
Abstract
Background:
Data of vitamin D sufficiency in Asian patients with osteoporotic fragility hip fractures are limited. This study aimed to obtain data from the Japanese population.
Methods:
Patients aged 60 years or older with hip fractures were prospectively enrolled. Serum 25-hydroxyvitamin D (25(OH)D) levels were measured. Levels were compared between patients receiving and not receiving treatment for osteoporosis, those with and without previous contralateral hip fractures, and those with femoral neck versus trochanteric fractures. Sex-based differences were also assessed. The serum levels in patients younger than 60 years with extremity fractures were assessed, and differences between elderly and younger patients were evaluated. The individual correlation between 25(OH)D levels and the ultraviolet (UV) index and age was analyzed in elderly patients with hip fractures.
Results:
The data of 360 patients (aged 84.7 ± 8.2 years), comprising 80 men and 280 women, were analyzed. The mean 25(OH)D level was 16.5 ± 7.2 ng/mL. The prevalence of vitamin D insufficiency (25(OH)D <30 ng/mL) and deficiency (25(OH)D <20 ng/mL) was 93.9% and 71.7%, respectively. A significant difference was noted in the prevalence of vitamin D deficiency between patients with and without previous contralateral hip fractures. Age and 25(OH)D levels were found to be correlated, with no correlation between the UV index and the 25(OH)D levels. The 25(OH)D level in the younger population (n = 123) was 20.7 ± 8.6 ng/mL, which was significantly higher than that of the elderly.
Conclusion:
Perennial vitamin D insufficiency is prevalent in elderly Japanese patients with hip fractures.
Introduction
Hip fractures are one of the most serious complications of osteoporosis. Vitamin D is an important regulator of bone metabolism. Hypovitaminosis D is associated with secondary hyperparathyroidism, which increases bone turnover and accelerates bone loss, resulting in an increased risk of fractures. 1 –6 Hypovitaminosis D is also associated with muscle weakness in the lower extremities with consequent poor function and increased risks of falling. This further increases the risk of fracture. 6 –8
Data on vitamin D sufficiency in patients with osteoporotic fragility hip fractures are limited, particularly in Asian populations. 9 –15 The purpose of this study was to examine the prevalence of both, vitamin D insufficiency and deficiency in elderly patients with fragility fractures of the hip in the Japanese population, by estimating serum 25-hydroxyvitamin D (25(OH)D) levels, which is a reliable indicator of vitamin D sufficiency. 16
Materials and methods
Study design
This was a prospective cross-sectional study.
Ethical standards
This study was approved by the institutional ethics committees of the participating institutes. All patients were enrolled after informed consent and were studied in accordance with the principles of the Declaration of Helsinki.
Inclusion criteria
Patients aged 60 years or older, with hip fractures treated surgically at two hospitals between August 2014 and May 2016, were prospectively enrolled. The two hospitals were located in the same prefecture in central Japan. Patients with both femoral neck and trochanteric fractures were included. Femoral neck and trochanteric fractures were diagnosed by reviewing the radiographs. A group of younger patients aged less than 60 years requiring hospitalization for extremity fractures were simultaneously enrolled prospectively. These patients were from five hospitals including the two mentioned hospitals located in the same prefecture in central Japan.
Exclusion criteria
Patients with pathological fractures, bone metastases, atypical femoral fractures, and those receiving vitamin D supplementation were excluded. Elderly patients with hip fractures caused by high-energy injuries were also excluded.
Serum 25(OH)D assay
The remainder of the sera from routine blood examination samples drawn during hospital admission was used for this study. The serum 25(OH)D levels were measured using the radioimmunoassay (DiaSorin, Stillwater, Minnesota, USA). For the purposes of this study, vitamin D insufficiency and deficiency were defined as 25(OH)D levels below 30 ng/mL and 20 ng/mL, respectively. 17 The data on serum 25(OH)D levels were collected, and the mean and standard deviations were calculated; the proportion of patients with insufficiency and deficiency of vitamin D was assessed.
Comparison of 25(OH)D levels
In the elderly hip fracture patients, 25(OH)D levels were compared between those treated and not treated for osteoporosis, with or without previous contralateral hip fractures, with femoral neck versus trochanteric fractures, and in men versus women. The serum 25(OH)D levels between patients aged 60 years or older and younger than 60 years were also compared. The Mann–Whitney U test was used for comparative analyses. A p value below 0.05 was considered statistically significant (two-sided test).
Comparison of proportions of vitamin D insufficiency and deficiency
The proportion of vitamin D insufficiency and deficiency in the elderly patients with hip fractures was compared between those treated versus not treated for osteoporosis, those with previous contralateral hip fractures versus without fractures, those with femoral neck versus trochanteric fractures, and in men versus women. The proportion of vitamin D insufficiency and deficiency was also compared between patients aged 60 years or older and younger than 60 years. The Pearson’s χ 2 test was employed for comparative analyses. A p value below 0.05 was considered statistically significant (two-sided test).
Correlation analysis
Correlation between the 25(OH)D levels with the ultraviolet (UV) index and age was individually assessed among elderly patients with hip fractures. The Spearman’s rank correlation coefficient was employed for the analyses. A p value below 0.05 was considered statistically significant (two-sided test).
Results
Characteristics of elderly patients with hip fractures
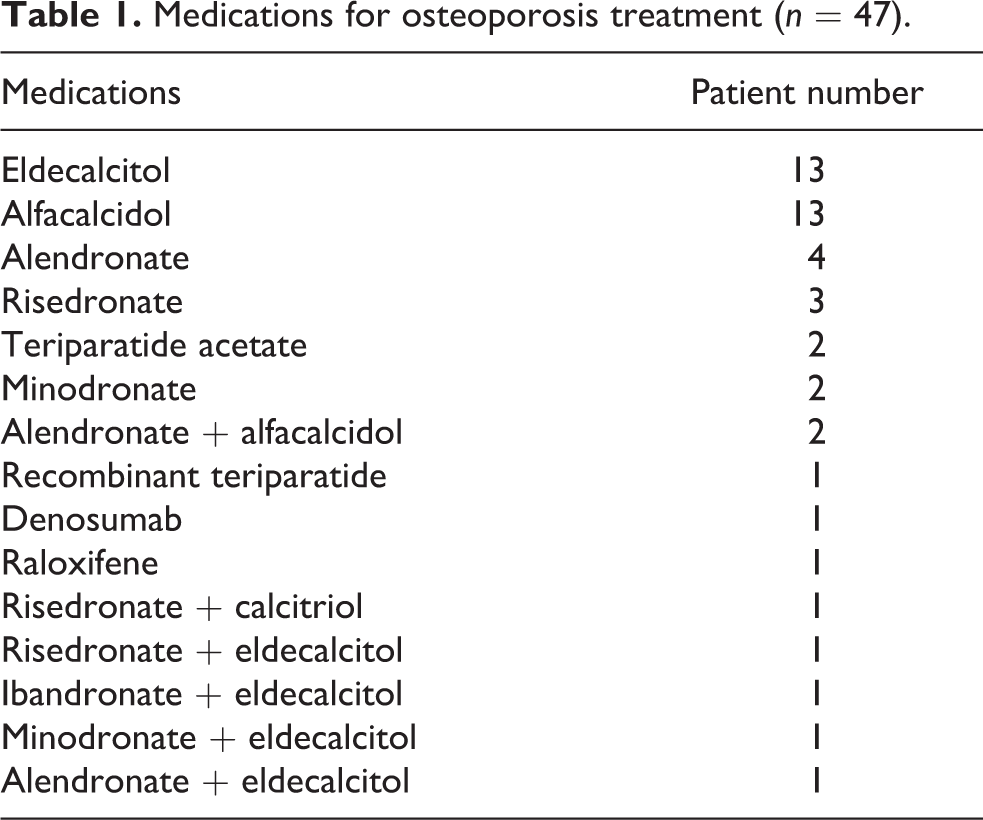
Five and four patients with atypical femoral fractures and pathological fractures owing to bone metastases from malignant tumors, respectively, were excluded. Among the 483 patients enrolled, 360 (74.5%) were aged 60 years or older with hip fractures. The mean age (±standard deviation) was 84.7 ± 8.2 (range 60–101) years. The cohort comprised 80 men (22.2%) and 280 women (77.8%). A total of 144 (40%) and 216 (60%) fractures were femoral neck and trochanteric fractures, respectively; 47 (13.1%) patients were receiving medications for osteoporosis (Table 1). A total of 39 (10.8%) patients had previously sustained a contralateral hip fracture.
Medications for osteoporosis treatment (n = 47).
The 25(OH)D level in the elderly patients with hip fractures
The mean 25(OH)D level was 16.5 ± 7.2 (range 5–44) ng/mL. The prevalence of vitamin D insufficiency and deficiency was 93.9% (338 of 360 patients) and 71.7% (258 of 360 patients), respectively (Table 2).
Data of patients aged ≥60 years with fragility hip fractures (n = 360).
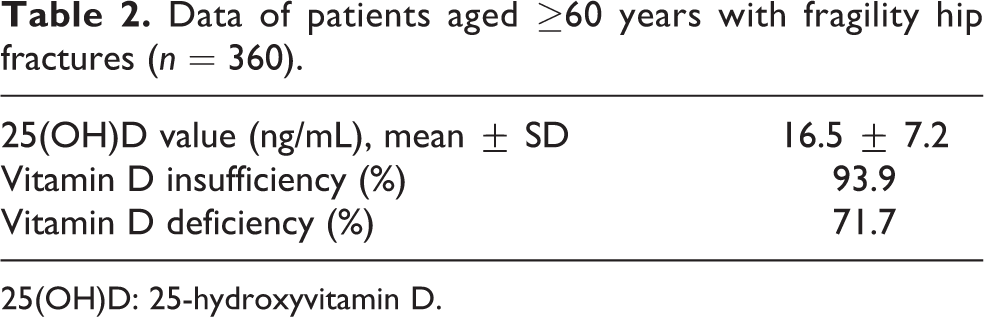
25(OH)D: 25-hydroxyvitamin D.
Comparison of 25(OH)D levels
There were no significant differences in the mean 25(OH)D levels between any of the subgroups analyzed (Table 3).
Analysis of subgroups of patients aged ≥60 years with fragility hip fractures (n = 360).

25(OH)D: 25-hydroxyvitamin D.
a Statistically significant difference.
Comparison of proportions of vitamin D insufficiency and deficiency
There was a significant difference in the prevalence of vitamin D deficiency between patients with previous contralateral hip fractures versus those without fractures (p = 0.024). There were no significant differences in the prevalence of vitamin D deficiency between the other subgroups analyzed; vitamin D insufficiency was also not significantly different between any of the subgroups analyzed (Table 3).
Correlation between the UV index and 25(OH)D levels in the elderly hip fracture patients
No correlation was noted between the UV index and 25(OH)D levels in this group (Figure 1) (p = 0.912).

Scatterplot showing lack of correlation between UV index and 25(OH)D levels. UV: ultraviolet; 25(OH)D: 25-hydroxyvitamin D.
Correlation between age and 25(OH)D levels in the elderly hip fracture patients
A significant negative correlation was noted between age and 25(OH)D levels (p = 0.044, correlation coefficient = −0.106; approximate line y = −0.0828x + 23.528) (Figure 2).

Scatterplot showing correlation between age and 25(OH)D levels. Increasing age was associated with lower 25(OH)D levels. 25(OH)D: 25-hydroxyvitamin D.
25(OH)D levels in the younger patients
The 25(OH)D level in the younger population (n = 123; age 43.1 ± 12.1 (range 20–59) years, comprising 83 men and 40 women) was 20.7 ± 8.6 (range 5–53) ng/mL. This was significantly higher than that of the older population. The prevalence of both vitamin D insufficiency (82.1%, 101 of 123 patients) and deficiency (48.8%, 60 of 123 patients) was also found to be high in the younger population. However, this was significantly lower than the prevalence in the older population (Table 4).
Data of patients aged <60 years (n = 123).
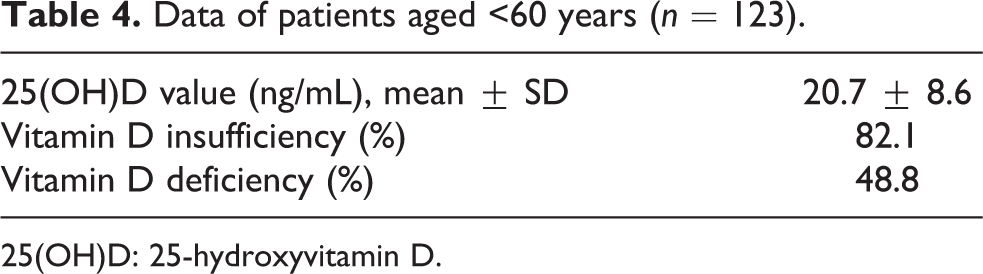
25(OH)D: 25-hydroxyvitamin D.
Discussion
The relationship between serum 25(OH)D levels and hip fractures has been reported in the Western population. 18,19 The 25(OH)D levels in patients with hip fractures are reported to be significantly lower than in controls. Serum levels of 25(OH)D are a linear predictor of major osteoporotic fractures and a quadratic predictor of hip fractures. 20 Reports suggest that lower serum 25(OH)D levels increase the risk of hip fractures (33% increase per 10 ng/mL decrease). 21 Data on the Asian population are limited. An epidemiologic survey conducted in Sado City in the Niigata Prefecture of Japan has shown similar trends as the West. 22 The prevalence of vitamin D insufficiency was reported to be 74% 23 and 39.3% 24 among Japanese patients diagnosed with primary osteoporosis. The prevalence of vitamin D insufficiency in the present study was found to be higher than that of previous reports, suggesting that the fractures resulted from severe osteoporosis. Sakuma et al. reported that the average serum 25(OH)D level and the prevalence of vitamin D deficiency was 16.3 ng/mL and 79.0%, respectively, in 225 Japanese patients with hip fractures. 25 The results of that study were similar to those of the present study.
Among those with osteoporosis, patients with hip fractures have high disease severity. Measures for secondary fracture prevention should be instituted in these patients to prevent subsequent hip fractures. 26 Hagino et al. 26 reported that women aged 65 years or older who had initially sustained a hip fracture were four times likelier to sustain a subsequent episode compared to the general population. The proportion of patients in the present study receiving medications for osteoporosis was low, similar to those of previous reports. 26,27 The occurrence of hip fracture is indicative of osteoporosis. In addition to fixation of the hip fracture in these patients, it is essential to manage osteoporosis. There is evidence of the beneficial effect of risedronate for preventing recurrent hip fractures in elderly Japanese women. 28 In addition, reports have suggested that zoledronic acid administration after hip fractures reduced the rate of new clinical fractures and improved survival 29 and subsequent health-related quality of life. 30 Pharmacological treatment of osteoporosis should therefore be initiated.
The high prevalence of vitamin D insufficiency and deficiency in the elderly patients with hip fractures should be recognized. In the present study, the prevalence of vitamin D deficiency was higher among patients with previous contralateral hip fractures compared to those with no fracture history. Reports suggest that optimal vitamin D repletion is necessary to maximize the response to antiresorptive agents including bisphosphonates, in terms of both bone mineral density changes and anti-fracture efficacy. 31 –34 Major clinical trials examining the effect of zoledronic acid on patients with hip fractures have ensured optimal vitamin D repletion. 29,30 There is also evidence suggesting that hip fractures in elderly women may be prevented by vitamin D and calcium supplementation. 35 The results of the present study and that of previous reports suggest that vitamin D supplementation may be considered in addition to the initiation of osteoporosis medication for elderly patients with hip fractures.
Vitamin D biosynthesis is affected by UV exposure as in sunbathing. The correlation of the UV index and 25(OH)D levels was therefore assessed; no correlation was observed between these variables. This was probably owing to the decline in outdoor activities among the elderly, which considerably reduced sun exposure, leading to perennial vitamin D insufficiency and deficiency.
A correlation was found between age and 25(OH)D levels in this cohort. Increasing age correlated with lower 25(OH)D levels. Tsukutani et al. 36 reported that hip fractures increased with age among patients aged 70 years or over. It has been speculated that decreasing vitamin D sufficiency with age is associated with an increasing prevalence of hip fractures.
Vitamin D insufficiency and deficiency was approximately 80% and 50%, respectively, in younger patients with fractures of the extremities. Steele et al. 37 reported that 25% of younger men sustaining a high-energy fracture are vitamin D insufficient. Hood et al. 38 reported that vitamin D deficiency and insufficiency in acute orthopedic trauma patients aged over 18 years is common. The overall prevalence of vitamin D insufficiency and deficiency was 77% and 39%, respectively. There were no statistically significant age or sex differences in the population. Maroon et al. 39 reported that the prevalence of vitamin D insufficiency and deficiency in 80 young National Football League players was 68.8% and 26.3%, respectively. Manickam et al. 40 reported that prevalence of vitamin D insufficiency in young physicians to be 77%. Reports suggest that vitamin D insufficiency and deficiency are common even in the younger population. The findings of the present study may suggest that 25(OH)D levels should be evaluated in all patients with orthopedic trauma, irrespective of age.
In this study, patients aged younger than 60 years with extremity fractures needing hospitalization constituted a control group for comparison. However, it would be ideal to select elderly patients (aged 60 years or over) without hip fractures as controls, while assessing the impact of vitamin D insufficiency and deficiency on the prevalence of hip fractures.
Conclusion
Perennial vitamin D insufficiency is prevalent in elderly Japanese patients with hip fractures. Further studies comparing the vitamin D status between elderly patients with and without hip fractures will provide more insights into the impact of vitamin D insufficiency and deficiency on the prevalence of hip fractures.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a grant from Zenkyoren (National Mutual Insurance Federation of Agricultural Cooperatives).