
Abstract
Purpose:
The purpose of this study was to assess the outcomes in a series of patients, who underwent cerclage and figure-of-eight tension band wiring using a single titanium cable for comminuted patellar fractures.
Methods:
We describe a modified tension band technique using a single titanium cable to create an ellipsoidal cap structure that combines the circumferential and figure-of-eight wrapping in the fixation of closed Association for the Study of Internal Fixation/Orthopaedic Trauma Association 34C2 and 34C3 patellar fractures. We retrospectively reviewed 25 patients (16 males and 9 females, mean age 54 years) who underwent the described fixation technique between 2015 and 2017. Postoperative function was evaluated using the Böstman score.
Results:
At the mean follow-up of 25 months (range 17–39 months), the mean Böstman score was 27.3 ± 2.6 points (range 23–30). Eighteen patients (72%) had excellent results (score ≥28); seven patients (28%) had good results (score 20–27); and no patients had an unsatisfactory result (score < 20). All surgical incisions healed without major wound complications. Two patients reported minor complications (soft tissue irritation, cellulitis). No patients demonstrated loss of reduction or implant failure during the follow-up period.
Conclusion:
The modified anterior ellipsoidal cap tension band using a single titanium cable created an effective tension band structure in the treatment of comminuted patella fractures. It is a simple operative technique that produced a stable fixation construct, which allowed early functional rehabilitation and weight-bearing with a high rate of excellent outcomes at 2 years after surgery.
Keywords
Introduction
Fractures of the patella account for 1% of all fractures. 1 Based on the anatomical and biomechanical features of the patella, the Association for the Study of Internal Fixation (AO) developed and accepted the technique of tension band wire fixation as the standard of care for patellar fractures. 2 Subsequent modifications resulted in the modified anterior tension band (MATB) technique, which utilizes a stainless steel wire in a figure-of-eight configuration wrapped around two vertical Kirschner wires (K-wires). According to the AO, in comminuted patellar fractures, the MATB technique should be combined with an additional circumferential cerclage around the patella. 3 The two independent wire structures provide cerclage compression and tension band compression, respectively.
Tension-band wiring techniques using a variety of wire materials for patellar fractures have been described with the goal of optimizing fixation while minimizing soft tissue irritation. 4 Alternative materials to stainless steel wires have been proposed to minimize common complications of painful irritation and wire migration. 5 The titanium cable is a biologically inert material and has been widely used in various implants in orthopedic fracture fixation. Evolution of the cerclage cable technology resulted in a crimped cable connection that maintains greater tension and resistance compared to a twisted wire connection. 6 Borrowing from the concept of the MATB, we propose a modified technique of tension band wrapping using a single titanium cable as an ellipsoidal cap (Figure 1) for the treatment of comminuted patellar fractures. Our modification aims to improve the compression function of the tension band in both the static and the dynamic phases.

Abstract representation of the ellipsoidal cap structure, which was constructed by a single titanium cable, with the cable overlying the anterior surface of patellar in an ellipsoidal cap manner.
The purpose of this study was (1) to describe our modified tension band technique and (2) to assess the outcomes in a series of patients who underwent surgical fixation of patellar fractures using this technique.
Materials and methods
This was a retrospective cohort study that was approved by our hospital’s Institutional Ethics Committee. Consecutive patients over 18 years of age who presented with closed comminuted patellar fractures from October 2015 to December 2017 were included for review. All surgical cases were performed by three orthopedic trauma surgeons (CYC, ZXL, and YX).
Surgical technique
The patient was positioned supine on a radiolucent table after induction of anesthesia. A longitudinal midline skin incision was performed from 1 cm above the upper pole of the patella carried caudally to 1 cm below the lower pole of the patella. The structures under the deep fascia were exposed, but the intact peripatellar retinaculum was carefully preserved. The debris and hematoma at the fracture site were thoroughly debrided. The damaged retinacular rents were repaired when appropriate. With the knee in a slightly flexed position, the patellar fracture was reduced and maintained with two-pointed reduction forceps.
Two 2.0-mm titanium K-wires (Synthes, West Chester, PA, USA) were placed across the fracture site to maintain the reduction. The K-wires were typically placed from the smaller to larger segment, using either an antegrade or retrograde fashion, at a level 5 mm below the anterior cortical surface and parallel to the axis of the patella. Intraoperative fluoroscopy with imaging in multiple planes was utilized to confirm an anatomical reduction. Next, the titanium cable (diameter: 1.0 mm, length: 750 mm; Orthopaedic Cable System, Synthes, West Chester, PA, USA) was passed circumferentially around the equator of the patella and tightened to complete the cerclage step. Typically, the passage of the cable was started from the medial and lower pole of the patella. The cable was passed underneath the K-wire through the patellar tendon by the cable passer and extended from 15 mm to 25 mm within the retinacula and was kept taut by hand. Once the cerclage passage was complete, the limb of the cable was not passed across the crimp but passed behind the two K-wires again (Figure 2(a)). This limb was subsequently crossed over the anterior surface of the patella to create a figure-of-eight configuration. The upper and lower poles of the figure-of-eight, which were bound to the K-wires within the quadriceps and patellar tendons, typically shared the same tunnel of the initial cerclage step.

(a) Intraoperative photograph showing that the titanium cable (green arrows) has completed the cerclage and is being inserted into the passer (blue arrows). The cable is then passed through the patellar tendon and underneath the K-wires again, and starting the figure-of-eight wrapping. (b) The titanium cable is compressed by the tensioner after the figure-of-eight wrapping. The fracture reduction, articular congruity, and fixation construct are confirmed by fluoroscopy in the (c) AP and (d) lateral views before crimping. AP: anteroposterior.
Lastly, the titanium cable was passed back through the open hole in the crimp. The knob on the cable tensioner was turned clockwise until the tension reached 30 kg to complete the ellipsoidal cap tension band structure in the anterior part of the patella (Figure 2(b)). The fracture reduction, articular congruity, and fixation construct were confirmed by fluoroscopy before crimping (Figure 2(c) and (d)). The cable was cut as close to the cable crimp as possible. K-wires ends were bent to prevent escape of the cable over the K-wire and cut smoothly. Knee range of motion (ROM) was tested immediately to assess the stability of the fixation, and it was assured that passive flexion of the knee could reach 120°. Final fluoroscopic images were taken to check the reduction and fixation. The arthrotomy was copiously irrigated, and the retinacular tears were closed. The wound was closed in a standard, layered fashion.
Postoperative management
No casts or braces were necessary after the surgery. The skin sutures were removed 2 weeks after surgery. Functional exercises were initiated 24 h after surgery, including quadriceps isometric exercises and active slight knee motion as tolerated by the patient. The patient was advanced to partial weight-bearing or weight-bearing as tolerated when he or she was able to perform a straight leg raise on their operative leg. Full-weight bearing was encouraged when the operation knee can be achieved 90% ROM as in the unaffected side. Anteroposterior and lateral radiographs were obtained on postoperative day 1, then at 3 and 12 months postoperatively (Figure 3). Knee function was evaluated according to the grading scale of Böstman et al. 7 at the final follow-up visit (Table 1). Outcome data were presented using descriptive statistics.

A 19-year-old male patient with right patellar fracture (AO 34C3). (a) AP and (b) lateral X-rays demonstrate the degree of patellar comminution. (c) AP and (d) lateral X-rays were obtained postoperatively, demonstrating the ellipsoidal cap structure. (e) Lateral X-ray at 12 months demonstrate a stable fixation with healed patella. AP: anteroposterior; AO: Association for the Study of Internal Fixation.
Clinical grading scale of Böstman et al. 7

Results
Twenty-five patients (16 males and 9 females) underwent open reduction and internal fixation of closed comminuted patellar fractures using the described technique. The etiology of the injuries included 2 from motor vehicle accidents and 23 from falling injuries. The mean age at the time of surgery was 54 years (range, 18–87 years). There were 10 left-side cases and 15 right-side cases. Based on the AO/OTA Fracture and Dislocation Classification Compendium-2018, 8 there were nineteen 34C2 fractures and six 34C3 fractures. The average time from injury to surgery was 3.6 days (range 1–7 days).
At the mean follow-up of 25 months (range 17–39 months), the mean Böstman score was 27.3 ± 2.6 points (range 23–30; median 27.5; Table 2). Eighteen patients (72%) had excellent results (score ≥28); seven patients (28%) had good results (score 20–27); no patient had an unsatisfactory result (score <20).
Patients’ Böstman scores at the final follow-up.
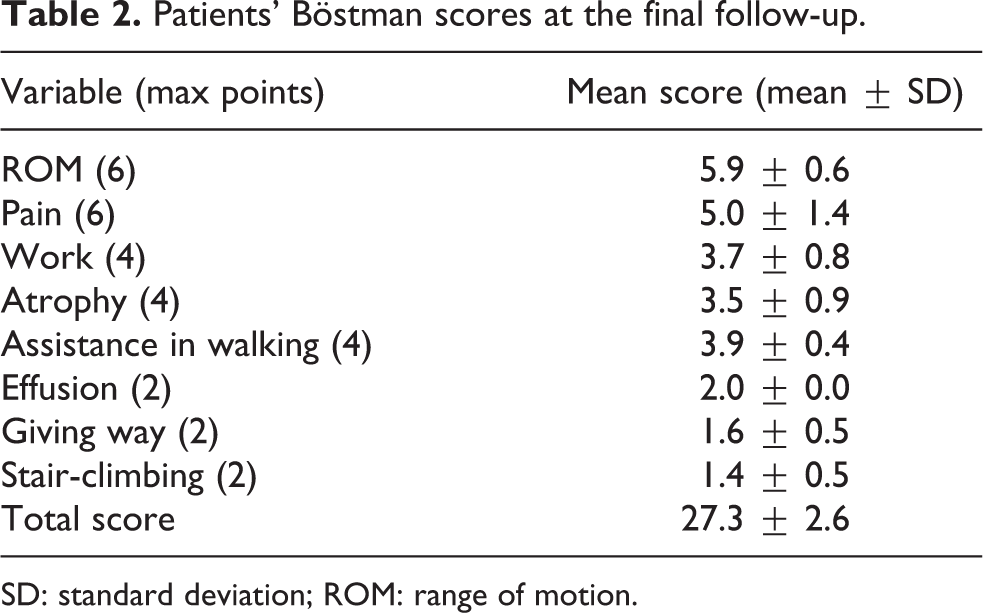
SD: standard deviation; ROM: range of motion.
All surgical incisions healed without major wound complications. Two of the patients reported minor complications from the surgery. One patient (Böstman score of 27) complained of moderate discomfort due to soft tissue irritation in the operative knee 2 weeks after surgery; however, pain resolved by the 3-month postoperative visit without intervention. In the second patient (Böstman score of 27), the incision site demonstrated mild cellulitis by postoperative day 5, and the patient was treated with an oral second-generation cephalosporin antibiotic for 10 days. Sutures were removed 16 days after surgery in this patient, and there were no signs of infection. No patients demonstrated loss of reduction or implant failure during the follow-up period.
Discussion
In this study, we presented a technique using a single titanium cable to create an ellipsoidal cap structure, which replaced the classically described MATB technique involving two independent wire structures that formed the figure-of-eight tension band and the cerclage wire. All patients sustained comminuted patellar fractures according to the latest classification compendium of AO/OTA. 8 At the mean follow-up of 2 years, all patients achieved good-to-excellent outcomes based on the Böstman scoring criteria. Two patients experienced minor complications associated with the surgery, including soft tissue irritation and surgical site cellulitis; however, these did not adversely affect fracture union or final outcomes.
According to the AO principle, the tension band acts to convert tension into compression at the opposite cortex but may not achieve an effective compression as a stable fixation in comminuted patellar fractures. 3 In such cases, the tension band technique should be combined with an additional cerclage around the fractured patella to reduce the gaps in a circumferential manner. Yang et al. 9 modified the AO MATB technique by substituting two stainless steel wires with two titanium cables and demonstrated excellent Rasmussen score (mean 27.9 of 30) at 1 year after surgery. Borrowing from these concepts, our modification aims to improve the compression function of the tension band in both the static and dynamic phases.
During the static compression phase, the AO MATB technique requires two steps: the circumferential wrapping and the figure-of-eight wrapping to build two independent constructs. Because of the two unsynchronized steps, the initial compression effect created by the circumferential wrapping may be attenuated by the subsequent figure-of-eight tension band. In our method, the two steps are performed synchronously while the titanium cable is continuously tightened and crimped. We postulated that the interfragmentary compression could be better achieved via a single step in the formation of the ellipsoidal cap as opposed to two separate steps. With the AO MATB technique, the second compression step may disturb the interfragmentary compression of the initial step, potentially causing fracture displacement. However, this assumption needs to be verified by the biomechanically study.
During the dynamic phase, upon knee flexion, the increased tensile force is converted to compression force at the posterior part of the patella. In the AO MATB technique, the area encompassed by the K-wire and the figure-of-eight wire forms the tension band, which provides a dynamic compression effect. The cerclage wire, on the other hand, mainly plays a role in static compression with less function in dynamic compression when it works independently of the tension band. 10 In our technique, we theorized that the tensile force can be transduced through the entire ellipsoidal cap structure via the single titanium cable, with the cerclage synchronously linked to the tensed figure-of-eight component during the knee flexion. The depth of the cerclage placement may also play an important role. 11 Matsuo et al. 12 described the placement of the cerclage cable in the superficial and deep layers of the patella. Similarly, Yang et al. 13 applied two cerclage cables at one-third and two-thirds of the depth of the patella. We considered that the primary function of the cerclage cable is to reduce the fracture fragments centripetally by holding the retinacula of the patella, and therefore, applied the cable at a depth of 50% in the sagittal plane of the patella.
In our study, we opted for the use of a titanium cable as opposed to a stainless steel wire, although both are commonly used in patellar tension band techniques. Biomechanical studies have demonstrated greater stiffness, strength, and creep with cable constructs compared to monofilament wires of similar diameter. 14,15 The greater flexibility of cable cerclages may more closely adapt to the irregularly shaped bone surface of the patella compared to stainless-steel wires. 16 The decision to trial the titanium cable as opposed to stainless steel wires was manifold. Firstly, based on our experience, the stainless steel wire was found to be pliable but difficult to pass. It was challenging to bend the stainless steel wire continuously for the cerclage, then for the figure-of-eight configuration, and during final tightening. This facilitated the passing and bending of the titanium cable into an ellipsoidal cap structure and allows for more precise control of the cable tension. Secondly, twisting of stainless steel wires to the desired tension may also be highly variable based on surgeon’s experience, with insufficient twisting leading to loosening and overtwisting leading to breakage. 16,17 The precise tightening control afforded by the cable tensioner and crimp in the titanium cable system helps to spread the pressure of cable and avoid excessive pressure concentration such as with wire twisting. 6 This ultimately reduces the risk of cable loosening or breakage during postoperative rehabilitation. 16 Thirdly, the ends of the steel wires are often sharp, especially when the cut occurs at the wire protrusions; however, if the cut is performed at the wire twist, a significant amount of cerclage tension is lost. 6 The subcutaneous location of the wire ends often causes soft tissue irritation. 18 Conversely, the edge of the titanium cable is left blunt with the crimp. Lastly, titanium instrumentation has the advantage of producing minimal magnetic resonance imaging artifact compared to stainless steel wires. 19
There were several limitations to this study, inherent to its retrospective nature. The patient cohort consisted of patients from three surgeons who may have different indications based on the clinical presentation of the patient and slight variations in surgical technique. The size of the case series is small given the rarity of the fracture and the specific type of patellar fracture involved in the study. The patients were followed up for a mean of 2 years; therefore, conclusions regarding long-term clinical and functional outcomes are difficult to extrapolate. We also did not explore the increased cost of the titanium cable system, which may influence surgeons and hospital systems in their choice of implant utilization. Lastly, the study also lacked a control group to which to compare the outcomes of our modified technique.
The modified anterior ellipsoidal cap tension band using a single titanium cable created an effective tension band structure in the treatment of comminuted patella fractures. It is a simple operative technique that produced a stable fixation construct, which allowed early functional rehabilitation and weight-bearing with a high rate of excellent outcomes at 2 years after surgery. Further biomechanical studies are necessary to compare fixation strength in the static and dynamic phases between our one-cable technique and the traditional two-wire technique.
Footnotes
Acknowledgements
We thank Zhonghua Lian, BSc and Yanjie Ye, MSc from Xiamen Medical Device Research & Testing Center for their brilliant illustrations.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Provincial Key Clinical Specialty Construction Program of Fujian (MINWEIKEJIAO [2012]-149), Fujian Medical University Sailing Foundation (2018QH1051) and Natural Science Foundation of Fujian Province (2017J01286).