
Abstract
Background:
Complete tumor removal and damaged nail bed repair are critical factors that determine the success of subungual tumor excision. We examined a modified proximally based nail bed flap approach for excision of subungual bone tumors of the distal phalanx and present cases where this approach was used, along with postoperative functional and cosmetic outcomes.
Methods:
Twenty-four benign subungual bone tumors, identified from 23 patients (9 males and 14 females), were included in this study. All patients underwent tumor excision by the modified proximally based nail bed flap approach. Pain was assessed using a numeric rating scale, and cosmesis was self-assessed using a visual analog scale preoperatively and 1 year postoperatively. We measured sensation of the involved digit tip, relative to opposite-side sensation, using static and moving two-point discrimination and Semmes–Weinstein monofilament tests 1 year postoperatively. Lastly, we assessed postoperative nail deformities and tumor recurrence as potential surgical complications.
Results:
Mean pain severity and cosmesis were significantly improved 1 year postoperatively. There were no significant differences in the digit tip sensation between the involved and the opposite-side digits 1 year postoperatively. We observed one case of tumor recurrence and four cases of postoperative nail deformities.
Conclusions:
The modified proximally based nail bed flap approach showed satisfactory functional and cosmetic outcomes. This approach enables a low rate of recurrence after removal of benign subungual bone tumors in the short term and cosmetically superior nail bed repair.
Level of evidence: Therapeutic, IV
Introduction
Subungual tumors encompass diverse phenotypes from benign to malignant and have a variety of clinical manifestations. 1,2 The typical clinical manifestations of subungual bone tumors involve painful, hard, and exophytic masses, nail deformities, nail bed damage resulting in discharge or infection, and nail lifting or extraction, often compromising quality of life. 1
Benign subungual bone tumors include osteochondromas, exostosis, and enchondromas. 3 Standard care typically includes tumor excision nail apparatus preservation. 1 Despite the relatively small size and superficial location of these tumors, surgical approaches are sometimes very difficult because the nail bed is located just above the mass. Therefore, proper surgical technique is the most critical factor to prevent nail deformities and reduce recurrence. 4
Past research has suggested a variety of surgical approaches for subungual bone tumor excision. 2 A direct approach through the nail bed, and lateral and volar side approaches of the distal phalanx have been proposed. 5 However, gaining sufficient tumor exposure is difficult with these methods; further, the nail bed could be damaged during these types of procedures. To obtain sufficient tumor exposure, a fish-mouth-type incision approach that involves elevating the nail bed and surrounding tissues has been proposed. 6 However, this method cannot be applied to cases with large-sized tumors or cases where the nail bed is already damaged. It also leaves a longitudinal incision scar along the lateral nail fold which some patients find cosmetically unacceptable. In addition, the fish-mouth-type incision might cause sensory impairment of the fingertip. Therefore, alternative surgical approaches, which could overcome those shortcomings, are necessary to improve surgical outcomes associated with subungual bone tumors.
Herein, we describe a modified proximally based nail bed flap approach to remove benign bone tumors in the subungual area. We also present cosmetic and functional outcomes associated with this surgical approach.
Materials and methods
Participants
This retrospective cohort study examined the clinical records and medical photos of 24 phalanges of 23 patients (9 males and 14 females) with subungual bone tumors, from October 2013 to September 2017. We included patients who (1) were diagnosed with a subungual bone tumor (Figure 1), (2) underwent preoperative magnetic resonance imaging (MRI) or computed tomography (CT) (Figure 2), (3) underwent tumor excision using the modified proximally based nail bed flap approach, and (4) were followed up for more than 1 year. Patients with malignant subungual tumors or histories of previous subungual tumor removal were excluded. In all cases, because the preoperative MRI or CT suggested benign subungual bone tumors, we did not perform diagnostic biopsy before surgery.

(a) Clinical photograph of case number 7 (11-year-old boy with subungual exostosis). (b) and (c) Preoperative posteroanterior and lateral radiographs of the left second toe, which showed a mass on the dorsal surface of the distal phalanx (white arrows).

Preoperative MRI images of the left second toe in case number 7. (a) T1-weighted axial image shows low-signal-intensity lesion at the distal end of the distal phalanx (white arrow). (b) T2-weighted axial image shows low-signal-intensity lesion (white arrow), and medullary continuity was not observed between the distal phalanx and the lesion. MRI: magnetic resonance imaging.
The research protocol was conducted in compliance with the Helsinki Declaration and approved by the Institutional Review Board of the University Hospital (IRB No.: 1809-052-971) on September 2018, and the requirement for informed consent was waived because this was a retrospective study.
Surgical procedures
All operations were performed by a single hand surgeon. Under general or local anesthesia, a rubber band tourniquet was applied on the involved digit. The nail plate was first removed from the nail bed (Figure 3(a)) and kept in soaked gauze for insertion after tumor removal. A proximally based fish-mouth-type incision was made on the nail bed, a lateral incision was made inside the lateral margin of the nail bed, and a distal incision was made at the junction between the nail bed and the skin. The nail bed flap was carefully elevated from the dorsal periosteum of the distal phalanx using a #15 Scalpel blade (Figure 3(b)). After the elevation of the nail bed flap, the exophytic portion of the main tumor mass was firstly removed using a micro-oscillating saw. In cases with exostosis, the margin of the main mass was additionally excised until the normal cancellous bone was revealed (Figure 4). To prevent tumor recurrence, additional adjuvant treatment using a high-speed burr and electrocauterization were conducted on the surface of the remaining medullary bone after tumor removal. After those procedures, the elevated nail bed was repaired using 6-0 absorbable monofilament sutures (Monosyn®; Aesculap Inc., Tuttlingen, Germany) (Figure 5(a)). In cases where the nail bed was damaged, the torn nail bed was repaired and then the nail bed flap was sutured. Finally, the nail plate was reinserted to protect the repair site and to prevent dressing gauze from sticking to the repaired nail bed (Figures 5(b) and 6).

Intraoperative clinical photograph after nail plate removal. (a) A modified proximally based nail bed flap incision line was drawn on the nail bed. (b) The nail bed flap was elevated.

(a) Subungual exostosis was removed using a sagittal saw and rongeur. (b) Clinical photo after removal of the subungual exostosis.

(a) The nail bed flap was repaired using absorbable sutures. (b) The nail plate was inserted and fixed with sutures.

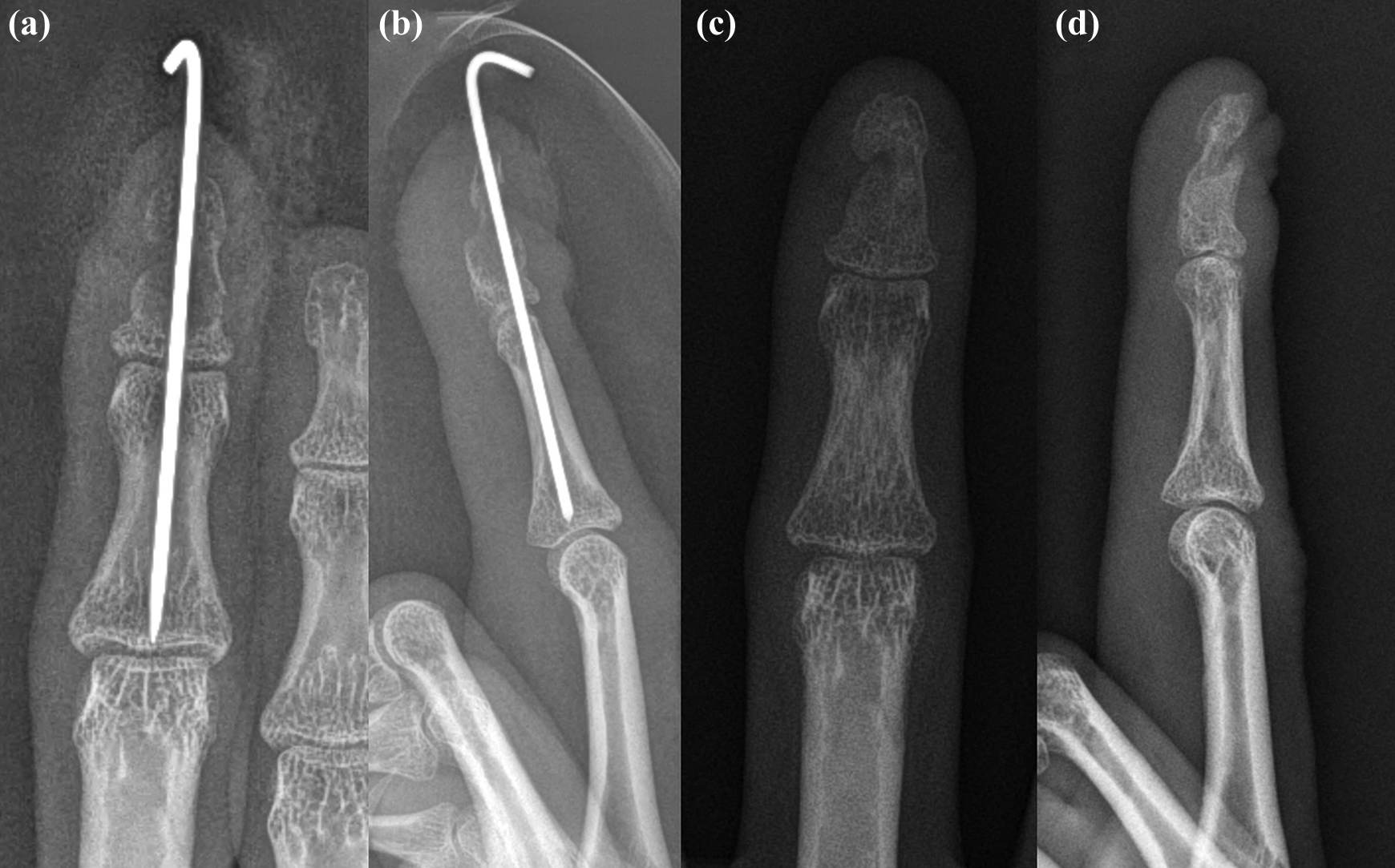
(a) and (b) Posteroanterior and lateral radiographs taken 1-month postoperatively showed successful removal of the tumor. (c) and (d) Partial onycholysis was observed 6-month postoperatively.
When the tumor developed in the medullary cavity, such as enchondroma (Figures 7 to 9), a small rectangular-shaped cortical window was made using an oscillating saw to approach the tumor mass (Figure 10(a)). The rectangular cortical window was soaked in absolute alcohol (95% alcohol). The tumor mass in the medullary cavity was removed using a small curette and rongeur (Figure 10(b)). In these cases, we firstly evaluated the cortical breakage using saline injection into the medullary cavity. If there was no leakage of the saline, we injected absolute alcohol into the medullary cavity to eradicate the remnant tumor cells. The empty space was filled with the allo-bone material and covered with the rectangular cortical bone after washing it with saline (Figure 10(c)). If pathological fracture was combined, a Kirschner wire was inserted for 4–6 weeks to maintain the reduction and to facilitate bone healing (Figure 10(c)).

(a) and (b) Preoperative anteroposterior and lateral radiographs of a 24-year-old female with enchondroma. An ovoid osteolytic lesion with fracture was observed at the distal phalanx of the right third finger (white arrow). (c) Clinical photo was taken at the same time point.

(a) Intraoperative clinical photo after nail plate removal. A modified proximally based nail bed flap incision line was drawn. (b) Illustration of the surgical incision line on the nail bed

(a) After elevation of the nail bed flap, the dorsal cortex of the distal phalanx was widely exposed. (b) Illustration showing the elevated nail bed flap and exposed subungual tumor.

(a) A rectangular window was made on the dorsal cortex of the distal phalanx. (b) The tumor mass in the medullary cavity was removed using a curette. (c) The fracture was fixed with Kirschner wire and the allo-bone graft was impacted.
Measurements of clinical outcomes
Clinical outcome measurements included self-reported pain scale, self-assessment of cosmesis, and sensory tests. We evaluated pain severity and self-assessed cosmesis preoperatively and 1 year postoperatively. Participants were asked to assess subungual tumor-related pain using a numeric rating scale (NRS) from 0 to 10, with higher scores representing more severe pain. Self-assessed cosmesis was scored using a visual analog scale (VAS, 0–10, with 10 indicating the worst imaginable appearance). Sensation of the digit tips was measured by static and moving two-point discrimination (TPD) tests using the AxoTouch® two-point discriminator (Axogen, Inc., Alachua, Florida, USA) and Semmes–Weinstein monofilament (SWM) test using the Baseline® Tactile™ monofilaments composed of 20 filaments (Fabrication Ent, Inc., Elmsford, New York, USA) at 1 year postoperatively. Both the TPD and SWM tests were performed on both the involved digit and the opposite-side digit. The stimulus intensity during the static and moving TPD test was determined as a stimulus that participants received as constant touching or moving, but no discomfort or pain. 7 The two-prong pressure was distributed simultaneously and equally and the static TPD test was performed at the center of the fingertip. The moving TPD test was performed along the volar side of long axis of the distal phalanx, from proximal to distal. The SWM tests were performed by placing the monofilaments perpendicular to the affected tip of the finger or toe and applying a force sufficient to bend the monofilament. The patients were blinded to the SWM sites, and the stimulation was applied for 1.5 s. Because the tactile sensitivity of the fingertip is different from that of the toe tip, we graded the size of the filaments measured during the SWM test as normal, diminished light touch, diminished protective sensation, loss of protective sensation, and deep pressure sensation only, depending on the thresholds of the fingertip and toe tip, respectively, 8,9 and calculated the percentage of patients with above-normal thresholds. Additionally, we evaluated postoperative complications including postoperative nail deformities and tumor recurrence at 1 year postoperatively.
Statistical analysis
A Shapiro–Wilk normality test showed that the data were nonnormally distributed; therefore, nonparametric tests were used. The Wilcoxon signed-rank test was used to compare pre- and postoperative NRS for pain and VAS for self-assessed cosmesis. We compared the results of static and moving TPD tests, performed on involved digits and opposite-side digits, using the Wilcoxon signed-rank test. The Fisher’s exact test was used to evaluate the different grades of the SWM between the involved digit and the opposite-side digit. The level of significance was set as p < 0.05. All statistical analyses were performed using IBM SPSS ver. 23.0 (IBM Co., Armonk, New York, USA).
Results
The average age at the time of surgery was 20.4 ± 14.6 years (range 6–54 years), and the average follow-up period was 18.21 ± 7.45 months (range 12–37 months). The tumors occurred on fingers in 17 cases (71%) and on toes in 7 cases (29%). Nail deformities were observed in 22 cases (Table 1).
Patient demographic data.
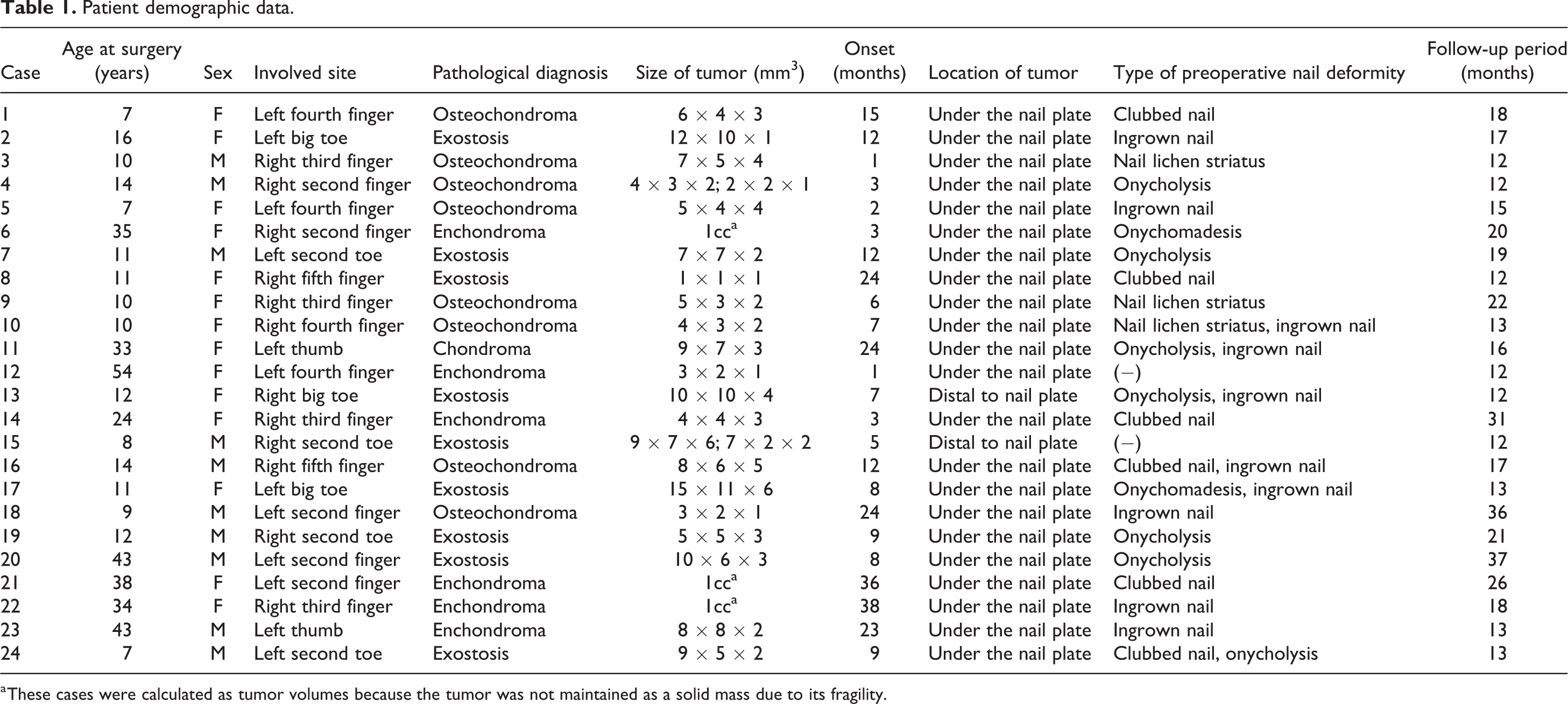
a These cases were calculated as tumor volumes because the tumor was not maintained as a solid mass due to its fragility.
Of the 24 benign subungual bone tumors, pathological diagnosis revealed 8 cases of osteochondroma, 9 cases of exostosis, 6 cases of enchondroma, and 1 case of chondroma (Table 1). There were 13 cases that presented with preoperative nail bed injuries (54%).
The mean NRS for pain significantly improved from 4.1 ± 3.4 before surgery to 0.5 ± 0.8 at 1 year postoperatively (p < 0.05) and the VAS for self-assessed cosmesis also showed significant improvement from 2.7 ± 2.2 before surgery to 7.6 ± 1.8 at 1 year postoperatively (p < 0.05) (Tables 2 and 3). There was no significant difference in mean static and moving TPD distances and SWM grades, between the involved and the opposite-side digits by 1 year postoperatively (Tables 2 and 3). There were 20 cases (83%) who showed better-than-normal sensory thresholds on the SWM test (Table 2).
Assessments of participants’ clinical outcomes.

NRS: numeric rating scale; VAS: visual analog scale; CS: cosmetic satisfaction; TPD test: two-point discrimination test; SWM test: Semmes–Weinstein monofilament test.
a Static TPD tests, moving TPD tests, and SWM tests were performed at 1 year after surgery.
b Postoperative nail deformity and tumor recurrence were also evaluated at 1 year after surgery.
Clinical outcome comparisons.

SD: standard deviation; NRS: numeric rating scale; VAS: visual analog scale; TPD test: two-point discrimination test; SWM test: Semmes–Weinstein monofilament test.
a Descriptive values are shown as mean ± SD.
b p < 0.001 by Wilcoxon signed rank test.
There was one case of tumor recurrence and the recurrence was observed 4 months after surgery. However, because the patient did not have any symptoms and the patient and her parents did not want reoperation, follow-up with 3 months interval was performed without surgical treatment. Of the 22 cases who had preoperative nail deformities, complete improvement was noted in 18 cases. In four cases, the deformities remained; however, they were improved (Figures 5 and 6).
Discussion
Complete tumor removal with nail bed tissue preservation is the most important factor for successful subungual tumor surgery. 2 Residual nail deformities often result in functional digit impairments and may affect patients’ subjective satisfaction with the surgical outcomes. 2,10 Suga and Mukouda reported on patients with nail bed defects that spontaneously recovered or epithelialized following the use of artificial skin. 6 However, in this study, we achieved successful nail bed repair without using any augmentation procedures (Figure 11). If primary nail bed repair is attempted without nail bed flap elevation, approximation of the nail bed defect would be very difficult due to the concentration of tension on the defect site. On the other hand, if the nail bed flap was first elevated, it can be repaired without tension.

(a) The nail bed was repaired with absorbable sutures. (b) Horizontal mattress sutures were used to repair the lateral side, and simple sutures were used to repair the distal side.
In patients with subungual tumors, pain or tenderness of the distal phalanx may result from compression or damage of the nerve adjacent to the tumor mass, but also from iatrogenic nerve injuries sustained during the surgery. These nerve injuries may cause postoperative sensory impairments, which often result in functional impairments including difficulty pinching tiny objects or postoperative loss of fine touch sensation. 11 Due to the communication of the volar and dorsal sensory nerve branches of the distal phalanx, sensory impairment of digit tip is possible even following surgeries that use a trans-nail bed approach. 12 However, no studies have tried to quantify digit tip impairments after the removal of subungual bone tumors. In this study, there were no significant differences in tactile sensation for the static and moving TPD and SWM tests between the involved and the opposite-side digits. No patients complained of the sensory impairments, including numbness or tingling of the digit tip, by 1 year postoperatively. Therefore, the approach used in this study appears to effectively prevent sensory impairment of the digit tip after tumor removal.
The modified proximally based nail bed flap approach has several advantages over the previous proximally based nail bed flap approach. 6 First, the approach used in the present study preserves the blood supply to the lateral side of the nail bed, thereby facilitating healing. The blood supply to the nail bed could be maintained from the lateral side through the radial and ulnar digital arteries (Figure 12). 13 Second, the operative scar is inconspicuously placed under the nail plate (Figure 13). The previous proximally based nail bed flap approach produced a visible scar on the lateral nail fold. The cosmetic VAS in this study showed significant improvement 1 year postoperatively (Figures 14 and 15). In addition, through nail plate repositioning, the nail bed incision and repaired nail bed could be protected. Third, elevating the nail bed flap is technically much easier than the previous proximally based nail bed flap approach. If an incision is made inside the nail bed, identifying the dorsal cortex of the distal phalanx is easier than it would be if the incision was made on the skin of the lateral nail fold. However, the nail bed tissue is very thin and easily torn; we should make an effort not to injure the nail bed tissue, during elevation of the nail bed flap and repair of the nail bed flap after the tumor excision.
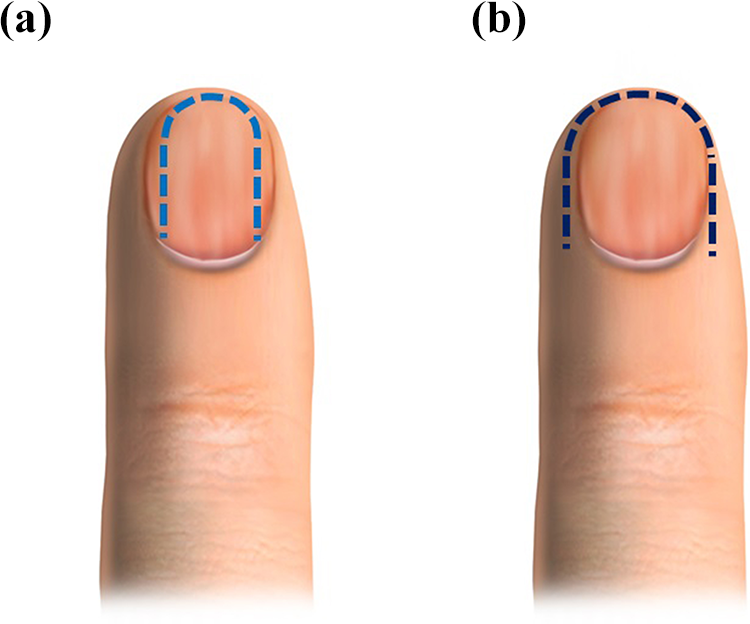
Comparison of the modified proximally based nail bed flap approach and the proximally based nail bed flap approach. (a) Illustration of the incision line in the modified proximally based nail bed flap. The lateral incision was made inside the lateral margin of the nail bed. (b) Illustration of the incision in the proximally based nail bed flap. The lateral incision was made on the skin of the lateral nail fold.
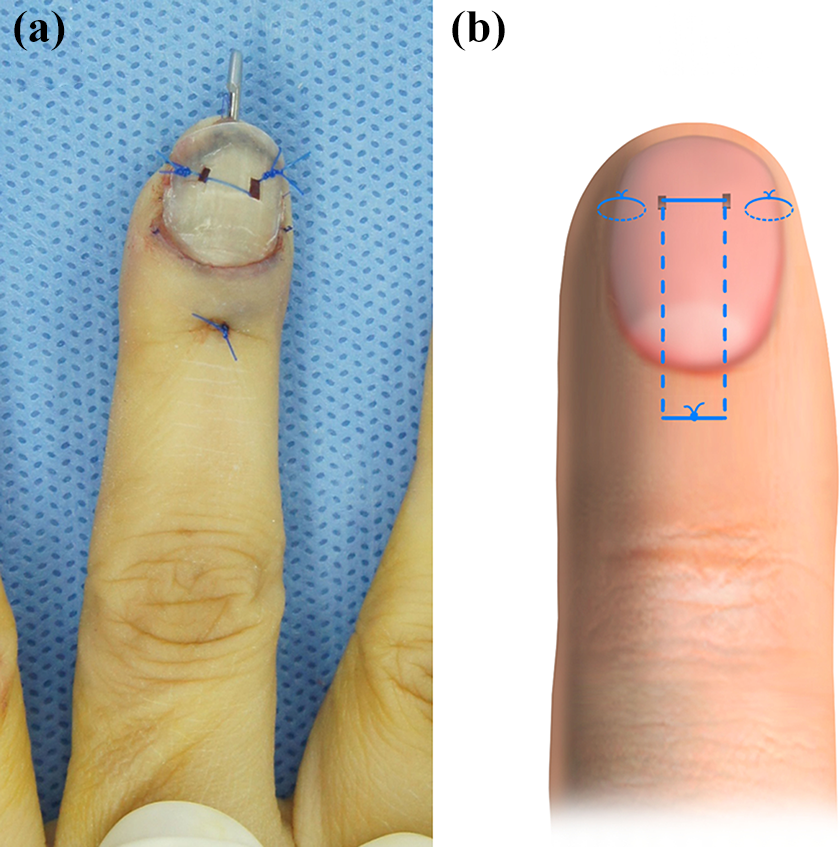
(a) The nail plate was inserted and fixed with nonabsorbable sutures. (b) Illustration of the nail plate fixation method.
(a) and (b) Posteroanterior and lateral radiographs were taken immediately after surgery. Kirschner wire was inserted to maintain the reduction of the pathologic fracture of the distal phalanx. (c) and (d) Posteroanterior and lateral radiographs taken 2 months after surgery showed partial bony union of the fracture.

(a) and (b) Posteroanterior and lateral radiographs taken 6-month postoperatively showed excellent bony union with acceptable alignment. (c) A clinical photo taken at the same time point showed no residual nail plate deformities.
The modified proximally based nail bed flap approach used in this study could provide better and wider exposure of tumor, which enables us adequate removal of the tumor. Furthermore, this approach can be applied to various other conditions of the distal phalanx, including osteomyelitis of the distal phalanx, abscess in the subungual area, or severely displaced fractures that require open reduction. If the volar approach was used for those conditions, sensory impairment might occur due to the iatrogenic damage to the small branches that arise from the digital nerve. 14
This study had several limitations. First, we included benign subungual bone tumors on the toes as well as the fingers. Although the results of this study suggested that pain severity and self-assessed cosmesis improved and phalangeal tip sensation was well-preserved postoperatively, these outcomes should be carefully interpreted. Sensory thresholds and sensitivity of the fingers and toes are different, as are the cosmetic expectation related to these structures. 15 Second, the small sample size reduced the statistical significance of our results. Third, we assessed tumor recurrence at 1 year postoperatively; however, 1 year is a short period to determine tumor recurrence, and it is possible that additional tumors eventually recur.
In conclusion, the modified proximally based nail bed flap approach was a very useful and effective method for excision of benign subungual bone tumors in terms of satisfactory surgical outcomes and low rate of recurrence in the short term. Future studies, with large sample sizes and long-term follow-up are needed, as are studies that compare this technique with other approaches. These investigations will help determine the optimal surgical approaches for treating benign subungual tumors.
Footnotes
Acknowledgements
The authors thank Jongock Choi for his contribution on the schematic drawings that illustrated the surgical procedures.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.