
Abstract
Purpose:
To report 13 consecutive cases of successful triad of anaesthesia, blood and coagulation management (ABC protocol) in haemophilic total joint arthroplasty (TJA) and its feasibility and safety on haemophilic TJA.
Methods:
All the clinical data of 13 consecutive cases were descend from electronic medical record. Patients who suffered from haemophilia A, undergoing primary total hip arthroplasty (THA) or total knee arthroplasty (TKA) with ABC protocol at the academic hospital from December 2014 to November 2018 were included, and demographic, perioperative characteristics according to the classified method were further analysed.
Results:
All 13 haemophilic patients had undergone successful surgery with ABC protocol. No massive blood loss was observed in perioperative period. The mean external blood loss was 876.92 ± 592.86 mL. The mean change in haemoglobin was 5.42 ± 2.43 g dL−1 at 5 days post-operatively. The mean allogeneic transfusion volume was 1.23 ± 1.35 units, and the mean volume of autotransfusion was 237.5 ± 76.93 mL. The average clotting factor consumption for per operated joint was 458.26 ± 226.45 IU kg−1 in all cases. No severe perioperative complications were occurred.
Conclusion:
ABC-related series of measures were appropriate management mode for patients received THA and/or TKA with mild or moderate haemophilia. However, more robust evidence came from larger samples is needed.
Introduction
Haemophilia is a bleeding disorder disease that causes severe arthropathy as a result of bleeding and organization repeatedly during advancing of disease. 1 Total joint arthroplasty (TJA) has been proposed as an alternative operative treatment for functional recovery and enhance the quality of life. 2 However, patients with haemophilia (PWH) received major surgery were associated with numerous risks in perioperative period, particularly high risks of haemorrhage, transfusion-related complications, severe pain, wound infection, deep venous thrombosis and so on. 3 –6
A variety of procedures have been described for integrated measures treatment of reducing blood loss and transfusion, including prefilled coagulation factor, blood salvage, continuous coagulation monitoring and proper use of blood clotting agents. However, their usage is insufficient due to lack of in-depth attention in anaesthesia and analgesia management, in other words, decision-making carried out by anaesthesiologists during perioperative anaesthesia management may play an important role on blood-sparing strategies, especially in those who have special haematic characteristics. A comprehensive and orderly protocol including anaesthesia, blood and coagulation management throughout perioperative period should be advocated, and that also can be multidisciplinary participation.
In this report, we aimed to present our successful clinical practice for patients who underwent total knee arthroplasty (TKA) or total hip arthroplasty (THA) because of terminal stage of haemophilia. The experience came from this case series focused on the triad of perioperative anaesthesia, blood and coagulation management, termed ABC protocol, that includes the identification of those who were most at risk of bleeding, and series of strategies used to minimize risks. Therefore, we assumed that the ABC protocol can be a useful reference for multidisciplinary cooperation in TJA accompany with haemophilia.
Materials and methods
Ethical approval
This study was approved by the ethic committee of our institute (Approval letter No. ZYYECK(2018)149). This study was registered in the Chinese Clinical Trail Registry (ChiCTR1900021917).
Study design
We retrospectively collected 13 consecutive cases of mild or moderate PWH with low responding inhibitors or without inhibitors undergoing primary haemophilic TKA and/or THA using ABC protocol from December 2014 to November 2018. This study is a single-centre case series. The institution is an AAA class hospital located in China.
Perioperative anaesthesia management
The procedure of perioperative anaesthesia management in haemophilic THA or TKA was as follows (Figure 1).

Algorithm of perioperative anaesthesia and coagulation management.
Planning the operation: Involvement of key cooperators
A multidisciplinary team approach was engaged in the entire medical process. The team includes orthopaedic surgeons, anaesthesiologists, haematologists, intensive care specialists, clinical laboratory specialists, transfusion medicine specialists and pharmacists. The team connected through online discussion group (WeChat).
Pre-operative: Optimize patient before surgery
Complete examination before surgery
Current laboratory values (e.g. blood routine, prothrombin time, activated partial thromboplastin time, plasma coagulation factor VIII (FVIII) activity, FVIII inhibitor assay, liver and kidney values and measurements of virus infection) were obtained pre-operatively.
Optimization of pre-operative clotting FVIII concentration
Pre-operative clotting factor replacement therapy was performed at 2 h before surgery by bolus infusion. Pre-intubation and pre-operative desired plasma peak level is 80–100%. 1 Precise dosage was calculated according to pharmaceutical instructions.
Identification of inhibitor risks
Prophylactic history, inhibitor history and the exact species of administrated coagulation factor concentrates were reviewed. FVIII inhibitor screening and assay were settled. A coagulative factor sensitivity test was arranged. The patient was given 15 IU kg−1 FVIII (the same brand planned to use in surgery). Blood samples were obtained at 15 min and 2 h after completion of infusion for plasma FVIII concentration measurement. Results were evaluated by comparing the hypothesized plasma FVIII value and the obtained outcomes. An inhibitor titre of ≥0.6 BU mL−1 or a decline of ≥20% was to be taken as symbol for intervention of advanced haemostatic agents (e.g. the prothrombin complex concentration (PCC) and the recombinant-activated factor VII (rFVIIa)).
Detection of concurrent coagulation disorder
Medications, past and family history and laboratory outcomes were reviewed.
Optimization of RBC mass
Pre-operative anaemia was identified, assessed and treated. Pre-operative autologous blood donation was avoided.
Intraoperative: Minimize blood loss during surgery
Treatment of clotting factor and haemostatic agents
Plasma FVIII peak level was maintained in between 80% and 100% throughout surgery. FVIII assay and coagulation screening tests were measured every 1–1.5 h, depend on the present bleeding speed and surgical process. Dosage was calculated according to pharmaceutical instructions. In TKAs, before deflating the tourniquet, FVIII was infused at least 15 min ahead. PCC or rFVIIa should be put into service and immediate inhibitor assay should be settled if the response of FVIII was suboptimal.
Other haemostasis agents such as tranexamic acid (10 mg per kilogram body weight at the beginning of surgery) and deamino-8-
If FVIII concentrates were unavailable, the alternative choice was cryoprecipitate and fresh frozen plasma (FFP). However, the World Federation of Hemophilia (WFH) supports the use of coagulation factor concentrates in the first place. 1 Secondly, it is general accepted that to achieve FVIII levels higher than 30 IU dL−1 with FFP alone is difficult, and that the safety and quality of FFP and cryoprecipitate are under concern. 1 Cryoprecipitate and FFP should not be taken as conventional choices.
Blood salvage
Intraoperative blood salvage of washed red blood cell (RBC) was applied and reinfused in THAs. Surgical swabs were washed for cell salvage. Acute normovolaemic haemodilution was avoided.
Minimization blood draws
Blood draws was restricted to analysis required volume (not too much nor too little) and should be performed by skilled phlebotomists. The frequency of sampling (including FVIII assays) was under regimentation.
Anaesthesia and fluid management
Anaesthetic tracheal intubation was performed gently by skilled anaesthesiologist. Tracheal tubes with a flexible and soft distal tip (Parker Flex-Tip™ Tracheal Tube, Well Lead Medical Co., Ltd. China) were used to prevent trauma and unwilling bleeding.
Peripheral nerve blocks and central venous catheterization were performed under the guidance of ultrasound by experienced anaesthesiologist. Repeated attempts were avoided.
Controlled hypotension was adopted during surgical procedures. However, blood pressure was adjusted to normal range while suturing deep fascia and subcutaneous tissue to better haemostasis the small vessels.
Fluid heating device and warm air blower were applied for normothermia maintaining.
Strict fluid therapy was employed while circulation system was stable, in order not to dilute the plasma coagulation factor concentration. In choosing the blood substitutes, Ringer’s solution and Gelofusine® were used.
Precise surgical technique and surgical devices that controlled bleeding
Precise pre-operative evaluation, right approach of operation and excellent surgical technique contributed to reducing surgical blood loss. Simultaneous multiple joint elective surgery was considered depending on patient’s opinion, pre-operative erythrocyte stoke, assessed arthropathy status and anticipated blood loss.
Midline skin incision and medial parapatellar approach were used in TKA. Posterolateral approach was used in THA.
Small vessels and bleeding spots in deep fascia and subcutis were precise stanched.
Intraarticular injection of tranexamic acid (tranexamic acid 2 g diluted to 60 mL with normal saline) was applied in both TKA and THA. Intraarticular pressurization was applied in TKA, by intraarticular infusion of normal saline infusion and clamping drainage tube.
Although the use of tourniquet is now controversial, we employed the tourniquet in TKAs. The timing of maintaining inflation was under regimentation of an hour. Tourniquet was deflated after wound closure.
A closed suction drain (Drainobag® Lock 600 K 14, B-Braun, Melsungen AG, Germany) was utilized routinely. Drain vacuum pressure was −80 kPa. Drainage was normally closed but opened in the morning rounds or when haematoma occurred. Drainage was removed at 72 h later or whenever drain output at morning rounds fell below 50 mL.
Post-operative: Maximize blood conservation after surgery
Maintain FVIII concentration
Post-operative plasma FVIII level was maintained at 80–60%, 60–40% and 50–30% in the 1–3, 4–6 and 7–14 days via bolus intravenous infusion. Blood samples were collected before (for dosage calculating) and 15 min after infusion to run FVIII assays and coagulation tests. Inhibitor screening was employed within 4 weeks of the last infusion.
Monitor bleeding and minimize blood sampling
Haemoglobin measurement was done immediately when the patient was sent back to ward. Haemoglobin assessments were accomplished at first day post-operatively and then every 2 or 3 days.
Complete post-operative analgesia
A thorough post-operative multi-modal analgesia programme including opioids, tramadol, peripheral nerve block and intraarticular cavity infiltration was planned. First analgesia doses were applied at 30 min before the end of surgery employing sufentanil (0.2 mg kg−1 body weight) and parecoxib sodium (Dynastat™, 40 mg intravenous administrated). Sufentanil and tramadol were applied in patient-controlled intravenous analgesia (PCIA) pump. Single-shot iliac fascia block (in THA) or femoral nerve block (in TKA) was performed at FVIII activity >80% with 0.33% of ropivacaine. Local infiltration of ropivacaine (75 mg), morphine (5 mg) and triamcinolone (40 mg) was applied in TKA (drugs were diluted to 60 mL with normal saline).
Data analysis
All haemophilic TKAs and THAs procedures were performed by the same orthopaedic surgical team who are experts in joint surgery. Anaesthesia were managed by senior attending physician or above. Data of patient baseline characteristics and surgical-related data regarding number of surgical sites, type of surgery, total operation time, external blood loss (EBL) amount, total blood loss (TBL) amount, allogenic RBC transfusion requirement (in units), autologous RBC transfusion amount (in mL), FVIII concentrates consumption (in gross and in IU kg−1 per surgical joint) and duration of hospitalization were extracted. Data were analysed according to surgical procedures, number of surgical joints and with/without inhibitors. Data were analysed by descriptive statistics and Mann–Whitney test using STATA (version 14).
Pre-operative blood volume was calculated using the Gross formula in male 7 : blood volume = 0.367 × height 3 (m) + 0.032 × weight (kg) + 0.604. TBL was evaluated with the Mercuriali formula 8 : TBL = blood volume × (Hctpre-op − Hctday 5 post-operative) + mL of transfused RBC. The change in haemoglobin was pre-operative haematocrit minus day-5 post-operative haematocrit. Transfusion threshold was 9 g dL−1 of haemoglobin level.
Results
All haemophilic TKA and/or THA employing ABC protocol were completed successfully without exceeding bleeding or unanticipated doses of coagulation factor or bypassing agents. Patients who underwent arthroplasties were all male and mostly with moderate haemophilia (72.7%). Six patients had low responding inhibitors. Five patients did not have inhibitors. Nobody had history of high responding inhibitor (Table 1). The mean age of the patients was 30.85 ± 10.72 years. One patient had diabetes. None of the patients had human immunodeficiency virus, hepatitis B virus or hepatitis C virus.
Patient characteristics.

IQR: interquartile range; SJPS: single-joint procedures; MJPS: multi-joint procedures.
Two patients replaced three joints in two operations respectively. Their data were recorded for each event and they were identified as 4A, 4B and 11A, 11B, which gave 13 cases in total.
There was no substantially increased bleeding over expectation. The median EBL of TKA, THA, TKA + THA, bilateral TKA and bilateral THA were 400, 1330, 1180, 480 and 900 mL, respectively. TBL were 554.05, 1036.78, 2155.18, 517.43 and 900 mL, respectively. The changes in haemoglobin level were 3.6, 3.2, 3.8, 2 and 5.2 g dL−1, respectively (Table 2). Compared to the patients without coagulation disorder underwent arthroplasty in our institute, 9,10 the data of blood loss were mostly excellent (n = 6) or good (n = 5). Two cases were defined as ‘fair’ according to the International Guidelines of WFH. 1 Case 4A (TKA) was a complex knee arthroplasty, and case 7 (TKA + THA) had an anamnestic response of coagulation factor inhibitor during surgery (inhibitor level boosted from 0.5 to 1.9 BU), which explains the excessive TBL of 1806.76 and 3339.46 mL.
Surgical outcomes (median IQR (Q1, Q3).
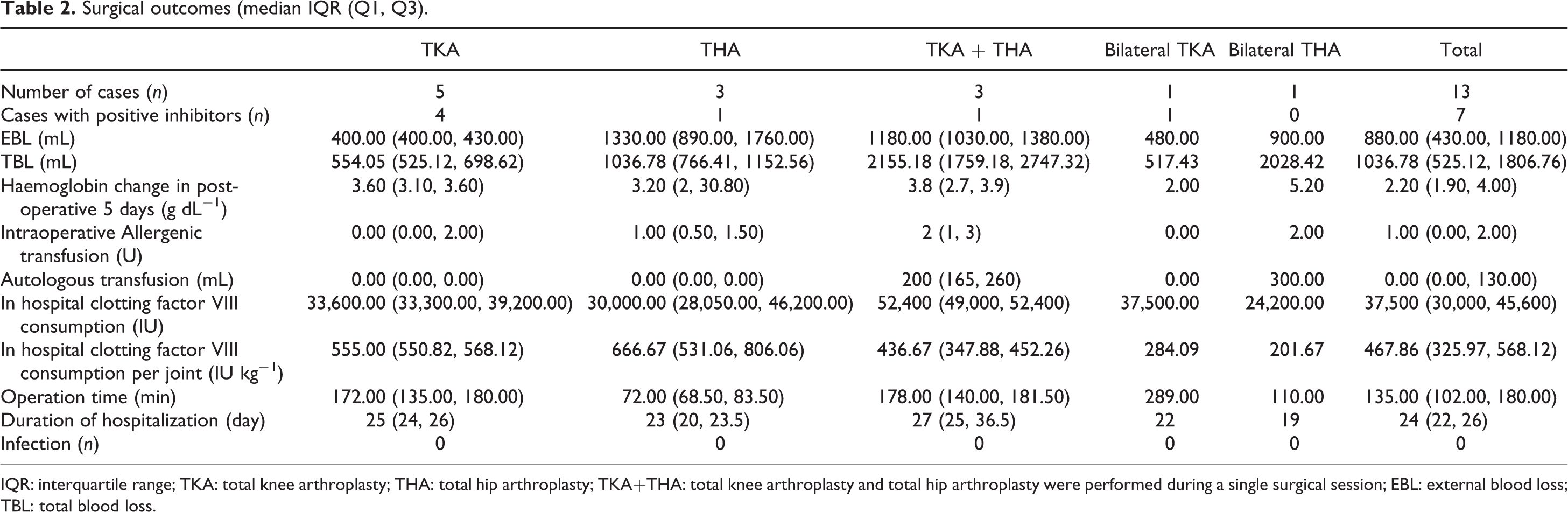
IQR: interquartile range; TKA: total knee arthroplasty; THA: total hip arthroplasty; TKA+THA: total knee arthroplasty and total hip arthroplasty were performed during a single surgical session; EBL: external blood loss; TBL: total blood loss.
The median amount of allogenic RBC transfusion were 0, 1, 2, 0 and 2 units, respectively. The median volume of autotransfusion of THA, TKA + THA and bilateral THA were 0, 200 and 300 mL, respectively. Intraoperative blood salvage was only applied and reinfused in THAs. The median consumption of FVIII concentrates were 33,600 IU (555.00 IU kg−1 per surgical joint), 30,000 IU (666.67 IU kg−1 per surgical joint), 52,400 IU (436.67 IU kg−1 per surgical joint), 37,500 IU (284.09 IU kg−1 per surgical joint) and 24,200 IU (201.67 IU kg−1 per surgical joint), respectively.
There was no need for additional analgesics. All cases were tolerable of multi-modal analgesia programme in the first and second post-operative days. The PCIA pump was removed at the second post-operative day and switched to oral analgesics. At the third post-operative day, two patients felt slightly pain but was tolerable.
There were no post-operative complications (e.g. wound infections, post-operative haematomas and deep venous thrombosis). The median duration of hospitalization were 25, 23, 27, 22 and 19 days, respectively.
All cases were divided into two groups (Table 3): single-joint procedures (SJPS) and multi-joint procedures (MJPS, more than one joint was replaced in single surgical section). The mean operation time was 128.25 ± 44.95 min and 172.80 ± 67.28 min for SJPS and MJPS (p = 0.27). Average TBL was higher in MJPS (1880.74 ± 932.89 mL) than in SJPS (859.97 ± 446.17 mL) but was not statistically significant (p = 0.06). Mean change of haemoglobin was 5.00 ± 2.26 g dL−1 and 6.08 ± 1.00 g dL−1, respectively (p = 0.42). Mean allogenic RBC transfusion volume was 1.00 ± 1.12 units and 1.60 ± 1.50 units for SJPS and MJPS (p = 0.53). However, transfusion rates were higher in MJPS (60%) than in SJPS (50%). As for autologous RBC transfusion, 80% of MJPS received salvaged blood reinfusion with an average volume of 237.50 ± 76.93 mL. Mean FVIII consumption was 36,837.50 ± 11,448.02 IU and 42,420.00 ± 10,634.74 IU in gross, and 580.16 ± 174.70 IU kg−1 per surgical joint and 329.87 ± 103.91 IU kg−1 per surgical joint, respectively, which was statistically significant (p = 0.02).
Comparison of haematological and surgical outcome depending on number of surgical sites (median IQR (Q1, Q3)).

IQR: interquartile range; EBL: external blood loss; TBL: total blood loss.
a Significant difference. A p value of <0.05 was considered significant.
Surgical outcome was then analysed according to the existent of inhibitor (Table 4). The data were divided into no-inhibitor group (inhibitor titre = 0 BU mL−1) and low responding group (inhibitor titre < 5 BU mL−1). The number of cases was 6 and 7, respectively. Hip and knee were 4/4 and 5/5 among the two groups, respectively. Initial FVIII level, number of surgical joint and operation time were not different among groups. No statistical significant was found comparing the two groups.
Comparison of haematological and surgical outcome depending on inhibitors (Median IQR (Q1, Q3)).

IQR: interquartile range; FVIII: coagulation factor VIII; EBL: external blood loss; TBL: total blood loss.
Discussion
Multidisciplinary setting is the insurance to the safety of haemophilic TJA due to the haematic abnormality. Thus, a perioperative protocol consisted of coagulation, blood and anaesthesia is needed for specific multidisciplinary implementations. However, the focus of current protocols, such as that discussed in Chevalier et al. and Wu et al., 11,12 is more about post-operative clotting factor infusion scheme rather than specific anaesthesia and blood management. Studies on the perioperative multidisciplinary issue about PWH are limited.
The experience came from this case series focused on the triad of perioperative anaesthesia, blood and coagulation management, termed ABC protocol, which was appropriate management mode for mild or moderate PWH without inhibitors or with low responding inhibitors received THA and/or TKA. To our knowledge, this is the first haemophilia-related protocol that had integrated three aspects for perioperative management.
Table 5 summarized the surgical outcome of haemophilic TJA in published literatures. In comparison to the previously reported haemophilic TKAs or THAs, our data (Table 2) show lower TBL and allogenic transfusion amount. While comparing to the published studies of TKAs and THAs with ordinary haemostasis in China, 18 –21 our data have a similar TBL outcome.
Surgical outcomes of haemophilia TJA in published literature.

TJA: total joint arthroplasty; TKA: total knee arthroplasty; THA: total hip arthroplasty; NM: not mentioned; HIV: human immunodeficiency virus; Hb: haemoglobin; TBL: total blood loss.
TBL of THA in Table 2 did not match with EBL. This could be the impact of diabetes and related drugs of the patient. That actual blood volume might be affected, which brought a deviation to the calculated TBL and estimated EBL.
Table 3 presents that MJPS appeared to be more efficient on consumption of FVIII concentrates. The mean clotting factor consumption per surgical joint in MJPS was a 42.95% virtual reduction compared to SJPS (p = 0.02). Similar results were also concluded in previous published studies, that MJPS significantly reduces clotting factor consumption per surgical joint by 54%. 22 To determine the influence of simultaneous arthroplasties for blood loss, we analysed the EBL, TBL, volume of transfusion and risk of transfusion according to the number of surgical joint, and no difference was found. Therefore, MJPS helps contribute to increasing clotting factor efficiency without adding additional blood loss and risk of transfusion, if performed with cautious selection of candidates and application of thorough multidisciplinary settings.
Post-operative pain significantly affects post-operative blood loss via two possible mechanism 23,24 : pain-stimulated sympathetic nerve thus increases arterial blood pressure or pain-induced leg contraction thus raises the venous blood pressure of the limb. In this regard, PCIA, peripheral never block and intraarticular analgesic injection were applied in our post-operative analgesia process. Effective pain relief was observed.
Our report indicates that the ABC protocol can be successfully used in patients with low responding inhibitors. The titre of inhibitor had no difference in EBL, TBL and allogenic transfusion volume. However, inhibitor was associated increase possibility of allogenic transfusion. Besides, the two cases with ‘fair’ haemostasis were inhibitors positive with increased inhibitor level post-operatively. The inhibitor may neutralize FVIII, 1 thereby effectively shorten the duration of FVIII, resulting in increased risk of bleeding and transfusion. To those with history of high responding inhibitors, even though inhibitor titre was low or undetectable pre-operatively, anamnestic response may arise when treated again with specific factor products. 1 Therefore, vigilance of inhibitor development is very important for anaesthesia management protocol in haemophilic population.
Wong et al. noted that post-operative clotting factor regime was associated with infection rates. 25 In our study, our post-operative clotting factor regime was based on the WFH guideline 1 and the Chinese Expert consensus 26 According to predisposing factors of infection, 25,27,28 we believe operation time, surgical exposure and intraarticular injection of tranexamic acid and pressurization contribute to zero infection in our study. However, due to the small sample size, further research is still needed.
Our study offers the possibility that the ABC protocol is an appropriated managing mode for mild or moderate PWH without inhibitor or with low responding inhibitors scheduled for primary TKA and/or THA. However, this report is not without limitations. One is that thromboelastography, which allows point of care coagulation function monitoring, was not included in our settings because we do not have one. Also, although rFVIIa were routinely prepared for acute generating inhibitors and uncontrolled massive bleeding, none of the cases in this series had been treated with rFVIIa. Therefore, this study can only provide limited reference for the application of rFVIIa. Furthermore, robust evidence, large samples and long-term follow-up studies are required to completely appreciate the contribution and impact of the ABC protocol.
To the best of our knowledge, this report is the first application of the perioperative triad of anaesthesia, blood and coagulation management of haemophilic TJA. ABC-related series of measures were appropriate management mode for patients received THA and/or TKA with mild or moderate haemophilia and with/without low responding inhibitors. However, more robust evidence came from larger samples was needed.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.