
Abstract
Purpose:
Anatomical sacral slope (a-SS), a pelvic anatomical parameter that does not require the center of the femoral head, strongly correlates with pelvic incidence (PI) during three-dimensional measurements in normal subjects. Sagittal alignment of spinal and pelvic parameters is typically evaluated using two-dimensional radiographs; however, the relationship between a-SS and PI has not been evaluated using radiographs. This study aimed to evaluate the correlation between a-SS and other spinal and pelvic parameters using radiographs.
Methods:
We evaluated 144 healthy women. Using sagittal radiographs, we measured lumbar lordosis (LL), thoracic kyphosis, PI, SS, pelvic tilt, and a-SS, which were defined as the angle between the superior end plate of S1 and a line perpendicular to the anterior pelvic plane. Pearson coefficients were used to determine correlations, and intraobserver and interobserver intraclass correlation coefficients (ICCs) were used for validation.
Results:
There was a strong correlation between PI and a-SS (r = 0.756). Moreover, correlations between a-SS and LL and between PI and LL were similar (r = 0.661 and r = 0.554, respectively). The intraobserver ICCs were 0.884 for a-SS and 0.840 for PI. The interobserver ICCs were 0.856 for a-SS and 0.653 for PI.
Conclusion:
a-SS was strongly correlated with PI. The correlation between a-SS and LL was equivalent to the correlation between PI and LL. Moreover, the ICC for a-SS was larger than that of PI. This study suggests that a-SS is a useful new pelvic anatomical parameter that can be used instead of PI.
Introduction
Pelvic incidence (PI) is a well-known pelvic parameter that affects sagittal spinal balance and posture in the standing position. 1,2 PI was first described by Legaye et al. 3 as an anatomical parameter of the pelvis, defined as the angle between the line perpendicular to the sacral plate at its midpoint and the line connecting this point to the axis of the femoral head (Figure 1). PI is significantly correlated with other radiographic thoracolumbar spinal and pelvic parameters such as lumbar lordosis (LL) and sacral slope (SS). 4,5 A high PI may lead to the forward displacement of the sagittal vertical axis and may be a risk factor for spondylolisthesis. 6,7 Furthermore, PI-LL mismatch affects adult spinal deformity. 8 Therefore, PI is considered clinically important and should be evaluated.

Pelvic parameters. PI: pelvic incidence; SS: sacral slope; PT: pelvic tilt; L-ASIS: left anterior superior iliac spine; R-ASIS: right anterior superior iliac spine; APP: anterior pelvic plane.
Sagittal alignment of the thoracolumbar spinal and pelvic parameters is typically evaluated by two-dimensional (2-D) sagittal radiographs in the standing position. 3,9 SS is defined as the angle between the line of the sacral plate and the horizontal line perpendicular to the direction of the force of gravity, and pelvic tilt (PT) is defined as the angle between the line connecting the midpoint of the sacral plate to the femoral head axis and the vertical line parallel to the direction of the force of gravity (Figure 1). These angles are related geometrically by the following formula: PI = SS + PT. SS and PT are considered as positional parameters because the angles depend on horizontal or vertical lines that are perpendicular or parallel to the force of gravity and are affected by the position of the subject. Conversely, the PI angle is considered an anatomical parameter because it remains the same regardless of the position of the subject.
Anatomical sacral slope (a-SS), which has been described in a previous study, is defined as the angle between the superior end plate of S1 and the line perpendicular to the anterior pelvic plane which is defined as the line connecting the midpoint of the bilateral anterior superior iliac spine to the pubic symphysis 10,11 (Figure 1). The measurement of a-SS does not depend on the femoral head. Previously, a strong correlation was found between PI and a-SS in normal subjects and patients with developmental dysplasia of the hip (DDH) using three-dimensional (3-D) measurements. 10 Therefore, a-SS may be useful for estimating PI and may be a novel anatomical parameter of the pelvis that does not require the center of the femoral head for measurements.
The purpose of this study was to evaluate the correlation between PI and a-SS using 2-D radiograph measurements of normal subjects. We also evaluated the correlation between a-SS and LL using 2-D sagittal radiograph measurements.
Materials and methods
This study included female patients who visited an osteoporosis clinic in our institution and underwent standing radiography of the thoracic and lumbar spine areas to assess the presence of asymptomatic vertebral fractures and spinal sagittal alignment from April 2015 to March 2017. The subjects were 194 Japanese women. The mean age was 64.3 (standard deviation (SD) 8.1; range 47–84) years, and the mean body mass index was 23.8 (SD 4.2; range 12.6–34.7) kg/m 2 . We excluded subjects who had vertebral fractures evident on thoracic and lumbar spine radiographs and those who had undergone surgeries of the hip joint, such as total hip arthroplasty. The remaining 144 women were included in this study, and we retrospectively examined the standing radiographs of the thoracic and lumbar spine areas in these subjects. As we evaluated only thoracic and lumbar radiographs, women with asymptomatic DDH could not be excluded from this study.
This study was approved by the ethics review board of Niigata University Graduate School of Medical and Dental Sciences (no. 2017-0178), and the need for informed consent was waived because of its retrospective nature.
Measurements of spinopelvic and spinal parameters
We measured PI, SS, a-SS, thoracic kyphosis (TK), and LL using standing thoracic and lumbar radiographs that included the pelvis. PI, SS, PT, and a-SS have been defined previously. LL was the angle measured from the inferior end plate of T12 and the superior end plate of S1 (Figure 2). TK was the angle measured from the superior end plate of T1 and the inferior end plate of T12 (Figure 2). We measured twice with 1-week interval to determine intraobserver reliability. We compared the measurements performed by another observer with our measurements to assess interobserver reliability.

Sagittal spinal parameters. LL is measured from the inferior end plate of T12 and superior end plate of S1. TK is measured from the superior end plate of T1 and inferior end plate of T12. LL: lumbar lordosis; TK: thoracic kyphosis.
Statistical analysis
We analyzed the data using SPSS (version 21; SPSS, Inc., Chicago, Illinois, USA). Pearson coefficients were used to determine the correlation coefficients of PI, SS, a-SS, LL, and TK according to Guilford and Fruchter’s definition. 12 The mean absolute difference (MAD), variability (SD), intraobserver reliability and interobserver reliability with intraclass correlation coefficients (ICCs), and two-sided 95% confidential intervals were calculated to evaluate variations. Statistical significance was set at p < 0.05.
Results
Details of the parameters are provided in Table 1. There was a strong correlation between PI and a-SS (r = 0.756), as defined by Guilford and Fruchter 12 (Table 2), which was similar to that reported in a previous 3-D study. 10 The following regression equation was used: PI = 0.8 × a-SS + 18.
Measurements of spinopelvic and spinal parameters in 144 healthy Japanese women without spinal pathology.a

PI: pelvic incidence; SS: sacral slope; PT: pelvic tilt; a-SS: anatomical sacral slope; TK: thoracic kyphosis; LL: lumbar lordosis; SD: standard deviation.
a Mean ± SD (range). All data are normally distributed.
Correlations of pelvic parameters and sagittal spinal parameters.
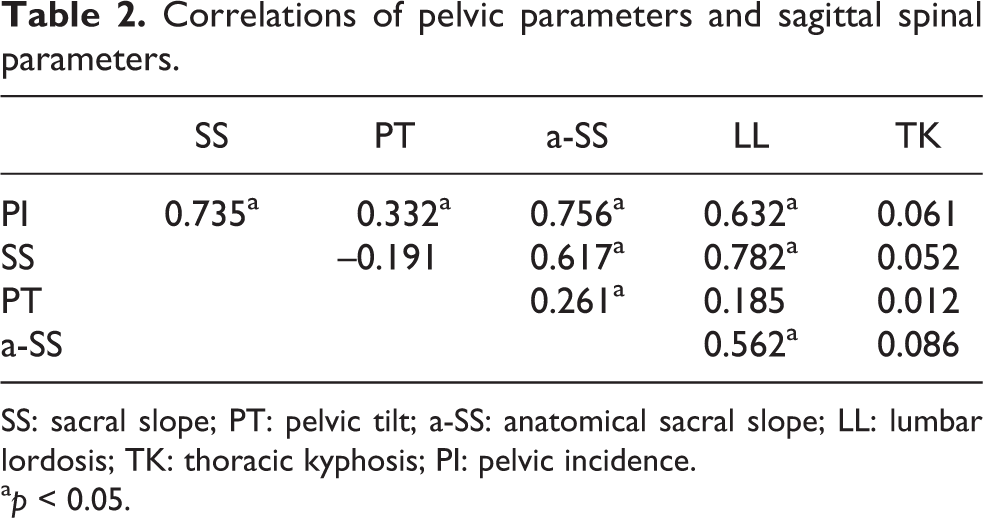
SS: sacral slope; PT: pelvic tilt; a-SS: anatomical sacral slope; LL: lumbar lordosis; TK: thoracic kyphosis; PI: pelvic incidence.
a p < 0.05.
Regarding the correlation between pelvic parameters and LL and TK, there was a strong correlation between SS and LL (r = 0.782), and this value was the highest among all the pelvic parameters in this study. Among the anatomical parameters, correlations between a-SS and LL and between PI and LL were similar (r = 0.562 and r = 0.632, respectively; Table 2). However, there were no correlations between TK and PI, PT, SS, or a-SS.
Intraobserver MADs ranged from 2.5° for SS to 3.6° for PI, and the minimum ICC was 0.727 for TK (Table 3). However, the interobserver MADs were slightly larger than the intraobserver MADs (maximum MAD was 4.6° for PI), and the minimum ICC was 0.653 for PI (Table 3).
Reliability of the measurement values.a

PI: pelvic incidence; SS: sacral slope; PT: pelvic tilt; a-SS: anatomical sacral slope; TK: thoracic kyphosis; LL: lumbar lordosis; MAD: mean absolute difference; ICC: intraclass correlation coefficient.
a MAD ± SD (ICC).
b p < 0.05.
Discussion
In this study, PI was strongly correlated with a-SS, and PI could be estimated from a-SS. The correlation coefficient for a-SS and LL was similar to that for PI and LL (r = 0.661 and r = 0.554, respectively). The subjects involved in this study were healthy women, without spinal pathology; however, subjects with asymptomatic DDH could not be excluded. The mean values were as follows: PI = 51.9 ± 10.4°, SS = 35.5 ± 9.9°, and LL = 51.3 ± 12.8°. Previous reports showed that PI ranged from 44.9° to 52.4°, SS ranged from 32.8° to 39.8°, and LL ranged from 48.8° to 58.1° in normal adults. 3,13,14 Legaye et al. reported that PI and SS were strongly correlated with LL in 49 normal adults. 3 Our results are similar to those of this previous report. Therefore, our measurement values seemed valid.
Schwab et al. 8 reported that PI-LL mismatch (PI-LL ≥ 11°) predicted disability in spinal deformity patients. After spinal fusion surgery for lumbar degenerative disease, PI-LL mismatch led to residual symptoms such as low back pain and other disabilities. 1,15 Therefore, defining PI is important. However, this requires identification of the femoral heads, which is occasionally difficult, especially in patients with nonspherical femoral heads, such as those with osteoarthritis of the hip. For such patients, a novel parameter that does not require the femoral head is needed.
According to the 2-D radiological measurements, PI was strongly correlated with a-SS in this study. The results were similar to those of a previous report that showed a strong correlation between PI and a-SS according to the 3-D measurements of the hip in normal subjects. 10 Therefore, PI could be estimated from a-SS using the following regression equation: PI = 0.8 × a-SS + 18. Furthermore, the significant correlation between a-SS and LL was similar to that between PI and LL. Therefore, a-SS may be useful for estimating PI and maybe a novel anatomical parameter of the pelvis that does not require the center of the femoral head for measurements, as it can be measured in patients with femoral heads that are nonspherical, flattened, or dislocated.
In addition, intraobserver and interobserver MADs of a-SS were smaller than those of PI, which used the center of the femoral head for measurements. Therefore, according to the 2-D radiological measurements, a-SS may have higher reliability than PI.
The current study had several limitations. First, only a few subjects were enrolled. Second, the subjects in this study were only healthy women; however, those with asymptomatic DDH could not be excluded. We previously found that PI of normal subjects was significantly smaller than that of DDH patients; however, a-SS of normal subjects did not significantly differ from that of DDH patients. 10 Therefore, the regression equation calculating PI from a-SS may differ between normal subjects and DDH patients. Further studies involving DDH patients are required. Third, only Japanese subjects were involved in this study. Arima et al. 16 reported that sagittal thoracolumbar spinal and pelvic parameters differed among African American, Caucasian, and Asian populations. Therefore, our results may be different from those for other races. However, correlation among spinopelvic parameters was reported in a previous study in Europe, 3 and it is similar to the finding in our study. Therefore, there may be no significant differences in the correlations of spinopelvic parameters among races.
a-SS is a novel parameter that is easy to use and can be measured using 2-D sagittal radiographs obtained in the standing position. Moreover, the correlation between a-SS and LL was similar to the correlation between PI and LL, and the 2-D results were similar to previous 3-D results. 10 We suggest that a-SS, which does not use the center of the femoral head, is a useful and novel pelvic anatomical parameter that can serve as an alternative to PI. Further large-scale studies involving not only normal subjects but also patients with hip and/or spinal diseases are required to validate the superiority of a-SS as an anatomical parameter.
Conclusion
a-SS was strongly correlated with PI according to 2-D radiological measurements. These results correspond with the findings in our previous report involving 3-D measurements. PI and a-SS were equivalent in terms of correlation with LL. Our results suggest that a-SS, which does not use the center of the femoral head, is a useful new pelvic anatomical parameter that can replace PI.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.