
Abstract
Study design
A retrospective study.
Objectives
This study aimed to evaluate the clinical and radiological outcomes of pedicle subtraction osteotomy (PSO) at L2 and L3 levels in ankylosing spondylitis (AS) patients with similar kyphotic deformities. The primary focus was to compare these levels in terms of spinal alignment, sagittal balance, and functional improvements.
Methods
A retrospective analysis was conducted on 28 AS patients who underwent L2 or L3 level PSO between 2010 and 2021. Patients were divided into two groups based on osteotomy levels (14 in each group) and matched for similar kyphosis angles and deformity patterns. Radiological parameters, including pelvic tilt (PT), pelvic incidence (PI), sacral slope (SS), lumbar lordosis (LL), thoracic kyphosis (TK), global kyphosis (GK), spinosacral angle (SSA), sagittal vertical axis (SVA), osteotomized vertebral angle (OVA) were measured preoperatively, immediately postoperatively, and at final follow-up using SURGIMAP. Functional outcomes were assessed using VAS, ODI, and BASFI scores.
Results
Both groups showed significant improvements in sagittal alignment parameters such as PT, LL, and SVA postoperatively (p < 0.01). The L3 group demonstrated better sagittal balance, achieving the recommended SVA value (<47 mm) at follow-up, while the L2 group did not. There was no significant difference in radiological parameters between the groups (p > 0.05). Functional outcomes, including VAS, ODI, and BASFI scores, improved significantly in both groups (p < 0.001), with no significant differences between them.
Conclusions
L2 and L3 PSO levels yielded comparable radiological and functional outcomes in AS patients with similar curve patterns. Both levels can be effectively utilized for correcting rigid kyphotic deformities, with L3 providing slightly better sagittal balance.
Introduction
Ankylosing spondylitis (AS) is a progressive chronic inflammatory disease. It is more common in males and peaks in the third decade of life. The disease has an unknown etiology. It shows very strong associations with HLA B27, but the exact pathogenic role of HLA B27 in AS has not been disclosed yet. AS initially starts with sacroiliac joint involvement and later affects other joints. Patients often suffer from characteristic low back pain, but less frequently, spinal disease is accompanied by arthritis of the peripheral joints. 1
One of the biggest problems of AS patients is progressive kyphotic deformity. It leads to serious psychological and functional impairment. Patients have difficulty sitting, standing, or lying down. Due to the sagittal imbalance, patients have restricted visual area. The primary indication for surgery is to restore standing, sitting, and walking balance and obtain an appropriate horizontal visual axis. 2 In addition, correction relieves the compression of abdominal viscera and improves respiration.
Very few studies compared single-level osteotomy, and these studies compared L1 and L2 level PSO.3–6 According to previous literature, L3 level osteotomy has a longer lever arm and thus can correct a higher degree angle. In the literature, no study compares L3 to other level PSO in similar curve patterns.
In this study, we aimed to investigate clinical and radiological outcomes of L2 and L3 level PSO with similar curve patterns in AS patients.
Material and methods
The study protocol was in accordance with the Declaration of Helsinki and ethical approval was obtained from the Sakarya University Faculty of Medicine Clinical Research Ethics Committee (Approval no. E71522473-050.01.04-241688-134). Informed consent was obtained from all participants. After the ethics committee approved, between January 2010 and December 2021, in a single center, 103 AS patients who underwent osteotomy surgery were analyzed retrospectively. L2 and L3 PSO levels and a minimum of 2 years of follow-up patients were included in the study.
Patients with incomplete medical records who underwent revision spinal surgery and with additional deformities in lower extremities were excluded from the study. Patients with similar global kyphosis angle (±15°) and similar pre-operative apex (T11-L2), with L2 level PSO 14 patients (group 1), L3 level PSO 14 patients (group (2) total of 28 patients included in the study.
There were 22 male and six female patients with a mean age of 45.8 years (range 27–71). The main complaint for most patients was the inability to look straight. In addition, the indications for the surgery were the inability to lie down flat in bed, abdominal viscera compressions and subsequent indigestions, and severe limitations in their daily life like walking, driving, or communication inabilities with other people. All of them also had significant psychosocial impairment.
All patients have examined pre and post-operative anterior to posterior and lateral view spinal radiographic. Preoperative, early postoperative, and final follow-up postoperative sagittal spinal and spinopelvic parameters were measured using the SURGIMAP© (Nemaris Inc., USA) (https://www.surgimap.com/) measurement system. It was taken while patients stood with hips and knees extension and shoulders flexion at 45° posture. Radiographically evaluated parametres were; Pelvic tilt (PT, the angle creatid by a line running from the midpoint of S1 plate to the center of the femoral heads and vertical axis), pelvic incidence (PI, the angle between the line perpendicular the midpoint of the S1endplate and a line connecting to bicoxofemoral axis), sacral slope (SS, the angle between the line parallel to S1endplate and the horizontal reference), lumbar lordosis (LL, the angle between superior end plate of L1 and superior end plate of S1), thoracic kyphosis (TK, the angle between superior endplate of T5 and inferior end plate of T12), global kyphosis (GK, the angle between the superior end plate of maximally inclined upper vertebra and inferior endplate of maximally inclined lower vertebra), spinosacral angle (SSA, the angle running from the C7 and middle of sacral plate line and spinosacral line), sagittal vertical axis (SVA, the length of a horizontal line between the center of C7 vertebral body and posterior superior aspect of the S1 vertebral body), osteotomized vertebral angle (OVA, the angle between upper and lower and plate in osteotomized vertebra). Preop, immediate postop, and the last follow-up radiographical assessments were reviewed.
Visual analog scale (VAS), The Oswestry disability index (ODI), and The Bath ankylosing spondylitis disease activity index (BASFI) questionnaires were done preop and the last follow-up. Intraoperative blood loss, operation duration, hospitalization duration, and complications were also reviewed.
Statistical analysis
All mentioned parameters were compared between two groups, and NCSS(Number Cruncher Statistical System) 2020 Statistical Software (NCSS LLC, Kaysville, Utah, USA) was used for statistical analysis. While evaluating study data, quantitative variables were shown with mean, standard deviation, median, minimum, and maximum values, and qualitative variables were shown with descriptive statistical methods such as frequency and percentage. Shapiro Wilks test and Box Plot graphics were used to evaluate the conformity of the data to the normal distribution. The Friedman test and Bonferoni Dunn test were used for post-operative comparisons for variables that did not show normal distribution in group comparisons according to follow-ups. Mann Whitney-U test for the evaluations of non-normally distributed variables according to two groups; Wilcoxon Signed Rank test was used for in-group assessments. Spearman’s correlation analysis was used to evaluate the relationship between the variables. Fisher Exact test and Fisher’s Freeman Halton test were used to compare qualitative data. The results were evaluated at a 95% confidence interval and significance level of p < 0.05.
RESULTS
Comparison of descprictive features and operational data.

aFisher Exact Test.
bMann-Whitney-U Test.
cFisher Freeman Halton Test.
Comparison of radiological results according to groups.

aMann-Whitney-U Test.
bFriedman Test & Dunn test with corection.
cBonferoni.
*p < 0.05 **p < 0.01.
Comparison of clinical outcomes by groups.
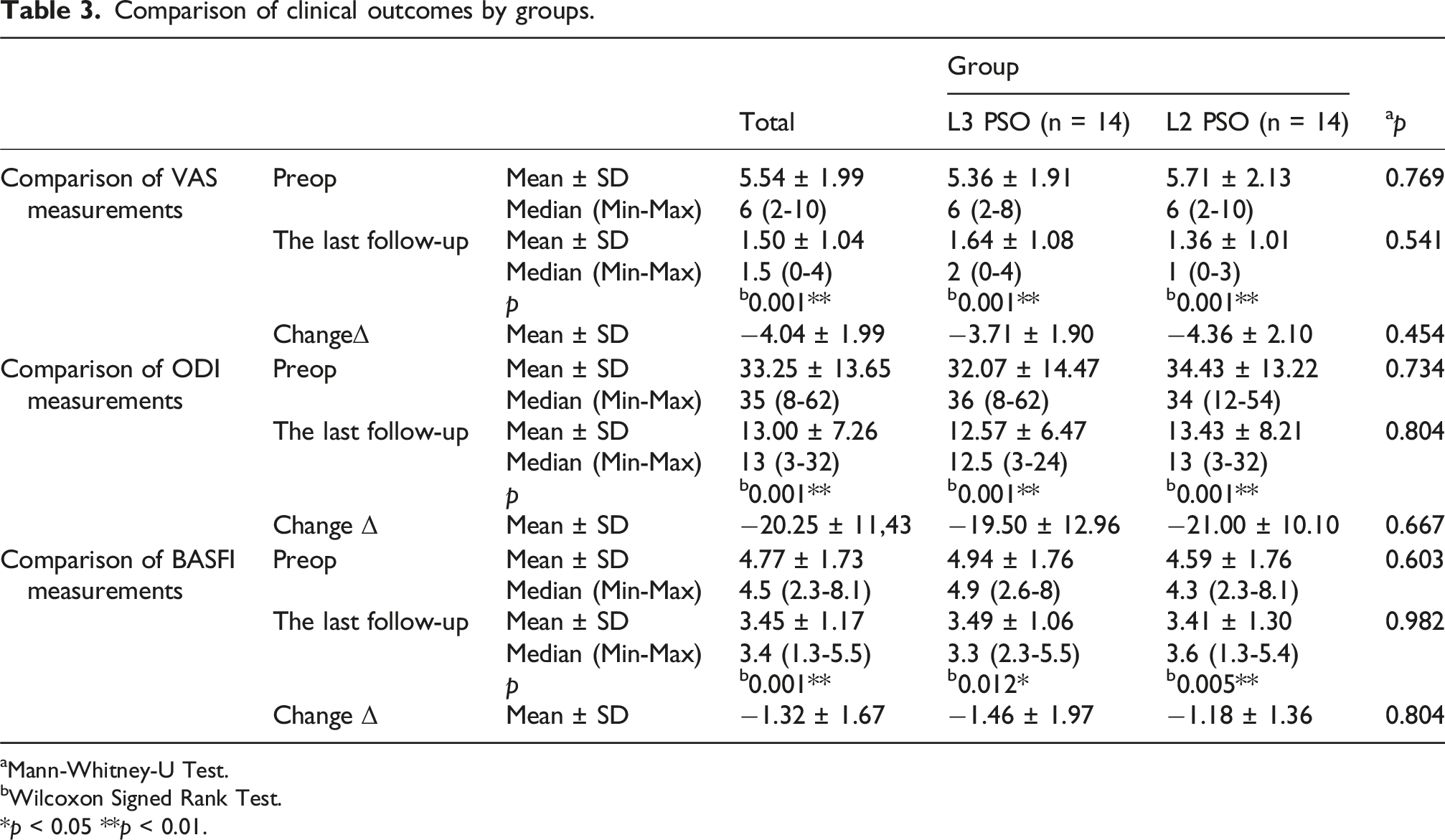
aMann-Whitney-U Test.
bWilcoxon Signed Rank Test.
*p < 0.05 **p < 0.01.
Reationship between preoperaive and early postoperative values and changes according to L3 PSO group.

r:Spearman’s correlation coefficient *p < 0.05 **p < 0.01.
Relationship between changes in preoperative and early postoperative values according to L2 PSO group.

r:Spearman’s correlation coefficient *p < 0.05 **p < 0.01.
Discussion
PSO has been described as an effective method in the treatment of rigid kyphosis.
1
Different opinions have been reported on the osteotomy level to be selected in the treatment of thoracolumbar kyphosis due to AS.2,3 Debarge et al. reported a close relationship between the PSO level and sagittal spinal and pelvic parameters.
8
Chen et al. reported in their experience with 78 cases that osteotomy from the lower lumbar spine was safer, while they suggested that osteotomy from the L2 and L3 vertebrae would provide maximum correction.
9
Tang et al. reported that osteotomy from the L2 vertebra provided greater correction in SVA than L1 when they compared osteotomy levels by matching AS patients with similar curve patterns for the first time
3
; however, Mittal et al. criticized the fact that osteotomy at the L3 vertebra level, which is routinely preferred in this study, and some important clinical and radiological parameters were not included in the study.
10
In this study, we compared the PSOs performed at L2 and L3 levels by matching AS patients with similar curve patterns. In addition, we compared the early postoperative evaluations, SSA (Figures 1 and 2) OVA measurements, and BASFI scoring by including them in the study. Preoperative, early postoperative and 4rd year postoperative spinal lateral radiographs of a 32-year-old female patient who underwent L3 PSO. Preoperative, early postoperative and 6th year postoperative spinal lateral radiographs of a 41-year-old female patient who underwent L2 PSO.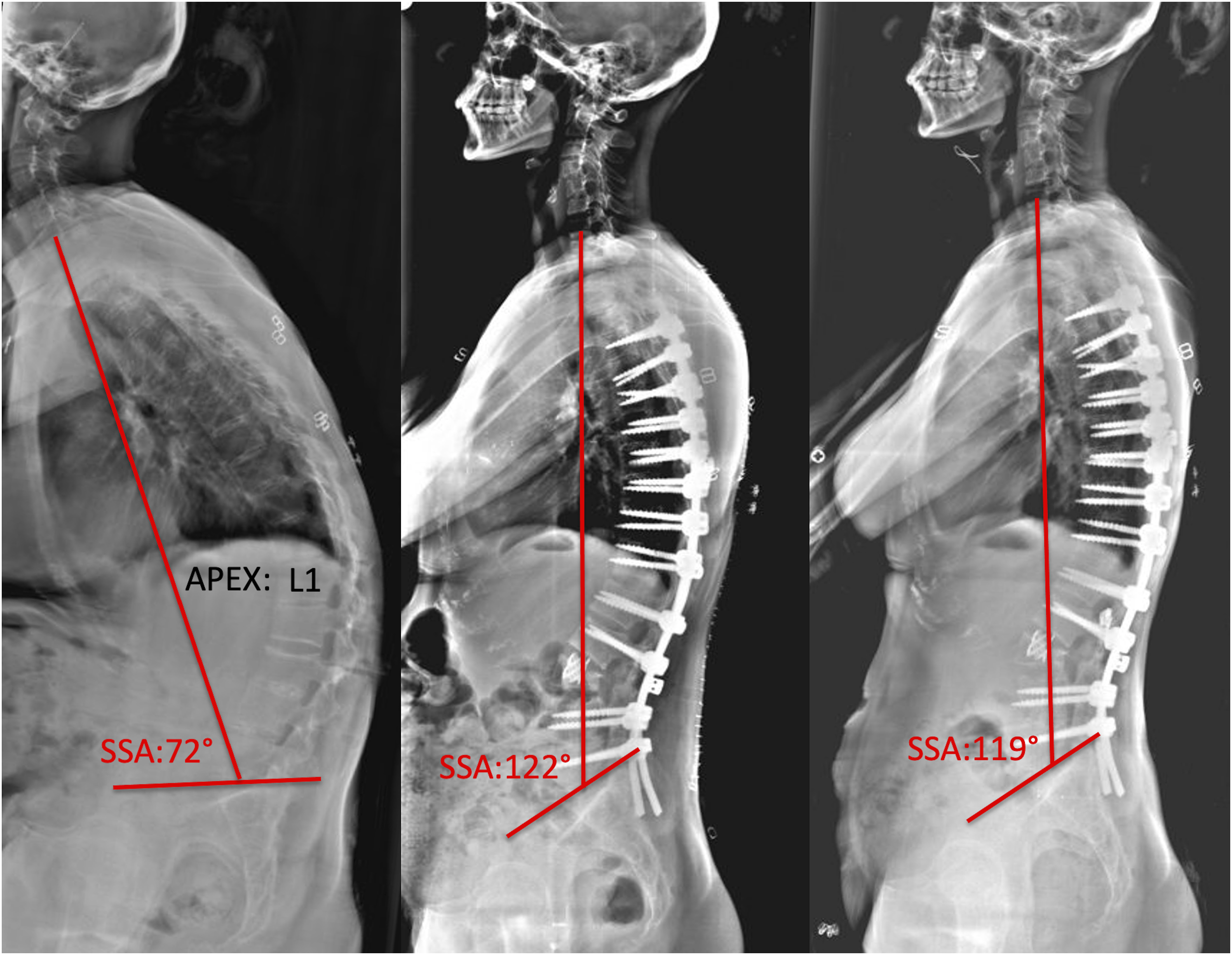

Except for TK, other sagittal spinal parameters improved significantly. No significant difference was observed between the groups in any of the radiological parameters at preoperative, early postoperative, and final follow-up. At the final follow-up, the mean SSA increased significantly from 88° to 112.6°. Mean SVA decreased significantly from 127 mm to 49 mm, and mean GK decreased significantly from 80.1° to 63.9°. This value in SVA was above the optimal sagittal alignment value recommended by Schwab et al..
11
When the groups were examined separately, it was seen that the recommended SVA value could be reached in the L3 group but not in the L2 group. Although there was no significant difference between the SVA changes between the two groups, it was seen that the L3 group provided better sagittal balance. Unlike previous studies, no significant change was detected in the PI value in the early postoperative period, while an average increase of 4.3 was observed at the final follow-up compared to the preoperative period (Figure 3). Studies suggesting that PI, which is normally considered constant, may change after spinopelvic fixation have been reported recently.
12
This change in PI value can be explained by the application of spinopelvic fixation in 13 of 28 patients (46%) in our study. Graphical presentation of preoperative, immediate postoperative and the last follow-up values of sagittal spinal parameters according to groups: Global Kyphosis (A); Spino Sacal Angle(B); Sagittal Vertical Axis(C); Osteotomized Vertebrae Angle(D); Pelvic Incidence(E); Pelvic Tilt(F); Sacral Slope(G); Lumbar Lordosis(H).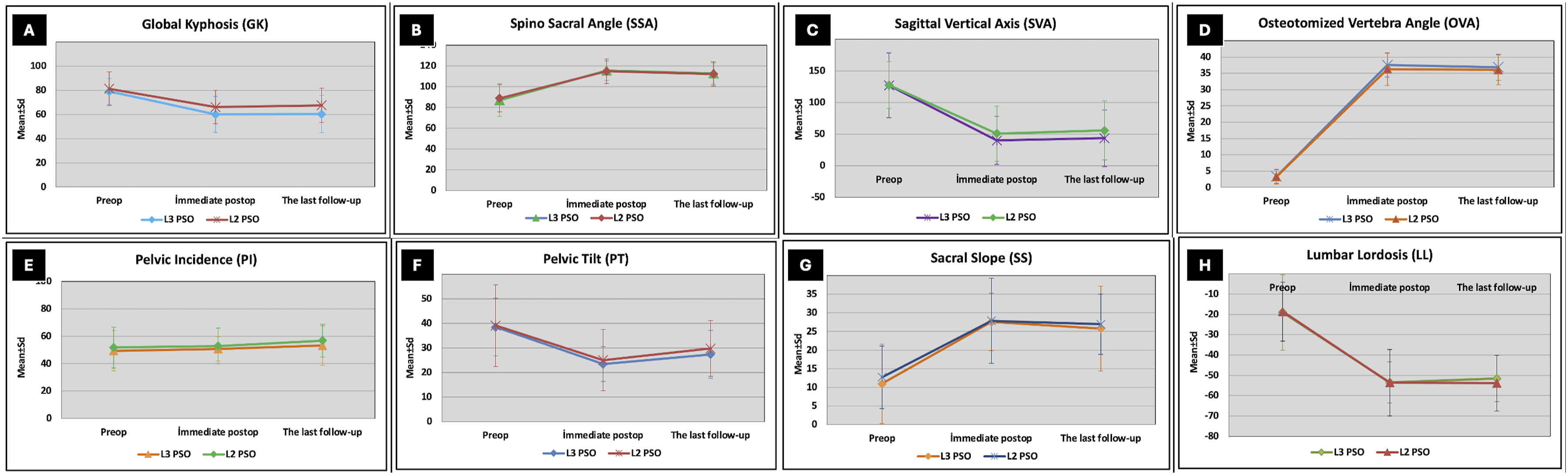
Studies have shown that the most important parameter in providing sagittal spinal alignment is the restoration of the LL.13,14 Luan et al. It was reported that patients who applied PSO due to thoracolumbar kyphosis due to AS had a longer force arm as they moved from T12 to L3, and maximum improvement was achieved in LL and SVA. 2 In our study, it was observed that an average correction of LL of 35° was achieved in both groups, and there was no difference between the groups. This can be explained by the fact that the L2 and L3 vertebrae are in the midlumbar and have similar pedicle widths. The fact that the OVA changed by 33° and 34° in osteotomies performed from the L2 and L3 vertebrae, respectively, supports this situation.
Recent studies have shown that AS patients have lower health-related quality of life scores (HRQoL) compared to the general population but similar to patients with other rheumatologic disorders. 15 In our study, VAS, ODI, and BASFI scores, which were low preoperatively, all improved significantly postoperatively. Despite having different osteotomy levels, the groups showed similar improvements in HRQoL scores. After surgery, the patients in both groups expanded their visual areas, their pain significantly reduced, and their quality of life increased. As the osteotomy level shifts distally, spinopelvic fixation may be necessary to maintain spinal sagittal balance, and studies are reporting that spinopelvic fixation in AS may be associated with lower ODI scores, 16 while studies are reporting that it does not affect clinical outcomes. 2 In this study, we could not evaluate this situation comparatively since there were similar spinopelvic fixation rates in both L2 and L3 PSO groups, but we observed that HRQoL scores of patients who underwent spinopelvic fixation also improved.
The current study has methodological limitations due to its retrospective nature. First, the sample group was relatively small due to strict inclusion criteria. Second, since patients who underwent spinopelvic fixation were not evaluated as a separate group, its effect on clinical outcomes could not be examined. Third, among the radiographic parameters, we did not evaluate some important sagittal parameters such as ChinBrow Vertical Angle and C2C7 lordosis, which have a significant effect on the patient’s forward-looking ability and quality of life in AS. Despite all these limitations, our study is valuable in terms of comparing the L2 and L3 vertebra levels, which are the most commonly preferred for PSO in thoracolumbar kyphosis surgery due to AS, on patients with similar curve patterns.
Conclusion
This study showed that osteotomy at L2 and L3 levels in AS patients with similar curve patterns resulted in similar radiological and functional outcomes. Surgeons can individually evaluate and use both osteotomy levels for optimal correction and healing.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.