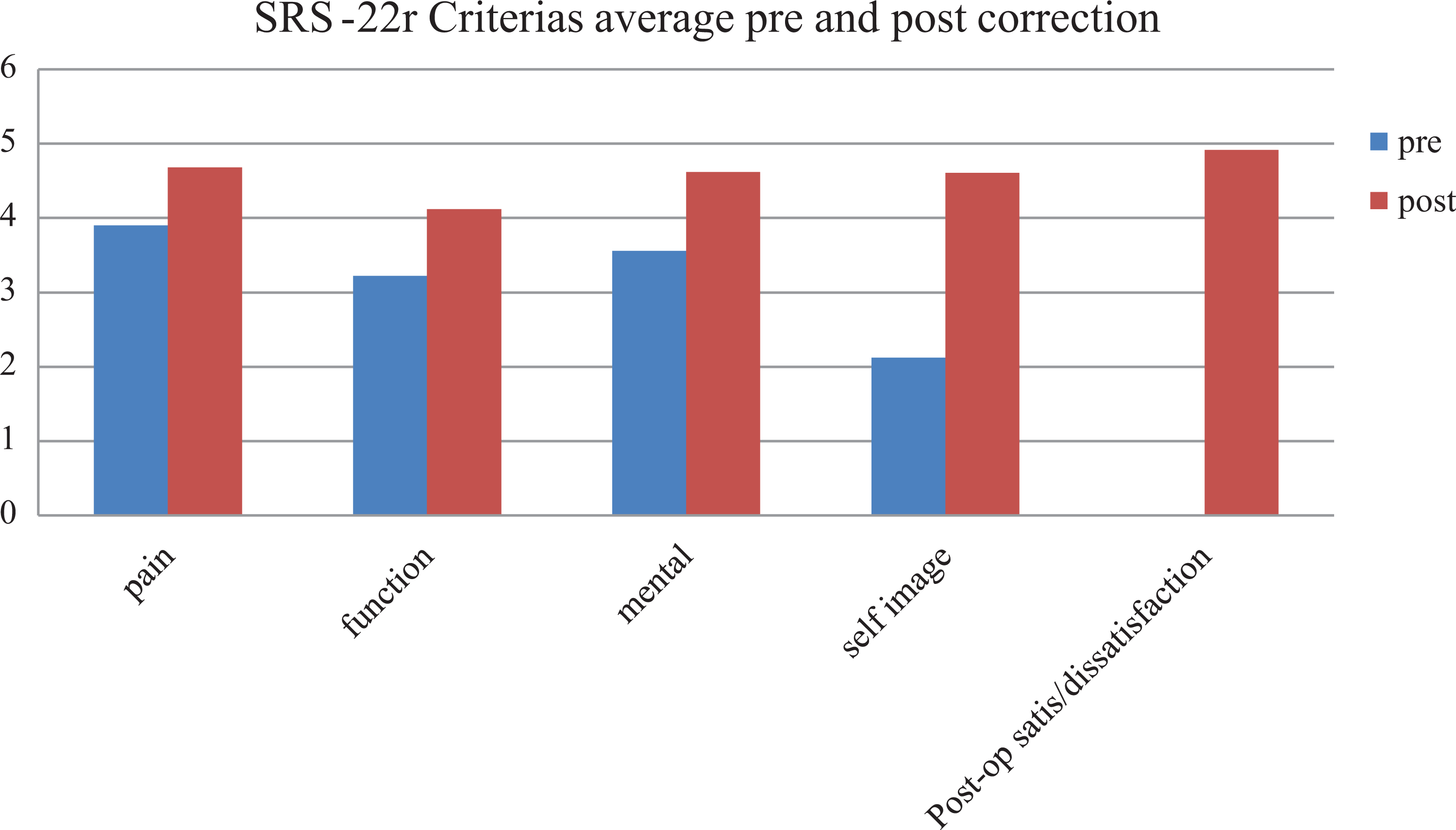
Diagram of correlation of SRS-2r pre- and post-surgery.
The range of SRS-22r values post-surgery was 4.16 and 4.96 (4.589 ± 0.291) and p-value = 0.046. The least results were that for function [the range was 3.2 and 4.8 (4.12 ± 0.37)] and the best results were that for treatment satisfaction [the range was 4 and 5 (4.96 ± 0.277)] (Table 3). Self-image can be obviously appreciated when the patient looks in the mirror (or is seen by his parents) and sees his height, abdomen, chest, and the absence of the kyphosis. Also, the patients feel better in terms of respiration, feeding, and post-surgery appearance.
SRS-22r values pre- and post-surgery.

SD: standard deviation.
Discussion
There is a limited rule of the conservative treatment of congenital kyphosis with bracing and there is no proof that it prevents progression or corrects the deformity. 3 Intraspinal malformations (duplication of the cord, tethered cord, or other deformities) are found in 20–40% of patients and should be treated surgically before treating the kyphosis. 1,3,23 Anterior, posterior, or combined approaches used to be done in the past to reconstruct the anterior compressive column and posterior traction column, but none of the studies confirmed which approach is the most suitable. Many surgical techniques were developed to correct kyphosis posteriorly, which are PVCR and reconstruction or shortening of the posterior column with PSO, wedge osteotomy, or decancellation of the vertebral body in addition to the posterior instrumentation. 3,19,20,21
The current study presents our results of treating 25 patients with severe thoracolumbar kyphosis who were treated with the single posterior approach. After insertion of pedicle screws and a suitable osteotomy according to the pathology (PVCR, PSO, wedge, or decancellation osteotomy), two rods were bent as needed and applied on the top of the screws. The correction was not satisfied for us, so we added gradual correction using the “in situ” bending instruments to overcome the residual deformity and tight the anterior soft and abdominal wall muscles.
The “in situ” bending is well known in correcting spinal deformities. Few previous studies mentioned the rule of the “in situ” bending in the correction of the congenital kyphosis, they used it once or twice to balance the spine and give it its final correction. Most of them were on a small number of different causes of sharp kyphosis; congenital, pathological, or traumatic. 24 –26 We could not find any study that talks about the repetitive gradual “in situ” correction. Thoracolumbar congenital kyphosis is usually sharply angulated (as seen in Figure 1), which may lead to anterior spinal cord compression as the spine grows, low back pain due to compensatory lumbar and/or thoracic lordosis. 2,3,5,14 In some cases, early-age surgical short segment fixation without fusion allows the anterior column to grow and may correct the deformity completely and avoid early spine fusion, which may lead to crankshaft phenomenon. 3 Adolescents and older patients underwent long segment fusion and fixation to correct the whole deformity and the sagittal balance at once.
Cho et al. reported improvement of 23 patients with acute thoracolumbar kyphosis of different causes with an average of preoperative Cobb’s angle of 71.8° and average Cobb’s angle of 39.2° at the final follow-up. The patients were treated with different approaches: anterior, posterior, or combined. 9 Atici et al. series of 10 cases with the mean local kyphosis reported the Cobb’s angle improvement from 67.7° before surgery to 31.5° after surgery. The patients were treated with closed wedge osteotomy. 3 Zeng et al. treated 23 mean kyphosis patients whose Cobb’s angle was 74.3° and improved to 21° after surgery. 1
Spiro et al. reported 10 severe congenital thoracolumbar kyphosis patients, their mean age was 11.1 years (5.4–14.1). These patients underwent PSO or PVCR through the single posterior approach. Cobb’s angles improved from 59.9° (45–110) preoperative to 17.5° at the final follow-up (3–40). 8 Wang et al. reported segmental kyphosis improvement from 87.3° before surgery to 17.6° post-surgery and 20.4° at the latest follow-up of 24 patients with congenital kyphosis who were treated with PVCR posteriorly. 12 Shi et al. mentioned the improvement of segmental kyphosis of 38 patients from 49.5 ± 11.7° at pre-operation, 6.8 ± 7.4° at post-operation (p < 0.001), and 8.0 ± 8.1° at the last follow-up. 20
Our study showed that the curves were corrected with this technique to about normal values; Cobb’s angle improved on average from 81.5° preoperatively to 21.7° at the final follow-up (p-value <0.0001).
The range of preoperative SRS-22r score values was 2.1 and 3.9 (3.2 ± 0.77) improved to 4.16 and 4.96 (4.59 ± 0.29) at final follow-up. Self-image and treatment satisfaction/dissatisfaction criteria showed the best results, which reflected the improvement of the patient’s body image, social presentation, and outfit choices with the disappearance of the kyphosis.
Using the repetitive gradual “in situ” corrective bending of severe thoracolumbar congenital kyphosis gave excellent clinical and radiological results. All our patients were satisfied with these results. Also, we found that the gradual correction is a safe procedure to relax the soft tissues for better deformity correction and to minimize the pulling-out of the screws. When it is used with spinal cord neuromonitoring, we can significantly minimize the chance of major neurological complications.
The patient’s standing height increased in all patients, although this improvement may be insignificant in the pre-puberty patients as they still have the growth potential. After puberty, height gain may be an important issue that is of psychological and social benefits for the patients. None of the previous studies mentioned the improvement of the patient’s height.
Limitations of this study include being a retrospective study, small number of patients (many of previous studies were less than our study), heterogeneity of the patients’ ages, different procedures of anterior column, neuromonitoring was not used in all patients, only one international score was used, no sagittal parameters were used in radiological evaluation, and being a single-institution study. We believe that more prospective multicenter studies with more patients should be done in the future.
Conclusion
Congenital kyphosis of the thoracolumbar area may occur due to failure of vertebral formation, which results in wedge or hemivertebra, or failure of segmentation, which results in an unsegmented bony bar. Surgical treatment is the best choice. Gradual correction with the “in situ” bender with or without osteotomy (excision of hemivertebra, PVCR, PSO, decancellation, or wedge osteotomy) through the single posterior approach can give satisfying clinical (patients’ standing height and SRS-22r scores) and radiological (Cobb’s angle) results.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.