
Abstract
Introduction
Hip fracture causes patient significant comorbidities. The history of previous fragility fracture (PFF) might have alarmed clinicians on the imminent fracture risk before the hip fracture occurs. This study is to review the impact of hip fracture on the mobility status in patients with or without history of PFF.
Methods
All hip fracture patients, who were admitted to a regional hospital from July 2022 to June 2024, were recruited. Their demographics data, pre-injury and post-injury 1-year mobility status, 1-year mortality, rates of bone density scan (DXA), and prescription of bone health medication (BHM) were retrieved from clinical record.
Results
336 patients were included. 108 (32.1%) patients were found with history of PFF and 26 (24.1%) of them were having their second hip fracture. All patients, whether with or without history of PFF, suffered from a significant decline in mobility. However, patients without a history of previous fragility fracture (NFF) have better pre-injury (p = 0.010) and post-injury mobility status (p = 0.027). The patients having the second hip fracture (PHF group), despite having better pre-injury mobility status (p = 0.015), had comparable post-injury mobility with the patients without history of previous hip fracture (NHF group) (p = 0.157). 1-year mortality for NFF was higher when comparing to PFF (15.4% vs 9.26%), yet the figure was insignificant (p = 0.139). Reviewing PFF cohort, 30 (27.8%) patients suffered from fragility fracture within 2 years before this episode of injury. 21 (19.4%) patients had history of recurrent fall which required admission. DXA was done and BHM was started in only 18 and 13 patients, respectively.
Discussion and conclusion
Hip fracture causes marked decline in patients’ mobility. Early and structured intervention should be taken for previous episodes of fragility fracture as they alarm the possible upcoming hip fracture, which could cause devastating outcome in terms of functional morbidity and mortality.
Introduction
Hip fracture is a devastating injury for geriatrics patients, which frequently results in significant and long-term health consequences. It is well established that hip fracture causes high burden to the community in terms of comorbidity and functional deterioration of individuals, and mortality. 1 Large prospective and population-based cohort studies reported that older hip fracture patients often present with multiple chronic conditions—including cardiovascular disease, diabetes mellitus, chronic kidney disease, and cognitive impairment—which not only increase the peri-operative risk, but also complicate post-operative recovery. 1-year mortality following hip fracture remains high, ranging from 20% to 30% from the literature, with the highest risk observed during the first 6 months after the injury.2,3
Apart from the impact on mortality, hip fracture leads to considerable functional and mobility decline, which deeply impacts patients’ independence in daily care and quality of life. Only about one-third to one-half of patients regain their ambulatory condition at pre-fracture level, while many are permanently dependent on walking aids or caregiver's support. 4 This loss of mobility correlates closely with a decline in health-related quality of life, particularly in domains related to self-care, mobility, and participation in daily activities. 5 As such, hip fracture often marks a turning point in the trajectory of aging, which subsequently leading to reduced elderly's autonomy, institutionalization, and social isolation.
Before suffering from hip fracture, prior fragility fractures—such as vertebral compression fractures or distal radius fractures—may serve as a sentinel event that indicates underlying skeletal fragility and a heightened risk for subsequent fragility fracture. Literature reported that patients with a history of fragility fractures have a significantly higher risk—up to twofold—of sustaining a hip fracture later, especially if no osteoporosis treatment was initiated after their initial fracture.6,7
In addition to signaling deteriorating bone health, fragility fractures have also been associated with higher comorbidity burden, including osteoporosis, sarcopenia, frailty, and other chronic illnesses. 8 , 9 This presents additional challenges during the peri-operative period of hip fracture patients, as they may have limited physiological reserves to withstand surgery, and more barriers to participating in and benefiting from rehabilitation. These patients are often slower in rehabilitation progress and more likely to have prolonged hospitalization, delayed mobilization, and reduced adherence to therapy. 10
Given the increasing prevalence of both osteoporosis-related fragility fractures and hip fractures among aging populations, there is a pressing need to better understand the intersection between these two conditions. In this study, we aim to evaluate the impact of hip fracture on elderly patients with a prior history of fragility fracture, specifically investigating differences in baseline characteristics, change in mobility status and mortality.
Methods
This is a retrospective cohort study which included all geriatric patients who suffered from hip fracture and admitted to a regional acute hospital, over a 2-year period from July 2022 to June 2024. The study aimed to evaluate the functional and mortality outcomes of hip fracture patients, stratified by the presence or absence of a prior fragility fracture. The study recruited patients at 65 years old or above at time of admission and had sustained a hip fracture classified as either a femoral neck of femur fracture or intertrochanteric femur fracture. To minimize confounding effects from non-operative management, patients who were treated conservatively were excluded from the analysis.
The primary outcome was to review the mobility status and 1-year mortality in all the hip fracture patients and comparing the statistics between patients with and without a previously documented history of fragility fracture. A fragility fracture was defined according to the World Health Organization criteria as a fracture occurring from low-energy trauma, such as a fall from standing height or less. The secondary outcomes were to characterize the types of prior fragility fractures sustained and review the incidence of recurrent fall before the index hip fracture; and to evaluate the coverage of osteoporosis management, which was assessed by whether patients had undergone bone density scanning and whether they had been prescribed bone health medication (BHM).
Data was extracted retrospectively from the hospital's electronic clinical records including medical consultation notes by medical officers, physiotherapist, and occupation therapist. Demographic and clinical variables collected included age, sex, history of previous fragility fracture (PFF) including its anatomical site, history of recurrent fall, mobility status both prior to the hip fracture and at post-injury 1 year, and mortality data at 1 year. Incidence of recurrent fall was counted as any admissions with explicit documentation of fall, which was happened after the first documented fragility fracture episode and before the index injury of hip fracture. While mobility status was categorized into four levels: (1) unaided ambulation, (2) ambulation with a one-sided aid such as a walking stick or quadripod, (3) ambulation with a two-sided aid such as a walking frame or rollator, and (4) being chairbound or bedbound. This categorization was to reflect clinically relevant thresholds of independence and assistive-device dependency.
Results
This retrospective study analyzed 336 patients with hip fractures after excluding 35 patients who received conservative management from an initial cohort of 371 patients. The study population was divided into two groups: 108 patients with a history of PFF (PFF group) and 228 patients without such history (NFF group). Within the PFF group, 26 patients were experiencing their second hip fracture, forming a subgroup designated as the previous hip fracture (PHF) group.
Demographics and mobility status
Baseline demographic analysis revealed no significant differences in age (p = 0.974) and gender distribution (p = 0.055) between the PFF and NFF groups. Both cohorts demonstrated significant mobility decline following the index hip fracture injury. For the PFF group, the proportion of patients who was able to walk unaided or required only one-sided aid before the index hip fracture dropped from 79.6% to 36.1% (p < 0.0001). While for the NFF group, the figure reduced from 89.0% to 45.2% (p < 0.0001). Significant intergroup differences were also observed, with the NFF group demonstrating statistically superior pre-injury mobility status (p = 0.010) and better post-injury mobility performance (p = 0.027) compared to the PFF cohort.
Subgroup analysis comparing the PHF cohort with patients without previous hip fracture history (NHF group) revealed that the NHF group enjoyed significantly better pre-injury functional status (p = 0.015). Surprisingly, despite this baseline advantage, post-injury mobility outcomes showed no statistically significant difference between these subgroups (p = 0.157), that ended up 26.9% and 43.5% of patients able to walk unaided or using one-sided aid for ambulation after 1 year of rehabilitation.
1-year mortality
Thirty-five out of 228 patients (15.4%) died within 1 year after index hip fracture in the NFF group, that the 1-year mortality rate was seen higher than that of the PFF cohort (9.3%), although this finding did not achieve statistical significance (p = 0.424).
Previous fragility fracture characteristics
Among the 108 patients in the PFF group, vertebral compression fracture was the most prevalent PFF (n = 40), followed by distal radius fracture (n = 36), hip fracture (n = 26), proximal humerus fractures (n = 19), pubic rami fracture (n = 8), and rib fractures (n = 5). 30 patients (27.8%) sustained at least one fragility fracture within a 2-year period preceding the index hip fracture, that hip fracture was considered as an imminent fracture.
Secondary prevention and risk factor analysis
Among the PFF group, 21 patients (19.4%) were found with documented recurrent falls resulting in hospital admissions prior to the index injury. Despite the presence of PFFs, bone mineral density (BMD) assessment was performed in only 18 patients (16.7%) and only 13 patients (12.0%) were initiated on BHMs following their initial fragility fracture in the PFF cohort (Tables 1 and 2).
Compare groups with and without history of previous fragility fracture.
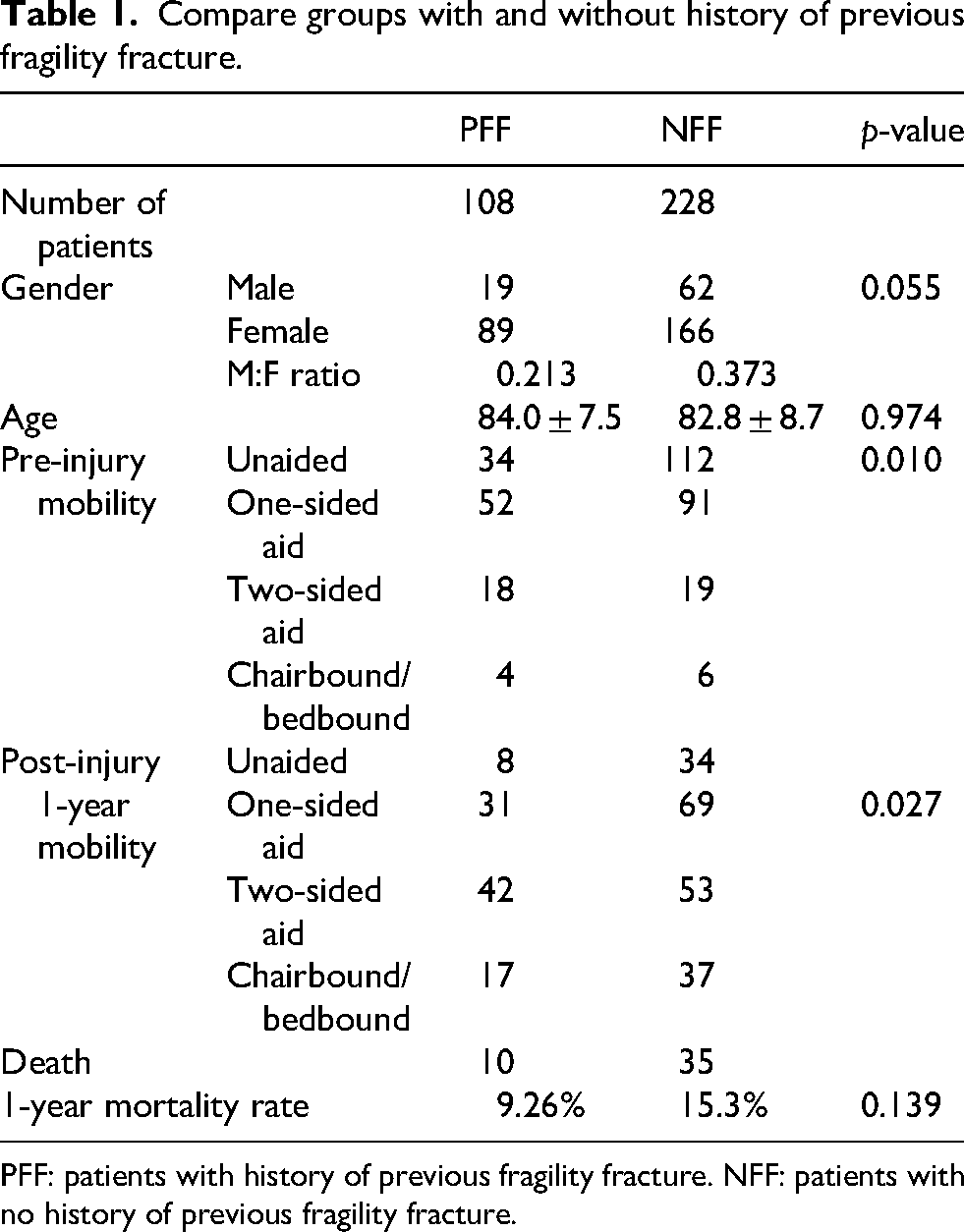
PFF: patients with history of previous fragility fracture. NFF: patients with no history of previous fragility fracture.
Compare groups with and without history of previous hip fracture.
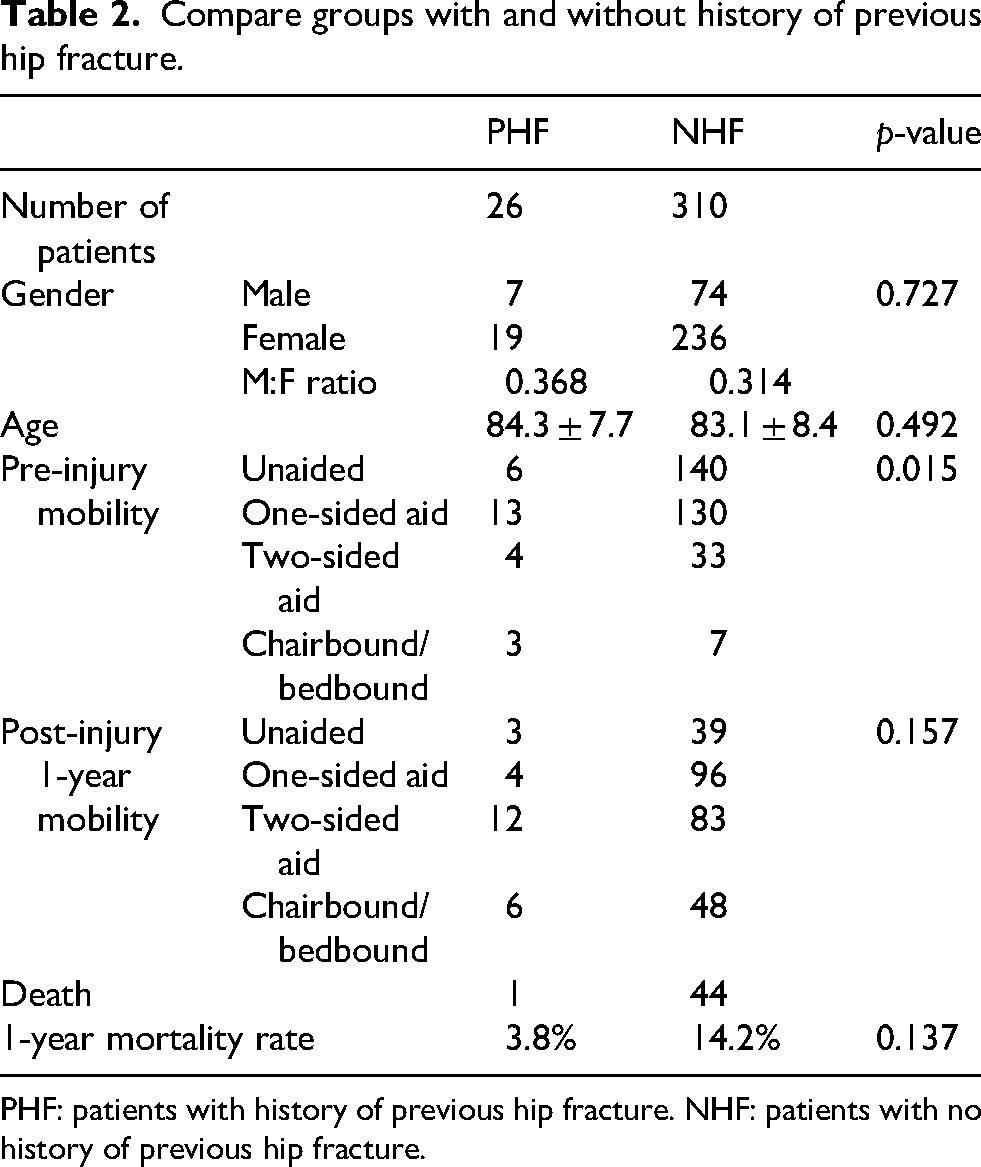
PHF: patients with history of previous hip fracture. NHF: patients with no history of previous hip fracture.
Discussion
This retrospective study delineates the functional and clinical outcomes after hip fractures in patients with and without a prior history of fragility fractures. The findings indicate that individuals with PFF experience significantly inferior pre-injury and post-injury mobility compared to those sustaining their first fragility fracture (NFF). These results highlight the cumulative musculoskeletal and functional deterioration possibly related to prior skeletal injuries.
Functional sequelae of prior fragility fractures
The findings that the PFF cohort demonstrated significantly lower pre-injury (p = 0.010) and post-injury mobility scores (p = 0.027) echo with existing literature identifying prior fragility fracture as an independent predictor of functional decline. Previous studies have attributed this to a compound consequence of osteoporosis-related compromised skeletal integrity, sarcopenia, altered balance, and decreased gait stability. 11 , 12
In our subgroup analysis among patients with and without a history of hip fracture, the findings revealed that patients with a PHF carried a significantly poorer mobility condition (p = 0.015) but exhibited statistically insignificant difference in post-injury mobility outcomes when comparing to those NHF group (p = 0.157). The finding likely reflects the profound functional consequence universally imposed by hip fractures, which often exceed the baseline differences in mobility capacity.
Imminent risk interval
In this cohort, 27.8% of PFF patients sustained their prior fragility fracture within 2 years of the index hip fracture. This temporal proximity supports the concept of the “imminent fracture risk” period, during which the incidence of refracture is markedly elevated. International epidemiological data indicate that approximately 50% of refractures occur within 24 months of an initial event. 7 The clustering of subsequent fractures within this 2-year window provides a compelling reason for quick action in secondary prevention interventions following any episodes of fragility fracture but not only hip fracture. Secondary prevention measures that were taken after incidence of hip fracture would be less meaningful as patients would already be suffering the devastating health impact caused by the hip fracture.
Mortality patterns and interpretive considerations
Contrary to generally reported mortality from literature—which demonstrate 1-year post-hip fracture mortality rates in elderly ranging from 14% to 58% 13 —our cohort identified a lower overall mortality of 13.4%. Meanwhile the 1-year mortality in the PFF group (9.3%) was even surprisingly lower when compared to the NFF group (15.4%), though without statistical significance (p = 0.424). This finding may, in part, be attributable to survivorship bias, wherein patients who survive a prior fracture may represent a relatively robust subset of the elderly patients; whereas patients presented as first-time hip fracture may reflect underlying unrecognized vulnerability.
Persistent secondary prevention gap
A salient and concerning finding was the low rate of osteoporosis assessment and pharmacological treatment among patients with prior fragility fractures. Only 16.7% underwent BMD assessment and merely 12.0% initiated BHM despite the incidence of prior fragility fracture which hinted the underlying osteoporosis. Similar treatment gaps were reported in multinational studies, where fewer than 20% of patients receive osteoporosis therapy after a fragility fracture. 14 , 15 While pharmacological intervention with BHM was shown to reduce refracture rates by up to 44%, 16 it is of utmost importance to start medication soon after identification of fragility fracture. Moreover, almost one-fifth (19.4%) of the patients in PFF group were found with history of admission due to recurrent fall. This group of patients further highlights the deficiency in the comprehensiveness of current fracture risk management strategies.
Clinical and policy implications
Structured post-fracture care pathways are essential to address treatment gaps and huge clinical needs. Attention should be prioritized in incorporating fracture liaison services (FLSs) and multidisciplinary coordination between orthopedics team, primary care, geriatric medicine, and rehabilitation services. FLS models have consistently been showing with increased BMD investigation, higher initiation rates of BHM, reduced refracture incidence, and overall cost-effectiveness.15, 17 Given the predominance of re-fracture within the imminent risk 2-year window and the marked functional impairment following hip fracture, clinicians should raise their awareness in rapid initiation of BHM, referral for fall prevention programs and targeted rehabilitation in hope of preserving the elderly's mobility and independence in daily activity.
Conclusion
Patients sustaining hip fractures with a prior fragility fracture history represent a subgroup of patients with poorer functional status both pre- and post-injury. The clustering of prior fractures within the 2-year imminent risk period, coupled with persistently low rates of osteoporosis evaluation and treatment, underscores critical gaps in secondary prevention of fragility fracture. To address these treatment gaps, well-structured care pathway is necessary to lower refracture risk, preserve mobility, reduce the mortality, and hopefully in a bigger picture, relieve economic burdens associated with recurrent fragility fractures.
Footnotes
Acknowledgements
Special thanks are due to the colleagues of Department of Orthopaedics and Traumatology in Alice Ho Miu Ling Nethersole Hospital for their diligent efforts in data collection.
Ethical considerations and informed consent statements
This is a retrospective study which only involves retrieval of information from existing clinical record. No additional intervention is required. Informed consent is not necessary as only retrospective record review was performed.
The study is approved by Joint Chinese University of Hong Kong-New Territories East Cluster Clinical Research Ethics Committee.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data supporting the findings of this study were not publicly available due to confidentiality and privacy restrictions. The data was retrieved from hospital's electronic record system. All data was encrypted and accessible only to the authors. No new data was generated during this study.