
Abstract
Purpose:
Medical errors are the third leading cause of death in the United States after malignant tumors and cardiovascular disease. Handling of errors becomes more and more eclectic due to the implementation of incident reporting systems and the use of checklists. Since 2015, any German hospital would have a critical incident reporting system (CIRS). The aim of this study is to discover the nationwide utilization and attitude toward CIRS of orthopedic and trauma surgeons.
Methods:
Between April 10, 2015 and May 22, 2015, a web-based questionnaire, which was designed by an expert team consisting of orthopedic and trauma surgeons, aeronautic human factors specialists, and psychologists (Lufthansa Aviation Training), was sent to all members of the German Society for Orthopedic and Trauma Surgery. The survey consisted of three questions regarding CIRS and its use in German hospitals.
Results:
A total of 669 orthopedic and trauma surgeons working in German hospitals completed the questionnaire. All participants rated CIRS as useful, although 71.3% of participants did not report a critical incident in the last 12 months. In that time period, only 13.4% of participating residents reported at least one incident, but 44.7% of chief physicians reported one incident within the same period.
Conclusion:
The present study demonstrates that even though CIRS as a tool is positively appreciated by orthopedic and trauma surgeons working in German hospitals, many do not know about its existence at their own hospital. This can be a reason for the low number of critical incidents reported.
Introduction
As the World Health Organization (WHO) pointed out in 2005, in their draft guidelines for adverse event reporting and learning systems, “The most important knowledge in the field of patient safety is how to prevent harm to patients during treatment and care.” 1 Independent of this, medical errors are the third leading cause of death in the United States after malignant tumors and cardiovascular disease. 2
One common definition of error is “action or inaction leading to deviation from team or organizational intentions.” 3 As such, it has become clear that errors do not only mean incidents leading to patients’ deaths but anything that does not happen exactly as planned. The handling of these errors becomes increasingly more unbiased due to incident reporting systems and the use of checklists. 4 The WHO highlighted that “the primary purpose of patient safety reporting systems is to learn from experience.” 1 Draft guidelines for adverse event reporting and learning systems were published in 2005. 1
There is ongoing research about critical incident reporting systems (CIRS) 5 that (i) consist of publications about implementing CIRS in the context of a single hospital or a single department 6 –8 and (ii) consist of nationwide projects such as the Australian Patient Safety Foundation, 9 the Taiwan patient safety reporting system, 10 and the German project “Every error counts.” 11
On the other hand, common barriers for reporting of critical incidents are known to most medical personnel: for example, the fear of blaming someone, the lack of organizational support and knowledge about the system, and inadequate engagement of clinicians. 5,12,13
Since December 2015 in Germany, the implementation of a CIRS is mandated. 14 In this context, critical incidents are defined as “An event that increases the risk of the occurrence of a serious adverse event or that actually results in a serious adverse event. A critical event requires immediate investigation and response,” 15 according to the Whitebook on patient safety published by the German Coalition for Patient Safety. Examples for critical incidents include preoperative labeling of the wrong side or incorrect dosage of medication due to transmission errors. 16
Still, the acceptance and use of CIRS is largely unknown. As stated, the aim of this study was to discover the nationwide utilization and attitude toward CIRS of orthopedic and trauma surgeons.
Materials and methods
Questionnaire
We performed a literature review with the search terms “human factors, patient safety, and medical errors” in PubMed. Publications from 1995 to 2015 were included and reviewed. Based on these results, an expert team consisting of orthopedic and trauma surgeons, aeronautic human factors specialists, and psychologists (Lufthansa Aviation Training) designed a questionnaire, 17 which was sent to 10 orthopedic and trauma surgeons, who were not involved in the questionnaire’s design. Based on their comments, the questionnaire was revised to encompass intelligibility and completeness.
Survey
Between April 10, 2015 and May 22, 2015, the web-based survey was conducted with SurveyMonkey® (Palo Alto, California, USA). All members of the German Society for Orthopedic and Trauma Surgery were invited to participate via e-mail, with exception of those members who were retired or were working abroad at that time (n = 7573). The first invitation was sent on April 10, 2015, a reminder sent 1 week later, and then another on May 11, 2015.
The survey consisted of three questions regarding CIRS and its use in German hospitals (Table 1). Furthermore, basic data, such as age, sex, and stage of advanced professional training, were acquired. In the German medical system, the stages of professional training are defined as follows: a resident is a medical graduate engaged in specialized practice under supervision in a hospital. Residency to become a consultant in orthopedic and trauma surgery lasts at least 6 years. During this time, residents are supervised by the deputy physicians or chief physician. The resident has to fulfill a catalog of advanced training including certain numbers of different surgery. Furthermore, the resident has to pass a board examination to become a consultant/specialist.
Questions regarding CIRS: Shown as questions and associated selection options.
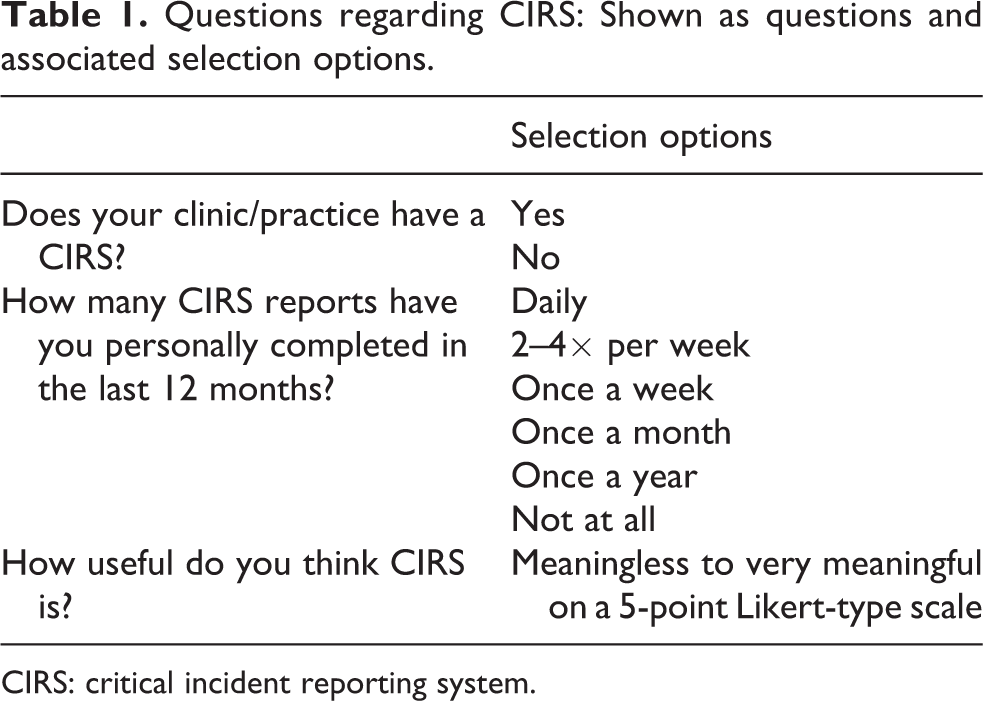
CIRS: critical incident reporting system.
A deputy physician is defined as a consultant surgeon in managerial capacity working in a hospital. Due to his/her competency, he/she takes responsibility for a circumscribed area of responsibility, for example, award, supervising several subordinated residents. The chief physician holds the responsibility for a complete department/center.
Statistical analysis
Digital data allocation was performed using SurveyMonkey. All results were collected anonymously and on a voluntary basis. Statistical analysis was performed using Microsoft Excel (Microsoft Inc., Redmond, Washington, USA) and SPSS (IBM, Armonk, New York, USA). Gaussian distribution was verified using the Kolmogorov–Smirnov test. To analyze differences among the groups, the mean scores from all groups were assessed using the parametric analysis of variance or the nonparametric Kruskal–Wallis test. Significance was recognized when p < 0.05.
Results
A total of 669 orthopedic and trauma surgeons working in German hospital completed the questionnaire (Table 2).
Study participants.

In addition, 76.7% of participants reported that CIRS had been implemented at their workplace (Figure 1).
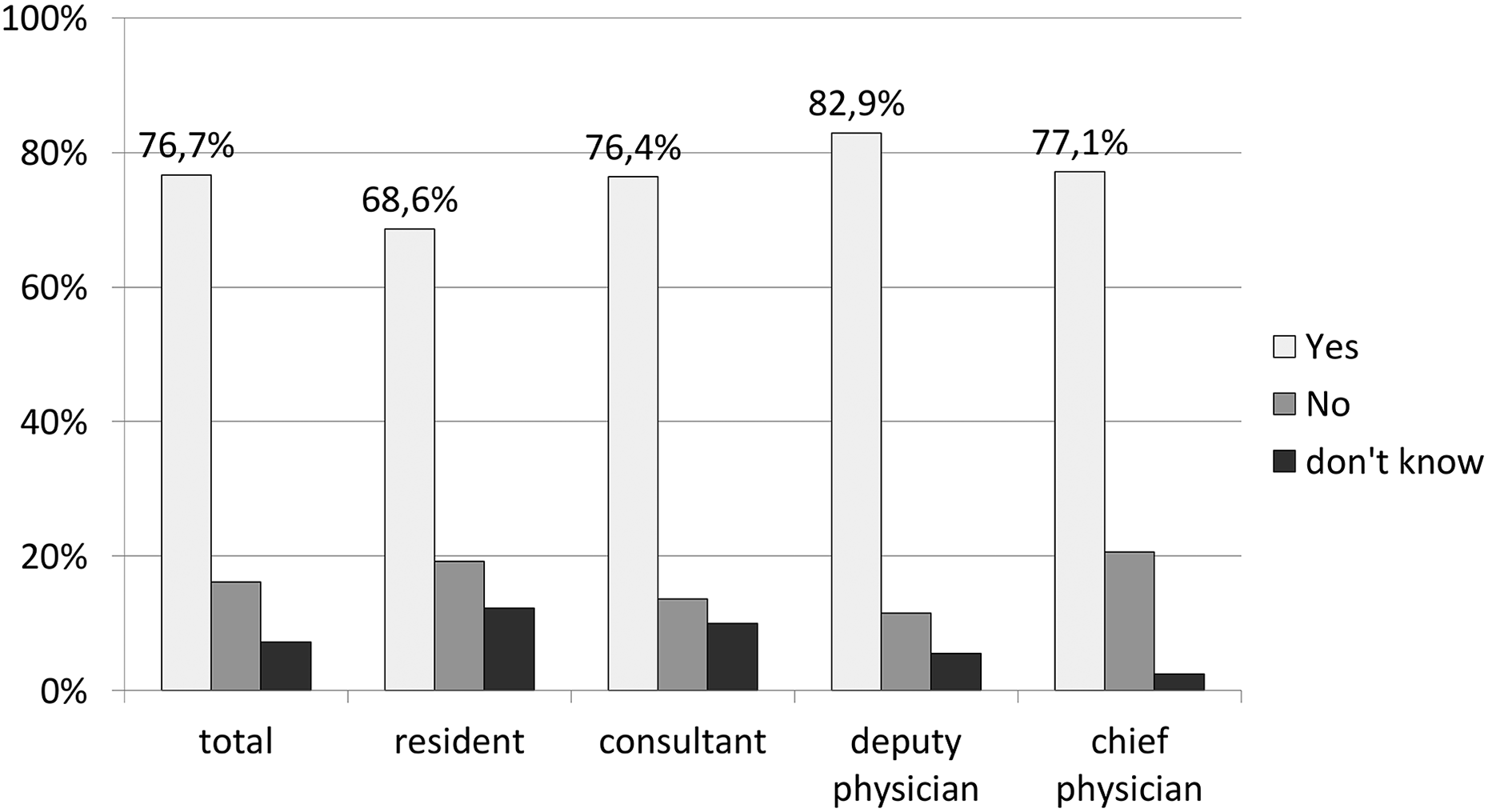
Existence of CIRS at the physician’s own hospital. Participants’ answers to the question of whether a CIRS exists at their workplace. Data are presented as percentage of the respondents answering “Yes” in white, “No” in light gray, and “I don’t know” in black. CIRS: critical incident reporting system.
All participants rate CIRS as useful (Figure 2). Despite this, 71.3% of participants did not report a critical incident in the last 12 months (Figure 3). Only 13.4% of residents reported one incident since then, while 34.6% of deputy physicians and 44.7% of chief physicians reported at least one incident (p < 0.001).

Subjective importance of CIRS. Subjective importance of CIRS was rated by the study participants on a 5-point Likert-scale (from “1” = meaningless to “5” = very meaningful). Data are presented as an average of overall participants and as an average for the different stages of advanced personal training. † p < 0.01. CIRS: critical incident reporting system.
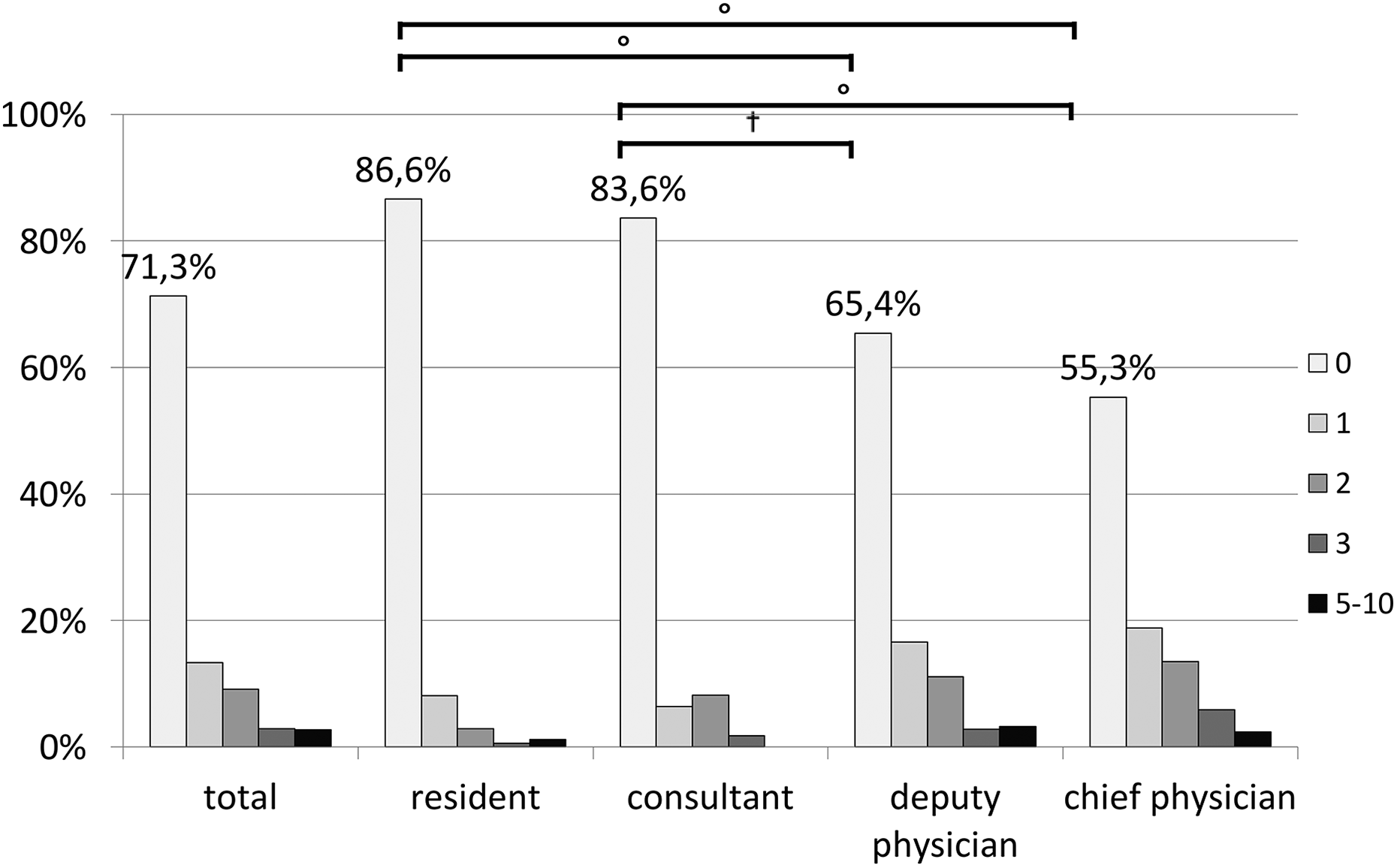
Frequency of personally reported critical incidents in the last 12 months. Participants rated how often they personally reported a critical incident within the last 12 months. Reports are grouped in frequencies from “0” = reported critical incidents (white) to “5–10” = reported critical incidents (black). Data are presented as a percentage for all participants and for the different stages of advanced personal training. °p < 0.001; † p < 0.01.
Discussion
The present study reports the use and attitude toward CIRS of orthopedic and trauma surgeons in Germany.
Study participants rated CIRS as meaningful. Similar results could be found in both national 18 and international studies for health-care workers. 19 And not only physicians rate CIRS as a useful tool: 60% of patients who believe that it is important to encourage medical doctors to openly admit and report medical errors. 20 Valentin et al. demonstrate that the number of errors in medication was significantly lower in hospitals in which CIRS was implemented. 21
Unfortunately, the present study revealed that one-quarter of all study participants and 31.4% of the residents reported that there is no CIRS functioning at their clinic or that they do not know if there is one, despite that since 2015, all German hospitals are supposed to have incorporated this system. 14 Thus, we were able to demonstrate a difference between the positive appreciation of CIRS and the knowledge of its existence and implementation in participants’ workplace. Thereby, our study results suggest that the implementation of CIRS should be better communicated within the medical system. This could be a reason for the low number of incidents reported by the study participants: more than 70% of them did not report a critical incident in the last 12 months. Similar results were found by George et al. in Malaysia. Only 44.8% of the medical doctors and pharmacists in their study had experience using medical error reporting systems. 22
It is important to keep in mind that even though there is a low rate of incidents reported, this does not mean that only few incidents do really happen. Sari et al. showed that in the case note review by trained professionals, 303 patient safety incidents were found during an analysis of a total of 1006 admissions in a large hospital trust in England, while only 54 were recorded by the reporting system. 23 These results differ from those of other health-care professions: Jember et al. demonstrated that the portion of medical error reporting among nurses in Ethiopia was 57.4% with a higher reporting rate in female than in male nurses. 24 Keeping this in mind, further studies should analyze the use of CIRS among all health-care providers who are involved in patient care in orthopedics and trauma surgery.
In the present study, residents reported significantly less critical incidents than other participants: 86.6% of them did not report a critical incident in the last 12 months. Even if chief physicians report a significantly higher number of incidents, less than 50% of them had reported an incident during the last 12 months. At the same time, Münzberg et al. demonstrated that errors occur significantly more often for residents than for chief physicians. 17 One possible reason for these divergent results was published by Hooper in 2015: in their focus group interviews, junior physicians pointed out that even with their positive attitudes toward CIRS, one common parameter that exerted a negative influence on attitudes toward CIRS was limited leadership by senior clinicians and a lack of exposure to role modeling. 25 This could be one possible reason for the low number of residents reporting incidents in the present study: the number of consultants who reported at least one incident in the last 12 months was only 3% higher than the number of residents. Therefore, it can be assumed that the role models for a meaningful use of CIRS are missing among orthopedic and trauma surgeons in Germany.
Additional barriers resulting in less incident reports included inadequate knowledge about what and how they should be reported, 25 too little feedback, no visible action based on them, 12,25,26 and concerns about departmental or professional sanctions, as well as getting someone in trouble. 19
Based on this and the results of the present study, the way in which critical incidents are handled should be increased among physicians. This is even more important as physicians and patients find that CIRS is extremely useful. Hooper et al. demonstrated that junior doctors find that engaging in CIRS (starting with early education) was a crucial part of the cultural change. 25 This is supported by the results of Donnelly published in 2015; due to the implementation of six plan–do–study–act cycles, the number of reported incidents should be increased by 100%. The cycles focused on increasing the degree of awareness of CIRS by establishing a definition of critical incidents, information leaflets, posters, and presentations about it, including the implementation of CIRS Training. They held team meetings in which all reported incidents were discussed to provide functional feedback to those who made the reports. 13
In this way, it is clear that CIRS must be used more transparently: examples of this could be critical incident reports in training for health-care professionals as well as in the form of safety alerts or patient safety newsletters. This is the only way in which CIRS can achieve its goal: “Learn from others’ errors.”
Limitations
There are some limitations that have to be discussed. On the one hand, it can be assumed that the answers are influenced by the social desirability of a positive attitude toward CIRS. This is especially important in the question regarding the importance of CIRS. Here, it is possible that the subjective importance of CIRS is overstated. Another possible limitation is that only 699 of the 7573 invitees completed the questionnaire. Here, it would be possible that in the sense of a selection bias mainly participants completed the questionnaire who believe CIRS to be an important tool. It is therefore possible that among all German orthopedic and trauma surgeons, the number of CIRS reports and the subjective importance of CIRS are even lower than among the study participants. Furthermore, it has to be taken in mind that all participants were orthopedic and trauma surgeons. Therewith, study results could not directly be transferred to other medical disciplines. This does not diminish the relevance of the results regarding patient safety in German hospitals; however, further studies have to focus on the acceptance and use of CIRS in other medical disciplines.
Conclusion
The present study demonstrates that even though CIRS as a tool is positively appreciated by orthopedic and trauma surgeons working in a German hospital, many do not know about its existence at their own hospital. This can be a reason for the low number of critical incidents reported. Further studies should evaluate if better communication regarding the existing tools in the hospital could increase the number of reported incidents.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.