
Abstract
Objective: In a descriptive study we present the CAT-scan norm data of pelvic sizes in Caucasian men and women. The study was performed to investigate possible differences in pelvic sizes between men and women and the inter-individual range of pelvic sizes. The data may be useful as a guide in the development of orthoses and prostheses.
Methods: Pelvis CAT-scans of 40 subjects, 20 males (23–66 years) and 20 females (20–72 years) were investigated. The research was approved by the regional ethics committee.
Results: The angle of the ramus ossis ischii (ROI) with the line of progression in the transverse plane (angle a) was 38.6° (SD 3.4) in females and 31.8° (SD 4.4) in males. This difference was statistically significant (Student's t-test (p < 0.0001). The ROI angle in the coronal plane (angle b) was negative or zero both in males and females. The horizontal distance between the medial border of the ROI and the lateral border of the femur (RF distance) was slightly smaller in females (95 mm) compared to males (107 mm), but this difference was not statistically significant. The distance between the midfemoral line and the anterior surface of the leg was also slightly smaller in females (89 mm) than in males (106 mm) but the difference was not statistically significant. We found a linear relation between the total AP soft tissue distance and the soft tissue circumference of the proximal leg at the level of the ROI.
Conclusion: There are significant gender differences in pelvic size and shape. The medial plane of the ROI is not in a slight angle of inclination towards the midline but appears to be zero. The medial contour of the ROI in the AP direction is slightly curved.
Keywords
Introduction
It is challenging to create an optimal pelvic support in the production of prostheses and orthoses. The pelvic support region must be designed to: (i) Achieve vertical support of body weight, (ii) stabilize the residual skeleton in both the coronal and sagital planes, (iii) accommodate functioning muscles, (iv) voluntary control the prosthetic knee, (v) individualize design, and (vi) provide optimum balance and comfort, function and appearance, both statically and dynamically (Michael 1990). The biomechanics of the coupling between the skeleton and the socket is an important factor for socket fit. This coupling is affected by the relative slippage between the subject's skin and the prosthetic socket. A loose fit may allow slippage, which may compromise stability, while a very tight fit may offer a more stable connection (Mak et al. 2001). In the past, various techniques and designs have been advocated and, in general, most use medially the ramus ossis ischii (ROI) of the pelvis and laterally the femur to transfer axial load from the body to prostheses or orthoses. In 1954, Charles Radcliffe developed the quadrilateral socket shape (Metzger 2006). During the 1980s, Ivan Long (Long 1985) introduced the Long's Line, and soon after, John Sabolich (Sabolich 1985) described the Contoured Adducted Trochanteric Controlled Alignment Method (CAT/CAM). In the same period the Narrow Medial Lateral (NML) concept was introduced by Swiss and German CPOs (Baumgartner and Botta 1995) and finally, in 1999, Marlo Ortiz introduced a modification of this NML principle with the ischial-ramal containment socket (M.A.S). When considering these relatively fast developmental changes and the current broad range of underlying opinions, one must conclude that an adequate support of the pelvis remains a challenging issue. Reliable studies comparing the different types of pelvic support are lacking. One of the reasons explaining the difficulty in adequately fitting and supporting the pelvis is the relatively complex anatomical shape and the individual contour differences of the ROI. Another important reason may be individual differences in the bony size of the pelvis, gender differences and the differences in ratio of bone and soft tissue. Since there is, from an empirical view, no clear theoretical concept of an ideal pelvic support, we decided to review the human anatomy and performed a descriptive study using CAT-scans to accurately measure the pelvis; i.e., shape of the ROI in diverse planes, analysing the individual differences in de ramus-femoral distance and the relation between anterior-posterior soft tissue distance versus the soft tissue circumference. These CAT-scan data are presented and we hope that this might prove useful as a guide in the development of better orthoses and prostheses.
Methods
Research questions
What is the angle of the ramus ossis ischii (ROI) with the line of progression in the transverse plane (angle a)?
What is the ROI angle in the coronal plane (angle b)?
What is the horizontal distance between the medial border of the ROI and the lateral border of the femur (RF distance) in men and women and what is the variance of the mean?
What is the inter-individual difference in the distance between anterior soft tissue border and the midfemoral line (AP distance)?
What is the relation between the total AP soft tissue distance and the soft tissue circumference at the level of the ROI?
Pelvic CAT-scans from a group of 40 adult Caucasian patients, 20 males (age 23–66 years, mean 44 years) and 20 females (age 20–72 years, mean 41 years) performed on a routine basis as part of the acute trauma protocol of the University Medical Centre St Radboud, Nijmegen, were analysed. Patients who had fractures or dislocations of the pelvis were excluded. All CAT-scans were performed with the same scanning protocol with 3 mm thickness slices and bone settings. Pelvic sizes were analysed in the transverse plane images. Figure 1 demonstrates how pelvic sizes and angles were measured. The angle (a) of the ROI with the line of progression was measured on the first transverse slice caudally from the foramen obturatum. The line of progression was drawn perpendicular to the line between the left and right femora. The measuring error of angle a was reduced by averaging the left and right ROI angle a. The mean angle of the ROI with the line of progression is presented for men and women separately with the standard deviation of the mean. The angle of the ROI in the coronal plane (b) was calculated by measuring the distance (1) on the most caudal image of the ramus between the medial border of the ramus and the mid-line of the body and measuring the distance (2) on the most cranial image of the ramus just caudally of the foramen obturatum between the medial border of the ramus and the mid-line. Distance 2 was standardly measured eight slices cranially of the most caudal image (1). By subtracting distance 1 and 2, the coronal angle of the ROI can be calculated goniometrically. When the distance 1 minus distance 2 was a negative value we presented the angle b of the ramus as zero.
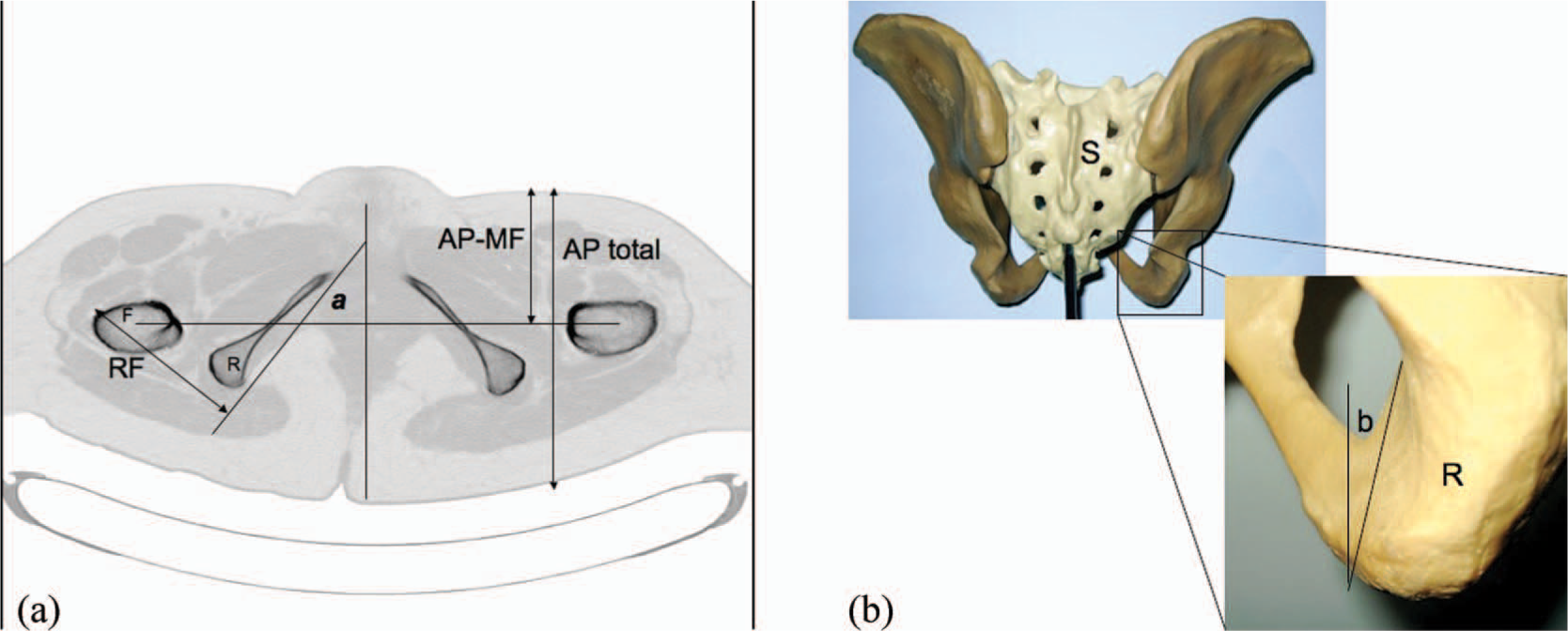
(a) CAT-scan of the female pelvis (transaxial image). Presented is the first transaxial image immediately caudally of the foramen obturatum. Femur (F), ramus ossis ischii (R), ramusfemoral distance (RF), ramus angle a, AP midfemoral distance (AP-MF), total AP distance (AP total). (b) Dorsal view on the pelvis to demonstrate the coronal ramus angle b, sacrum (S), ramus (R).
The horizontal distance between the medial border of the ROI and the lateral border of the femur (RF distance) was measured on the first transverse image caudally of the foramen obturatum.
The distance between the anterior body soft tissue border and the mid-femoral line (AP-MF distance) was measured on the first transverse image caudally of the foramen obturatum. On the same image we measured the body total AP distance and the circumference of the leg.
The research was approved by the regional ethics committee in Nijmegen, The Netherlands; CMO (Commissie Mensgebonden Onderzoek) nr 2005/093. The investigations were in accordance with the protocol and followed the ethical and humane principles of research. Informed consent was obtained from the patients stating that data from CAT-scans may be used for publication.
Results
Mean values of pelvic angles and sizes. Angles are presented in degrees and distances in mm, between brackets the standard deviation of the mean

An impression of the ROI shape in the transverse plane is presented in Figure 3. Five detail images of the ROI are shown. The medial margin of the ramus appeared to have a slightly arched form. This shape is similar in men and women.
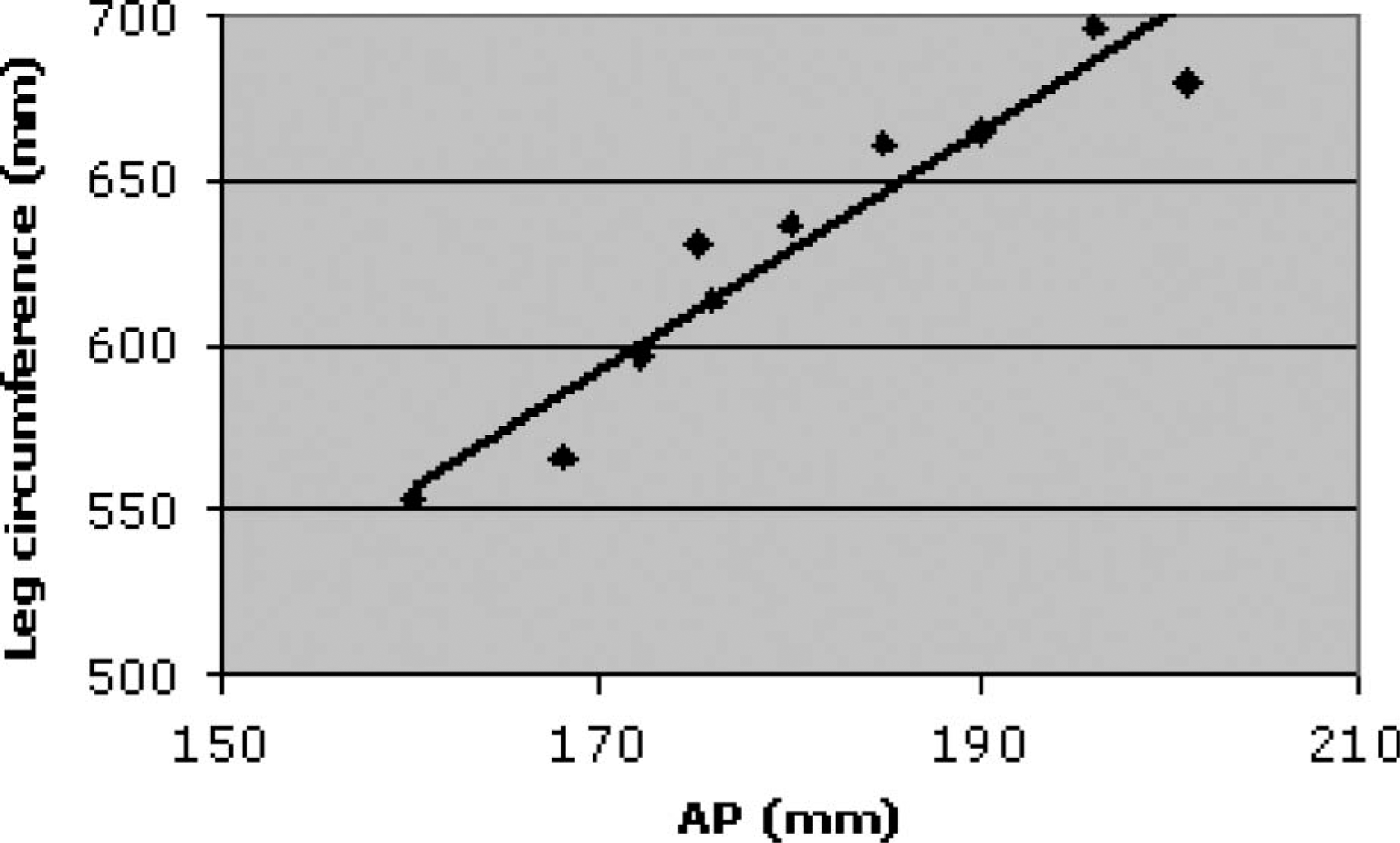
Relation between the body total AP distance and the leg circumference at the level of the ramus ossis ischii.
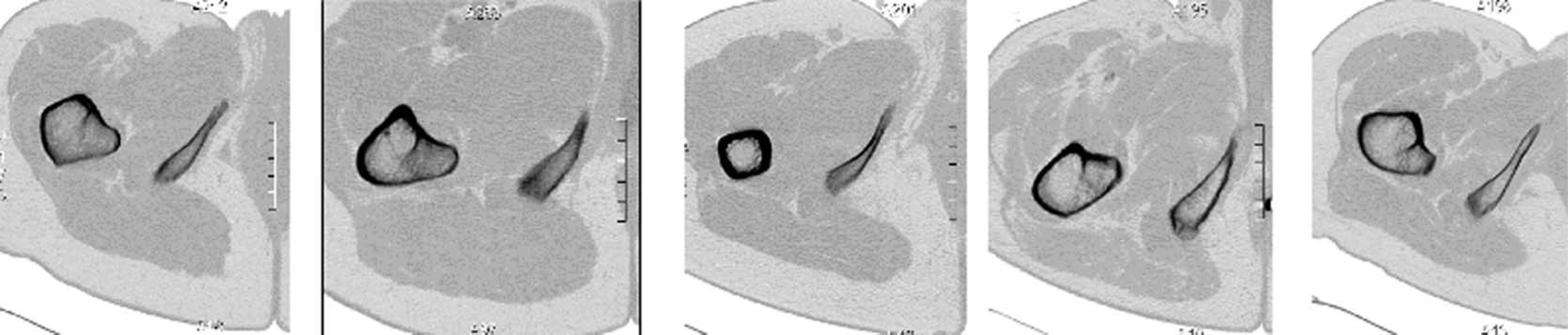
Detail of medial curvature of the tuber/ramus ossis ischii in the transverse plane, presented are images 1 cm cranially of the most caudal image of the ramus ossis ischii.
Discussion
The pelvic CAT-scan data of 40 Caucasian subjects are presented here. To our knowledge no other studies using CAT-scans have been performed on this topic. In the literature there are some empirical data regarding pelvic size and the gender differences (Baumgartner and Botta 1995). Without any references, the angle a of the ramus is in the literature considered to be 45° in females and 30° in males (Baumgartner and Botta 1995). In our CAT-scan study a mean ramal angle a of 39° in females and 32° in males was found. This gender difference of the ramal angle a was statistically significant. In our CAT-scan data we found no significant differences in RF or ML distance between males and females. However, the range of the RF or ML measurement was large between the different subjects; the smallest RF or ML distance in our study was 76 mm and the largest 130 mm. It must be taken into account that the RF or ML dimension measured on CAT-scans does not exactly correspond to the clinical RF or ML distance measured with sliding callipers. In the first place, the CAT-scan measure is specifically bony distance, not including soft tissue. Secondly, the CAT-scan measurement is a non-weight bearing situation, the patient being supine with the legs slightly exorotated. External rotation of the leg causes a slight decrease in RF or ML dimension.
Conclusion
There are significant gender differences in pelvic size and shape. The medial plane of the ramus is not in a slight angle of inclination towards the midline but appears to be zero. The medial contour of the ramus is slightly curved in the AP direction.